
Abstract
We present two patients with glioblastoma with an unusually stable clinical course and long-term survival who were treated after surgery and radiotherapy with adjuvant temozolomide (TMZ) chemotherapy for 17 and 20 cycles, respectively. Afterward, adjuvant TMZ chemotherapy was discontinued in one patient and the dosage of TMZ was reduced in the other. In addition to clinical status and magnetic resonance imaging, the biologic activity of the tumors was monitored by repeated methyl-11C-l-methionine (MET) and 3′-deoxy-3′-18F-fluorothymidine (FLT) positron emission tomography (PET) studies in these patients. In these patients, repeated MET-and FLT-PET imaging documented complete response to the initial treatment regimen, including resection, radiation, and TMZ, and during the course of the disease, recurrent, uncontrollable tumor activity. Continuation or dose escalation of TMZ in both patients was shown to be ineffective to overcome the metabolic activity of the tumor. Our data suggest that repeated MET- and FLT-PET imaging provide information on the biologic activity of a tumor that is highly useful to monitor and detect changes in activity.
TEMOZOLOMIDE (TMZ) is an oral, second-generation alkylating agent that was licensed in 1999 for the treatment of patients with malignant glioma showing recurrence or progression after standard therapy. For patients with recurrent malignant glioma, TMZ provides a therapeutic option with a predictable safety profile, clinical efficacy, and convenient dosing, which leads to important quality of life benefits. 1 TMZ is now standard adjuvant therapy in patients with newly diagnosed malignant glioma 2 in combination with radiotherapy.3–5
Owing to systemic adverse effects and possible neurotoxicity, adjuvant chemotherapy for patients with gliomas has not gained universal acceptance yet. 2 However, in a recent randomized controlled trial of radiotherapy alone versus radiotherapy with concomitant and adjuvant TMZ in patients with glioblastoma multiforme (GBM), it was shown that survival was longer for patients who had been assigned combination treatment. 4 At a median follow-up of 28 months, the median survival was 14.6 months with radiotherapy plus TMZ and 12.1 months with radiotherapy alone. The 2-year survival rate was 26.5% with radiotherapy plus TMZ and 10.4% with radiotherapy alone.
Based on these results, current therapy recommendations for patients with GBM are maximal surgical resection followed by radiotherapy plus concomitant and adjuvant chemotherapy with TMZ for 6 to 12 months.4–6 Owing to the poor prognosis for patients with GBM, there are no clear further therapy recommendations for the period after 12 months of adjuvant TMZ chemotherapy. Moreover, if patients respond to adjuvant TMZ, it is unclear how long TMZ should be administered. Imaging of the metabolic activity of tumor tissue in patients with GBM by positron emission tomography (PET) might allow for separation of therapy responders from nonresponders and prove useful for individual therapy decisions.
We present two patients with GBM with unusually stable clinical course and long-term survival who were treated with adjuvant TMZ for more than 12 months. In addition to clinical status and magnetic resonance imaging (MRI), the biologic activity of the tumors was monitored by repeated methyl-11C-l-methionine (MET) and 3′-deoxy-3′-18F-fluorothymidine (FLT) PET studies in these rare individual GBM patients. Additionally, we performed a noninvasive quantification of the FLT-PET data using kinetic modeling for assessment of the proliferative activity of the GBM in one patient.
Methods
PET Studies
MET- and FLT-PET images were acquired on a Siemens ECAT EXACT or ECAT EXACT HR (CTI/Siemens, Knoxville, TN). Ten-minute transmission scans with three rotating 68Ga/68Ge sources were obtained before tracer application to allow for attenuation correction. After injection of 20 mCi (740 MBq) MET, synthesized according to the method of Berger and colleagues, 7 tracer accumulation was recorded in three-dimensional mode over 60 minutes in 47 transaxial slices from the entire brain. Summed activity from 20 to 60 minutes after tracer injection was used for image reconstruction. FLT was synthesized according to the modified method of Machulla and colleagues8, 9 and 10 mCi (370 MBq) was injected. FLT-PET images were acquired as a 90-minute dynamic set (6 × 10, 3 × 20, 2 × 30, 2 × 60, 2 × 150, 16 × 300 seconds) as described previously. 10 Images were reconstructed with Fourier rebinning and filtered backprojection with a ramp filter. Images were corrected for scatter, attenuation, and random coincidences. Spatial resolution was 6 mm or better in all dimensions.
For data assessment, uptake ratios in MET- and FLT-PET images were determined as previously described.10, 11 In brief, a circular region of interest (ROI) of 8 mm in diameter was placed over the tumor area and normalized to a reference ROI placed over intact brain tissue in the corresponding contralateral region or, if impossible because of the tumor location, on intact brain regions.
As described previously, kinetic modeling of FLT-PET data using image-derived input functions was performed 12 and kinetic rate constants K1 (transport across the blood-brain barrier) and Ki (metabolic rate constant or net influx constant) were calculated. Values of K1 and Ki were presented in mL/cm3/min ± standard deviation.
Results
Case Presentations
Patient 1
A 37-year-old patient noticed weakness of the left arm and leg 4 weeks prior to admission in May 2001. Neurologic findings on admission were consistent with a slight hemiparesis of the left side. MRI showed a contrast-enhancing, tumor-suspicious lesion in the right frontal lobe. Neurosurgical resection was performed, and histopathologic examination of the lesion in June 2001 revealed a GBM World Health Organization (WHO) grade 4 (Figure 1). After resection, external radiation therapy was initiated. Owing to persistent gadolinium enhancement in MRI after a total radiation dose of 42 Gy, the external radiation therapy was terminated and a further neurosurgical intervention was performed in August 2001. Afterward, the first cycle of TMZ chemotherapy was initiated in September 2001. The dosage was 200 mg/m2 body surface per day for 5 days, and the cycles were repeated every 4 weeks. After 17 cycles of TMZ and stable clinical status without recurrence of the GBM as assessed by MET-PET (Figure 2), it was decided to discontinue TMZ therapy in May 2003.
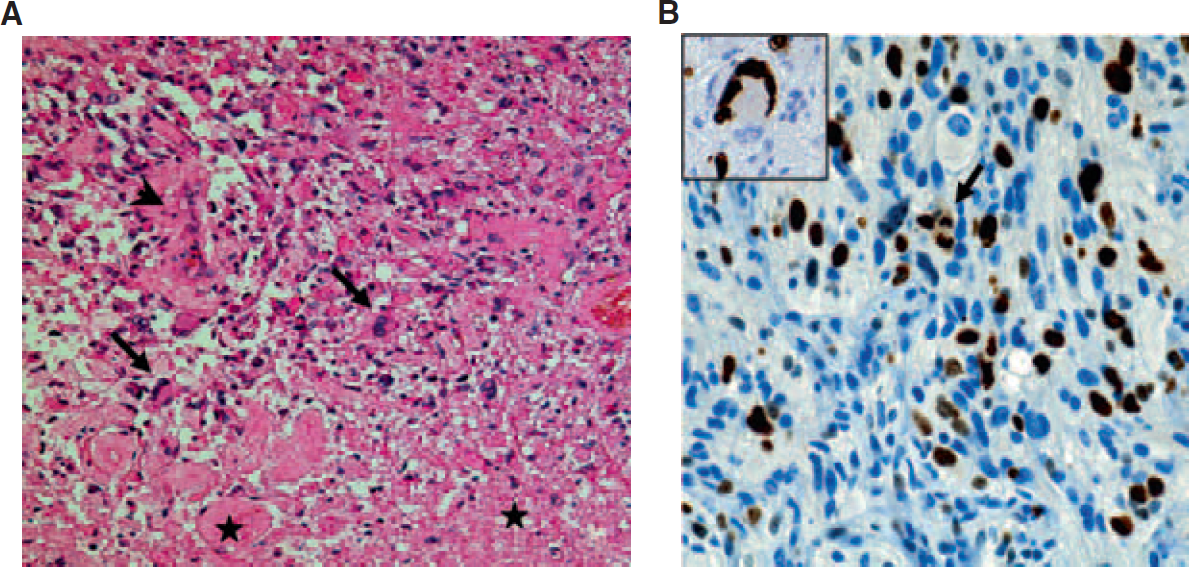
Glioblastoma multiforme (WHO grade 4), patient 1. A, An anaplastic cellular glioma composed of pleomorphic astrocytic tumor cells with marked nuclear atypia and increased mitotic activity. Single giant cells (arrows), microvascular proliferation (arrowhead), and necrosis (asterisks) (hematoxylin-eosin staining; ×200 original magnification). B, Proliferative activity is brisk and includes giant cells (insert). Arrow indicates a mitotic figure (MIB-1 immunohistochemistry, slight counterstaining with hemalum; ×400 original magnification).

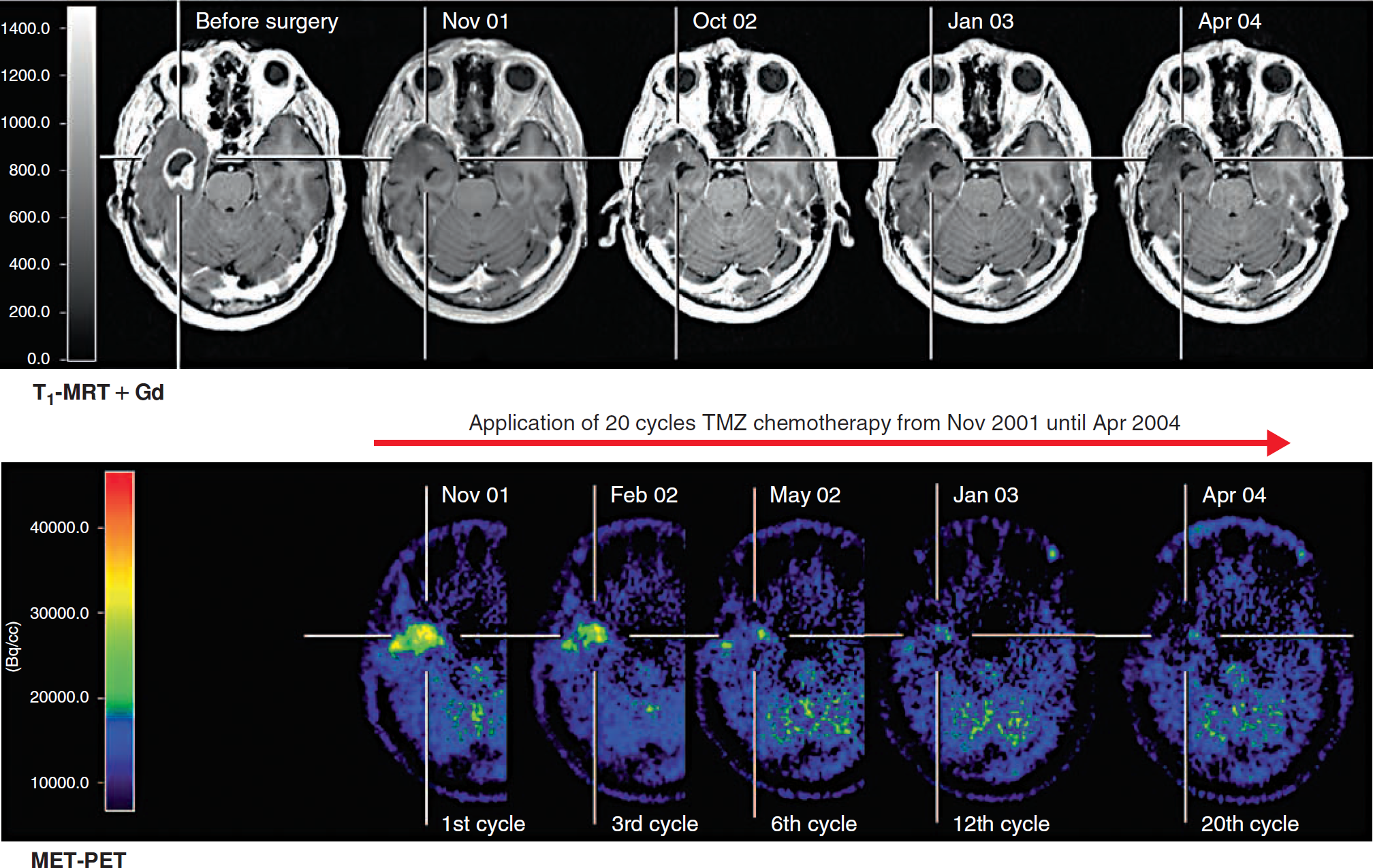
Patient 1 with a right frontal glioblastoma WHO grade 4. MET amino acid uptake was unchanged during the course of TMZ chemotherapy after resections and radiotherapy. After 17 cycles, the TMZ chemotherapy was discontinued (arrow). Six months later, the metabolic activity of the tumor as measured by MET-PET increased again and was not affected by restart of TMZ chemotherapy.
Six months after discontinuation of TMZ, a follow-up MET-PET showed recurrence of metabolically active tumor mass lateral to the resection defect without clinical symptoms (see Figure 2). The MET uptake was increased 1.8-fold in comparison to the unaffected contralateral brain tissue. 11 TMZ chemotherapy was initiated again at the standard dosage of 200 mg/m2 body surface per day over 5 days. A further follow-up MET-PET was performed 3 months later and showed similar uptake but an increased size of the MET uptake pattern (see Figure 2). The corresponding MRI was consistent with a recurrence of GBM and showed a positive contrast enhancement (see Figure 2). The patient was still free from clinical symptoms, but 1 month later, the first epileptic seizure occurred. During the course of the disease, the frequency of epileptic seizures increased up to daily seizures. Owing to clinical deterioration and imaging-based tumor progression, TMZ chemotherapy was discontinued. The patient died 8 months after the last MET-PET in October 2004.
Patient 2
A 53-year-old patient developed headache, weight loss, dizziness, and night sweats 2 months prior to admission in June 2001. Neurologic examination on admission showed no relevant deficit. MRI revealed a contrast–enhancing, tumor-suspicious, polycystic lesion in the right temporal lobe (Figure 3), which was resected in August 2001. Histopathologic findings confirmed a GBM WHO grade 4 (Figure 4, A–C). After resection, external radiation therapy up to a total dose of 60 Gy with concomitant TMZ chemotherapy (75 mg/m2 body surface per radiation course) was initiated. Subsequently, the first cycle of adjuvant TMZ chemotherapy was performed in November 2001 at a dosage of 200 mg/m2 body surface per day over 5 days, with cycles being repeated every 4 weeks (see Figure 3). After 20 cycles of TMZ and stable clinical status without recurrence in the right temporal lobe of the GBM as assessed by MRI and MET-PET (see Figure 3), TMZ cycles were repeated at 10-week intervals starting from April 2004 (Figure 5; arrow).
Effect of adjuvant TMZ therapy in patient 2 with a right temporal glioblastoma WHO grade 4 after resection and radiotherapy. MET uptake decreased during 20 cycles of TMZ chemotherapy. Increased gadolinium enhancement was not observed in MRI.

Glioblastoma multiforme (WHO grade 4), patient 2. A, An anaplastic cellular glioma composed of small astrocytic tumor cells, geographic necrosis, and large, thrombosed tumor vessels (asterisks) (hematoxylin-eosin stain; ×200 original magnification). B, Note the prominent microvascular proliferation with multilayered “glomeruloid tuft” glioma vessels (hematoxylin-eosin stain; ×400 original magnification). C, Proliferative activity is prominent (MIB-1 immunohistochemistry, slight counterstaining with hemalum; ×400 original magnification). D, The recurrency is composed predominantly of small astrocytic tumor cells with a prominent network of pathologic vessels (hematoxylin-eosin stain; ×200 original magnification). E, Marked nuclear atypia with multinucleated tumor cells (arrows) (hematoxylin-eosin stain; ×400 original magnification). F, Brisk proliferative activity (MIB-1 immunohistochemistry, slight counterstaining with hemalum; ×400 original magnification).
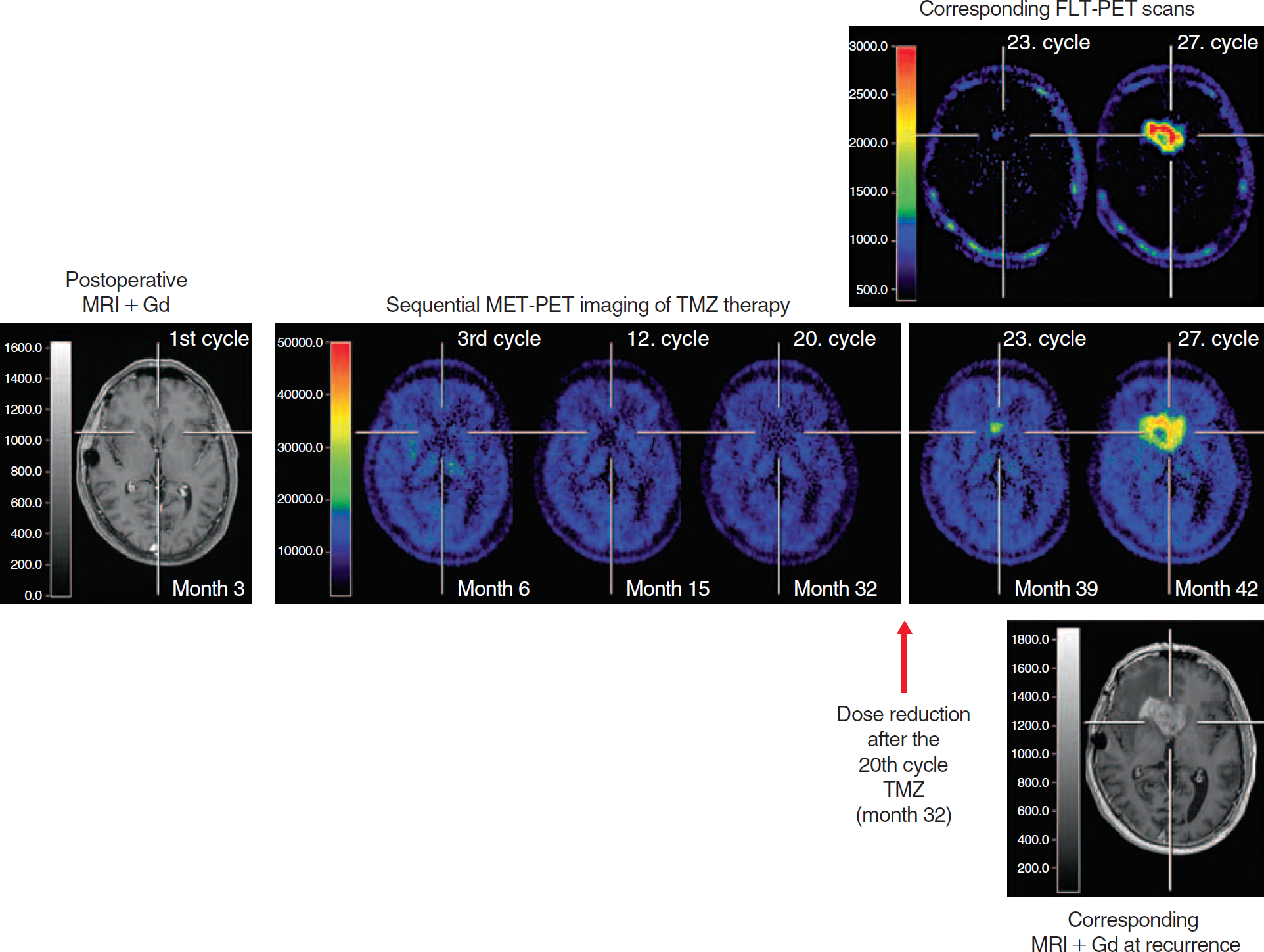
After 20 cycles of TMZ, a dose reduction by repeating the cycles every 10 weeks was performed in patient 2 (arrow). Seven months later, increased metabolic activity as measured by MET- and FLT-PET was observed at the right anterior part of the corpus callosum without contact to the primary tumor localization. Restart of dose-escalated TMZ chemotherapy did not have an effect on metabolic activity of the recurrent tumor tissue.
FLT- and MET-PET imaging 7 months after dose reduction of TMZ showed a new, small, metabolically active tumor mass at the right anterior part of the corpus callosum without contact to the primary tumor localization (see Figure 5). The MET uptake ratio was 1.9-fold increased in comparison to the unaffected contralateral brain tissue, and the FLT uptake ratio was 2.6-fold increased. Kinetic modeling of the FLT data revealed a K1 value of 0.004874 mL/cm3/min ± 0.0029 and a Ki value of 0.001517 mL/cm3/min ± 0.0021, respectively. TMZ chemotherapy was escalated according to a 1-week on/1-week off regimen. 13 The follow-up PET imaging 3 months after therapy escalation showed a MET uptake pattern at the right anterior part of the corpus callosum with a massive increase in size and uptake ratio to 3.4-fold (see Figure 5). In comparison with MET-PET, the FLT-PET showed as well a similar same-sized lesion but a higher FLT-uptake ratio (7.5-fold; see Figure 5). Kinetic modeling of this FLT-PET scan revealed a dramatic 18-fold increased value of Ki (0.027383 mL/cm3/min ± 0.0101) and a 25-fold increased K1 value (0.119845 mL/cm3/min ± 0.0089). The corresponding MRI was consistent with a recurrence of GBM and showed a positive contrast enhancement (see Figure 5). After maximal resection of the recurrent GBM (Figure 4, D–F), the patient died 6 months later after having received palliative care.
Discussion
We present two patients with GBM with a stable clinical course while on long-term adjuvant TMZ chemotherapy who both relapsed after discontinuation or reduction of TMZ. In these patients, repeated MET-PET imaging combined with two additional serial FLT-PET scans including kinetic modeling in one patient documented a complete response to the initial treatment regimen, including resection, radiation, and TMZ, and during the course of the disease, recurrent, uncontrollable tumor activity. Treatment decisions (decision against discontinuation of adjuvant TMZ chemotherapy when PET findings show no increased metabolic activity as well as the continuation or dose escalation of TMZ in both patients at the time of recurrence) were significantly supported by the findings of the metabolic PET images.
Once the tumors had relapsed, continuation or dose escalation of TMZ in both patients was shown to be ineffective in overcoming the metabolic activity of the tumor. A possible hypothesis for TMZ ineffectiveness might be an accelerated mutagenic process in resistant clones as a consequence of continued exposure to alkylating agents. Recent evidence suggests that the mismatch repair gene MSH6 in gliomas is inactivated owing to mutations. In consequence, alkylating agents convert from their function to induce tumor cell death to the promotion of neoplastic progression. 14
In clinical routine, long-term adjuvant TMZ chemotherapy in patients with malignant gliomas with respect to possible short- and long-term complications is being monitored clinically and by MRI studies. Metabolic tracers, such as positron emitter–labeled amino acids, have been proposed as new indicators of tumor activity. 15 A previous study revealed that monitoring of metabolic changes with MET-PET may provide an objective measure for response to TMZ treatment; thus, it should be integrated as an improved imaging modality to monitor biologic tumor activity. 16 MET-PET may be a valuable method to differentiate therapy responders from nonresponders and may provide important information for making treatment decisions, especially in nonresponders. MET-PET has been used to study the effects of radiotherapy in gliomas.17–20 It provides a more accurate assessment of tumor extent than contrast enhancement on computed tomography and MRI.21–24 Accumulation is largely due to carrier-mediated transport, which is not altered by dexamethasone 21 and also permits the alternative method of perfusion MRI distinction between tumors and contrast-enhancing necrosis.25–27 MET undergoes complex metabolism and is incorporated into proteins; therefore, increased uptake may reflect the metabolic needs of brain tumors. 28 The effect of chemotherapy with procarbazine, lomustine, and vincristine in an anaplastic oligoastrocytoma was monitored by repeated MET-PET 29 successfully and highlighted the potential of this technique to monitor chemotherapy. Most importantly, MET-PET may allow the prediction of clinical outcome in patients with gliomas within 3 months after onset of chemotherapy, 16 which makes it a valuable addition to conventional MRI.
In comparison with the imaging modalities MET-PET and gadolinium-enhanced MRI, FLT-PET was recently characterized in a heterogeneous glioma patient collective and seems to yield additional information on the activity and extent of gliomas. 10 Furthermore, FLT-PET can be used to evaluate the proliferative activity of primary brain tumors and to detect recurrent gliomas, especially malignant brain tumors.30–33 Relative FLT uptake within gliomas is greater than relative MET uptake, 10 indicating the possible role of FLT as a more specific tumor marker than [18F]-labeled fluorodeoxyglucose32, 34 and MET,35, 36 especially when kinetic modeling is used for assessment of tumor proliferation as a marker for the real biologic activity in patients with newly diagnosed high-grade glioma. 37 In the second patient presented here, the recurrent tumor tissue was detected by both FLT-PET including kinetic modeling and MET-PET.
Our data suggest that repeated MET- and FLT-PET imaging including kinetic modeling provide information on the biologic activity of a tumor that is highly useful to monitor and detect changes in activity. The observation that the metabolic changes occurred after discontinuation and dose reduction of adjuvant TMZ chemotherapy needs further exploration of whether TMZ should be given in patients with GBMs even when they do not show any active tumor.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.