
Abstract
To assess positron emission tomography (PET) with fluorine-18 fluorocholine for sextant localization of malignant prostate tumors. Histopathologic analysis was performed on step-sectioned whole-mounted prostate specimens from 15 patients who underwent PET with fluorocholine prior to radical prostatectomy. The maximum standardized uptake value (SUVmax) corresponding to prostate sextants on PET was measured by region of interest analysis and compared with histopathologic results. Histopathology demonstrated malignant involvement in 61 of 90 prostate sextants. The mean total tumor volume per specimen was 4.9 mL (range 0.01–28.7 mL). Mean SUVmax was 6.0 ± 2.0 in malignant sextants and 3.8 ± 1.4 in benign sextants (p < .0001). The area under the receiver operating characteristic curve was 0.82 for sextant detection of malignancy based on SUVmax measurement. Tumor diameter directly correlated with sextant SUVmax in malignant sextants (r = .54, p < .05). In 13 subjects, the largest tumor in the specimen corresponded to the sextant with the highest SUVmax. Fluorocholine PET can serve to localize dominant areas of malignancy in patients with prostate cancer. However, PET with fluorocholine may fail to identify sextants with smaller volumes of malignancy.
PROSTATE CANCER is the second leading cause of cancer death in American men over 50 years of age. The diagnosis of prostate cancer is typically obtained after transrectal ultrasound-guided prostate biopsy. However, this method of diagnosis is prone to sampling error; consequently, a large number of clinically significant prostate cancers are missed at the initial biopsy.1–5 Although advancements have been made at alternatively detecting primary prostate cancer with ultrasonography or magnetic resonance imaging (MRI), not all of the clinical and technical hurdles associated with these techniques have been overcome.6–8
Positron emission tomography (PET) offers an alternative approach for detecting tumors through noninvasive measurement of metabolic changes at the cellular level. This technique works by depicting the biochemical interactions of radiolabeled tracers in vivo. Fluorine-18 (18F)-labeled fluorocholine is a synthetic derivative of choline that is being investigated as a potential tumor imaging agent for PET. The phosphorylation of fluorocholine by choline kinase, an enzyme commonly overexpressed in malignancy, is responsible for the intracellular trapping of this compound. 9 The observation that there is increased choline metabolism in malignant prostate tissue relative to normal tissue supports the possibility of using fluorocholine PET to visualize cancer in the prostate gland.10,11
The objective of this histopathologic correlation study was to preliminarily evaluate PET with 18F-fluorocholine for sextant-level localization of malignancy in the prostate gland. The definition of prostate sextants is based on the prostate biopsy convention in which the prostate gland is divided into basal, mid-, and apical portions on each side.4,7,12–14 PET scanning with fluorocholine was performed prospectively in subjects with organ-confined prostate cancer who subsequently underwent radical prostatectomy. Step-sectioning of completely embedded prostate specimens was used to obtain the diagnostic standard of reference for this study.
Materials and Methods
Human subjects research approval for this study was obtained from the participating hospitals' institutional review board and the Department of the Defense Human Subjects Research and Review Board. To meet inclusion criteria for the study, subjects had to have clinically organ-confined prostate cancer (stage II) for which radical prostatectomy was elected as primary treatment. Written informed consent was obtained from all subjects prior to their involvement with the study.
Radioactive Tracer Synthesis
Synthesis of 18F-fluorocholine was performed by fluorination of ditosylmethane with fluorine-18 followed by alkylation of fluorotosylmethane with dimethylethanolamine. The synthesis procedure was automated and performed at an on-site cyclotron laboratory using a computer-controlled chemical process control unit (CTI/Siemens CPCU, CTI/Siemens, Knoxville, TN). 15 All synthesis products passed standard assays for radiochemical purity, radionuclidic identity, chemical purity, sterility, and pyrogenicity in compliance with US Pharmacopia Good Clinical Practice guidelines.
Imaging
PET was performed in the supine position after a 3-hour fast. All PET scans were obtained with a 32-ring whole-body PET scanning instrument (SHR-22000, Hamamatsu Photonics KK, Hamamatsu City, Japan). Whole-body transmission scans were first acquired using two germanium 68 rod sources over five fields of view (FOV) for 3 minutes each. After transmission scanning, 3.3 to 4 Mbq/kg of 18F-fluorocholine was administered through an antecubital vein. After a 10-minute delay, two-dimensional emission scans were acquired for 7 minutes over each FOV. Imaging proceeded in a cephalad direction starting at the pelvis. The PET images were reconstructed using an ordered subsets expectation maximization algorithm. Segmented attenuation correction was applied to the emission data using the measured transmission data. Reconstruction resulted in 4 mm × 4 mm × 3.6 mm voxels. Images were viewed and analyzed on a workstation using PET image analysis software (Medasys Data Systems, Gif-sur-Yvette Cedex, France).
Immediately following PET, computed tomography (CT) of the pelvis (slice thickness 3.2 mm, reconstruction interval 2.0 mm) was performed without intravenous contrast using a conventional CT scanner (four-slice CT, Philips Medical Systems, Shelton, CT). The CT images were spatially registered to the PET images using commercial software (HERMES, Hermes Medical Solutions, Battle Ground, WA). Images were reviewed and analyzed on computer workstations.
Image Analysis
Image analysis was performed by two independent readers with PET imaging experience (S.A.K., M.N.C.). The readers were blinded to the histopathology results at the time of the initial reading, although it was known that all subjects were diagnosed with prostate cancer. Analysis began with visual inspection of CT-registered PET images to identify the prostate. The prostate can be identified on fluorocholine PET images as a discrete region of uptake located inferior and slightly posterior to the urinary bladder (Figure 1). Measurement of uptake in prostate sextants was performed as follows: prostate volumes on CT-registered PET images were manually segmented into sextants consisting of an upper (basal) one-third, middle one-third, and lower (apical) one-third portion of the gland on each side. Using region of interest analysis, the maximum standardized uptake value (SUVmax) corresponding to prostate sextants on each image slice was measured and the SUVmax of each sextant was recorded. SUVmax was defined as the maximum measured activity divided by the injected radioactivity normalized to body weight. The individual readers obtained concordant sextant SUVmax measurements in all subjects.

Transverse axial fluorocholine positron emission tomographic images of the prostate. In this example, a malignant tumor demonstrates increased fluorocholine uptake from the base to the apex of the prostate (long arrows point to malignant prostate sextants). Urinary excretion of fluorocholine is evident in the urinary bladder (large arrowhead) but did not interfere with prostate visualization.
Prostate Specimen Analysis
After surgery, the prostate specimens were placed in a 10% formalin solution for 3 days. Histologic processing of the prostate specimen was then performed by the step-section technique. Completely embedded whole-prostate specimens were sectioned at regular 2.2 mm intervals. Thin slices from each section were mounted on large glass slides and stained with hemotoxylin and eosin. Areas of malignant tumor on each slide were manually segmented and assigned to their corresponding sextant by a single pathologist with extensive experience in genitourinary pathology (I.A.S.). Each slide was photographed to scale using a digital camera mounted on a stage (Figure 2). The size, Gleason scoring, and sextant location of all malignant tumors were recorded for each specimen.

Left, Micrograph (×10) of a prostate specimen containing multiple malignant tumors (outlined in black). The largest malignant tumor is located in the anterior right base (black arrow). It measures 1 cm in largest diameter. Right, The corresponding transverse axial computed tomography-fused positron emission tomographic (PET) image of the pelvis demonstrates highest fluorocholine uptake (white arrow) in the area to the largest malignant tumor found by histopathology. Smaller malignant tumors in the specimen were not distinctly evident on fluorocholine PET.
Analysis and Statistical Considerations
Statistical analysis was performed at the prostate sextant level, with histopathologic findings serving to determine the presence or absence of malignancy in each sextant. Sextants were classified as malignant if they contained a portion of at least one malignant tumor regardless of its size. Statistics included sensitivity and specificity for sextant diagnosis using various SUVmax thresholds for defining malignancy in prostate sextants based on receiver operating characteristic (ROC) analysis. Differences in sample means were tested for significance using the Student t-test. The linear relationship between two variables was assessed using the Pearson correlation coefficient. Statistical analysis was performed using JMP version 5 (SAS Institute Inc., Cary, NC). All tests were two-sided, and p values < .05 were considered significant.
Results
Subject Characteristics
Fifteen subjects underwent preoperative fluorocholine PET with whole-prostate histopathologic analysis of their specimens after surgery. Individual subject characteristics are summarized in Table 1. The average age of the subjects was 62 years (range 47–71 years). The median serum prostate-specific antigen (PSA) level was 5.1 ng/mL (range 3.5–13.8 ng/mL). The mean weight of prostate specimens was 50 g (range 13–106 g). Multifocal prostate cancer was found in 13 subjects and unifocal prostate cancer in 2 subjects. Benign prostatic hyperplasia or prostatitis was evident in every prostate examined. Sixty-one of 90 prostate sextants were found to harbor malignant tumors on histopathologic analysis. The median number of malignantly involved sextants was 4 (range 2–6). The mean total tumor volume per specimen was 4.9 mL (range 0.01–28.8 mL). The median Gleason sum score was 6 (range 6–9).
Characteristics of 15 Subjects Who Underwent Fluorocholine Positron Emission Tomography Prior to Radical Prostatectomy with Whole-Mount Histopathologic Analysis of Their Prostate Specimens
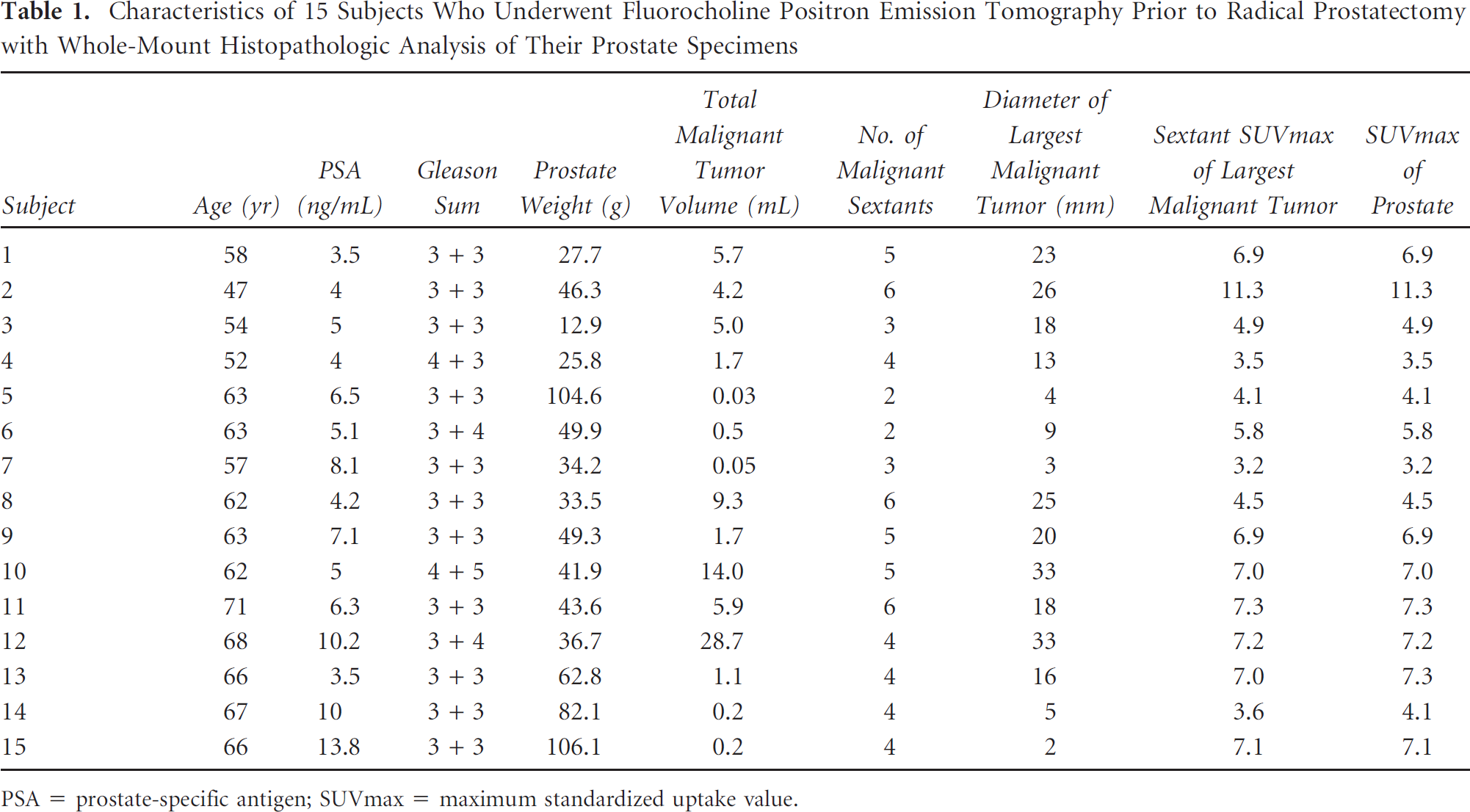
PSA = prostate-specific antigen; SUVmax = maximum standardized uptake value.
PET Images
The SUVmax of the prostate and the SUVmax of the sextant containing the largest tumor for each subject is listed in Table 1. The mean SUVmax of malignant sextants was significantly higher than the mean SUVmax of benign sextants (6.0 ± 2.0 vs 3.8 ± 1.4, respectively; p < .0001). The area under the ROC curve was 0.82 for fluorocholine PET detection of malignant prostate sextants (Figure 3). The highest diagnostic accuracy was achieved using a sextant SUVmax of 5.6 or higher to classify a sextant as malignant. At this point of the ROC curve, accuracy, sensitivity, and specificity were 72%, 64%, and 90%, respectively. With lower SUVmax threshholds, sensitivity can be increased at the cost of specificity. For example, sensitivity and specificity were 85% and 62%, respectively, using a SUVmax threshold of 4.0

Receiver operating characteristic curve for fluorocholine positron emission tomographic diagnosis of malignant prostate sextants (regardless of tumor size). Area under the curve = 0.82.
In all subjects, the highest SUVmax of the prostate was localized to a malignant sextant (Table 2). In 13 of 15 subjects, the sextant with the highest SUVmax was also the sextant containing the largest tumor of that specimen. There was a statistically significant correlation between maximum tumor diameter and SUVmax in malignant sextants (Pearson correlation coefficient r = .54, p < .05) (Figure 4). There were no significant correlations between highest SUVmax in the prostate, subject's age, serum PSA, and Gleason sum score.
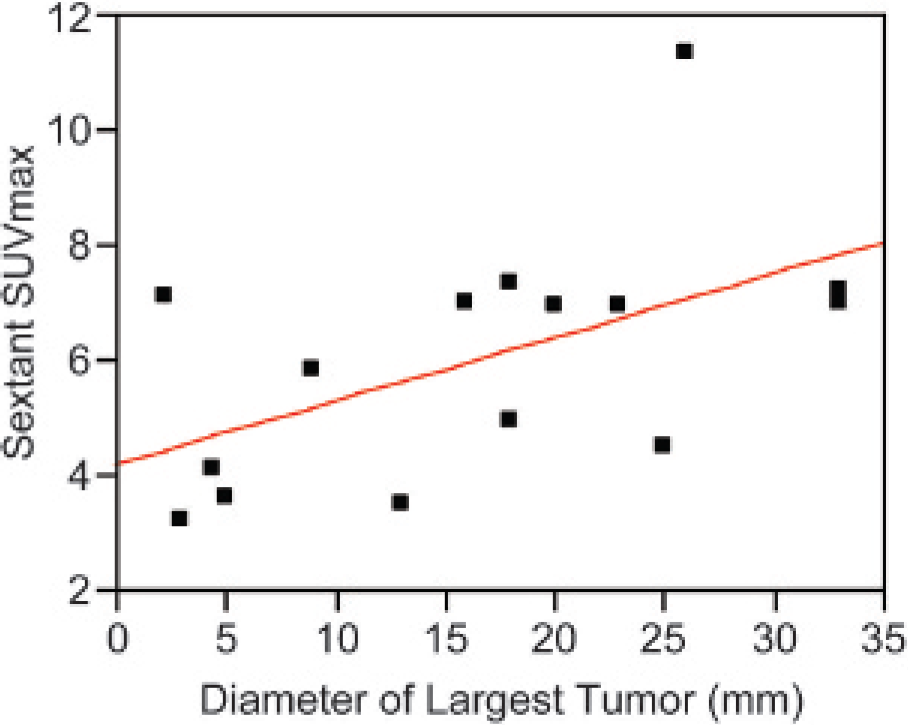
Sextant maximum standardized uptake value (SUVmax) as a function of largest tumor diameter in malignant sextants.
Sextant Malignancy and Maximum Standardized Uptake Value
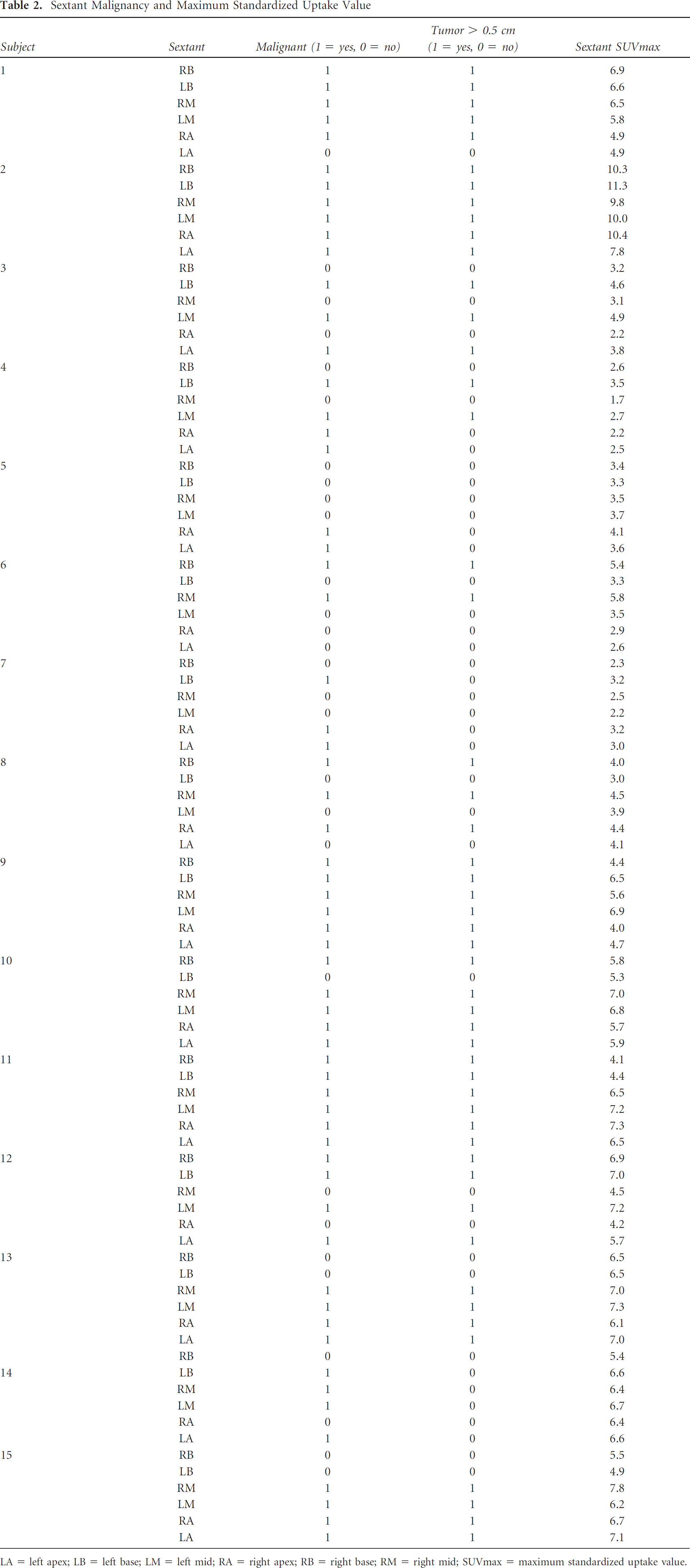
LA = left apex; LB = left base; LM = left mid; RA = right apex; RB = right base; RM = right mid; SUVmax = maximum standardized uptake value.
Discussion
The prostate gland is a challenging organ to image with nuclear techniques because of its anatomic location and small size relative to the spatial resolution of most nuclear imaging devices. The spatial resolution of PET is influenced not only by detector design and reconstruction method but also by the physical effects of radioactive scatter and positron travel. 16 Because of these factors, there is spillover of radioactive signals from small sources, which leads to larger but dimmer sources on the final reconstructed PET image. The finding of a correlation between the SUVmax of malignant sextants and tumor size in this study is attributable in part to the limited spatial resolution of current PET instrumentation.
For very small tumors, there is also a partial volume effect owing to the fact that SUV is a reflection of the average radioactivity concentration in a volume of tissue that corresponds to an image voxel. 17 Assuming that fluorocholine is concentrated by malignant cells, the measured SUV of a voxel-sized volume containing both malignant and benign cells should be lower than the measured SUV of the same volume of tissue containing only malignant cells. Despite this limitation in quantitative assessment with SUVmax, the measurement of sextant SUVmax on fluorocholine PET provided a degree of accuracy that was comparable to that of endorectal MRI, magnetic resonance spectroscopy, and carbon 11 choline PET for sextant-level detection of prostate cancer.7,18–20 Given that prognosis in prostate cancer may be related to tumor size,21,22 a lower sensitivity for small malignant lesions may be acceptable in the appropriate clinical context.
The relatively small tumor volumes found in those enrolled in this study were not surprising since the majority of subjects were from a young military population that has undergone periodic screening for prostate cancer. The fact that fluorocholine PET has performed reasonably well in this group of lower-risk patients is encouraging. In this study, the sextant with the highest SUVmax was consistently malignant and often corresponded to the site of highest tumor volume in the specimen. These findings support the possibility of using fluorocholine PET as an imaging adjunct for directing prostate biopsies (to the areas of highest malignant potential) or for assisting with prostate radiation therapy planning (with the goal of delivering higher radiation doses to the densest areas of malignancy).
The use of SUVmax in this study provided a reproducible, objective measure for classifying the prostate sextant. However, when objective threshold values are applied to produce a dichotomous result, there is usually a trade-off between diagnostic sensitivity and specificity that is a function of the threshold value. 23 Although an SUVmax threshold of 5.6 resulted in the highest overall accuracy in this study, certain clinical applications, such as prostate biopsy, may benefit from a higher sensitivity achieved through using a lower SUVmax threshold. Appropriate SUVmax thresholds should be selected based on clinical requirements.
A previous study evaluating prostate PET/CT with fluorocholine reported no significant difference in fluorocholine uptake between malignant and benign prostate lesions. 24 However, there were differences in imaging technique between this and the current study. In particular, prostate imaging in this previous study was begun at 2 minutes postinjection of fluorocholine, whereas in the present study, imaging was begun at 10 minutes postinjection. Although tissue uptake of fluorocholine is indeed rapid, a 2-minute delay before imaging may not have been sufficient to allow visualization of malignant prostate tumors.9,25 In a previous study, we also observed the ratio of fluorocholine uptake between malignant and benign areas of the prostate to increase significantly over the interval of 10 minutes to 1 hour postinjection. 26 Further study is needed to determine the optimal fluorocholine PET scan protocol for evaluating prostate tumors.
With delayed imaging, there is an increase in the amount of bladder radioactivity encountered. This is the result of urinary excretion of fluorocholine or its metabolites. Although the effects of urinary bladder activity on prostate image interpretation have not been studied specifically, it is conceivable that radioactive scatter from the bladder can lead to both false-positive and false-negative results. If bladder radioactivity can be reduced, it may be possible to improve the overall diagnostic accuracy of fluorocholine PET for prostate tumor diagnosis. Dynamic imaging and protocols to minimize urinary bladder radioactivity may be useful in future PET-computed tomographic (CT) studies to further optimize fluorocholine PET for prostate imaging.
The results of this study should be considered in light of several limitations. First, the accuracy of fluorocholine PET was assessed only in patients with known prostate cancer. Therefore, the results of this study cannot be applied to patients who are only suspected of having cancer. For example, the utility of fluorocholine PET in patients with elevated PSA levels and negative initial prostate biopsies requires specific study. Furthermore, the sextant assignment of malignant tumors on histopathology and the measurement of sextant SUVmax were performed by different individuals. Although this ensures independence between the diagnostic test and gold standard interpretations, there is the possibility that sextants defined on PET may not correspond precisely to sextants defined on the specimen. However, the effects of any potential sextant mismatch are likely small given that sextants correspond to relatively large nonanatomic regions of the prostate. Finally, this study was conducted using a conventional stand-alone PET scanner. Newer technologies such as time-of-flight scanning, list-mode data acquisition, and PET-CT have been introduced that may enable more detailed subsextant, per-sextant, or per-lesion evaluation of the prostate with fluorocholine. By increasing the count-rate performance of PET, time-of-flight may particularly improve the quality of prostate images, especially in larger patients. 27 PET-CT should enable more accurate anatomic localization of fluorocholine accumulation in the prostate compared with stand-alone PET. These new technologies should be beneficial for future prostate cancer localization studies using fluorocholine.
Conclusion
This histopathologic correlation study in patients with relatively low tumor burdens supports fluorocholine PET as an imaging technique for delineating prostate sextants with malignant involvement. Although there was lower sensitivity for sextants with small tumor burdens, this technique does appear capable of localizing dominant malignant regions in the prostate and thus may have value for specific clinical applications such as targeted prostate biopsy or prostate radiation therapy dose augmentation.