
Abstract
Among female-specific cancers worldwide, ovarian cancer is the leading cause of death from gynecologic malignancy in the western world. Despite radical surgery and initial high response rates to first-line chemotherapy, up to 70% of patients experience relapses with a median progression-free survival of 12–18 months. There remains an urgent need for novel targeted therapies to improve clinical outcomes in ovarian cancer. This review aims to assess current understanding of targeted therapy in ovarian cancer and evaluate the evidence for targeting growth-dependent mechanisms involved in its pathogenesis. Of the many targeted therapies currently under evaluation, the most promising strategies developed thus far are antiangiogenic agents and PARP inhibitors.
Among female-specific cancers worldwide, ovarian cancer is the leading cause of death from gynecologic malignancy in the western world [1]. It is estimated that 14,180 deaths from this disease will occur this year out of 21,290 women diagnosed, with a 5-year survival rate of approximately 30% in advanced-stage disease [2]. The current standard of care for ovarian cancer is a combination of optimal cytoreductive surgery and platinum-based chemotherapy with the carboplatin—paclitaxel regimen [3]. Despite radical surgery and initial high response rates to first-line chemotherapy, up to 70% of patients experience relapses with a median progression-free survival of 12–18 months [4]. Sensitivity to platinum-based chemotherapies also decreases with each subsequent relapse with the development of platinum-resistant and refractory disease [5]. As such, the long-term survival remains poor, with a high risk of recurrence. Furthermore, chemotherapeutic regimens for treatment of ovarian cancer adversely impact quality of life due to side effects, such as neurotoxicity, arthralgia and fatigue [6]. There remains an urgent need to establish novel targeted therapies and their routes of administration to improve clinical outcomes and tolerability in ovarian cancer treatment. In an age when great advances have been made in understanding the genetics and molecular biology of this heterogeneous disease, the introduction of novel targeted therapies will have a major impact on ovarian cancer management. Several are in the early stages of development, while other targeted agents have been examined in first-line therapy of ovarian cancer in clinical trials. These targets include VEGFR- and EGFR-signaling cascades [7,8]. Moreover, alternative routes of treatment have been proposed, such as intraperitoneal chemotherapy and nanotechnology-based therapy, which have shown promising results in early clinical trials [9,10]. The standard platinum-based treatment of ovarian cancer is evolving as intraperitoneal (ip.) chemotherapy has shown to be superior to intravenous (iv.) chemotherapy following optimal debulking surgery [11]. The aim of this review is to assess current understanding of targeted therapy in ovarian cancer, and evaluate the evidence for interfering with growth-dependent mechanisms involved in its pathogenesis. Targeted therapy directed at pertinent cancer cell growth and survival pathways will first be explored, singly and in combination with other anticancer and chemotherapeutic agents. The strengths and weaknesses of the evidence will be evaluated. Lastly, a summary of key findings will be made to identify possible changes in clinical care arising from findings of current studies.
Targeted therapeutic options in ovarian cancer
As a result of a greater understanding of molecular pathways involved in carcinogenesis and tumor growth, the following potential therapeutic targets have been identified for ovarian cancer; anti-VEGF/VEGFR angiogenic inhibitors, non-VEGF angiogenic inhibitors, PARP inhibitors, EGFR inhibitors, folate receptor inhibitor, IGFR inhibitors.
Anti-VEGF/VEGFR angiogenic inhibitors
Two primary strategies have been used to inhibit the VEGFR-signaling pathway, namely inhibition of the ligand (VEGF) with antibodies or soluble receptors, and inhibition of the receptor with tyrosine kinase inhibitors [12,13]. Of the VEGF targeting therapies, the most thoroughly investigated molecular targeted drug in ovarian cancer is bevacizumab. Bevacizumab is a recombinant monoclonal anti-VEGF antibody [14]. Several Phase II studies have shown bevacizumab is active in recurrent ovarian cancer and may be used singly or in combination with chemotherapy (Table 1). Currently, antiangiogenic agents are moving from Phase II to III clinical trials in ovarian cancer. The GOG-218 trial investigated the addition of bevacizumab every 3 weeks to standard three weekly carboplatin and paclitaxel in a randomized three-arm placebo controlled study [15]. The trial enrolled 1873 patients with stage 3–4 ovarian cancer who had residual disease following primary debulking surgery. In the two experimental arms, bevacizumab was given with chemotherapy and subsequently continued as maintenance treatment, while in the other arm, patients switched to placebo after chemotherapy. A substantial benefit in progression-free survival (PFS) was seen in the bevacizumab maintenance arm compared with the control arm at 10.3 and 14.1 months, respectively. A second Phase III trial (ICON-7) in 1528 high-risk early-stage or advanced ovarian cancer patients similarly examined addition of bevacizumab to standard carboplatin and paclitaxel followed by maintenance bevacizumab until disease progression [16]. The PFS at 36 months was substantially greater in patients receiving bevacizumab. Furthermore, an updated analysis of high-risk patients (stage 3 or 4 with >1 cm residual disease) at 42 months demonstrated a greater extent of benefit at 14.5 months for standard therapy in comparison with 18.1 months with combination treatment. In both trials, addition of bevacizumab was well-tolerated. Grade ≥2 hypertension (symptomatic increase by >20 mmHg (diastolic) or to >150/100) was observed in 16.5 and 22.9% in the two bevacizumab arms compared with 7.2% in the control arm. The incidence of other adverse effects such as gastrointestinal perforation and proteinuria was infrequent.
Anti-VEGF angiogenic inhibitors in ovarian cancer.
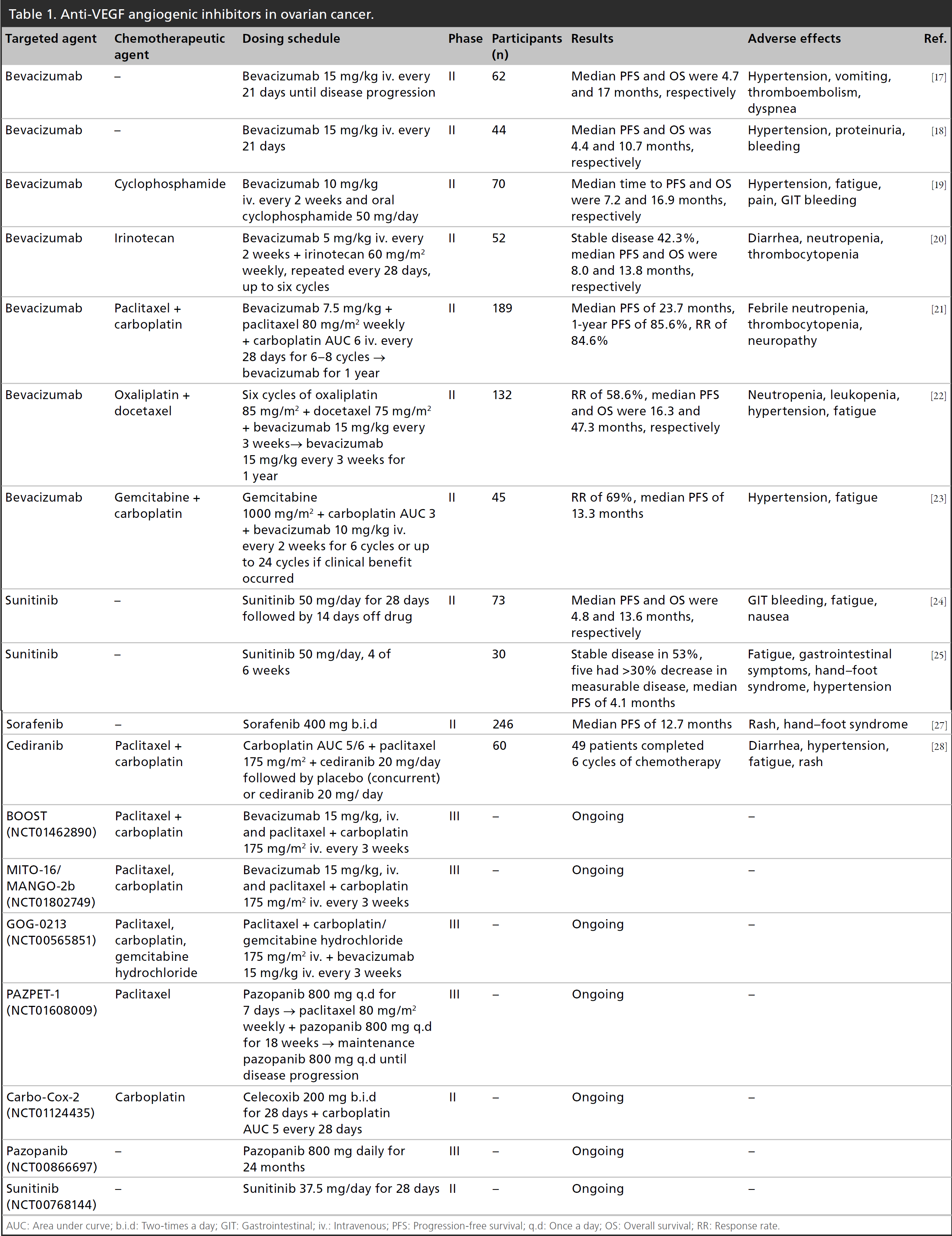
AUC: Area under curve; b.i.d: Two-times a day; GIT: Gastrointestinal; iv.: Intravenous; PFS: Progression-free survival; q.d: Once a day; OS: Overall survival; RR: Response rate.
In relapsed disease, both the OCEANS and AURELIA studies have evaluated addition of bevacizumab to chemotherapy and demonstrated an improvement in PFS. In AURELIA, for patients with relapsed platinum-resistant ovarian cancer, median PFS was 3.4 months with chemotherapy alone versus 6.7 months in conjunction with bevacizumab [29]. Likewise, in the OCEANS trial, addition of bevacizumab to carboplatin and gemcitabine in patients with relapsed platinum-sensitive ovarian cancer prolonged PFS at 12.4 months in the combination therapy group in comparison with 8.4 months in the chemotherapy group [30]. The AURELIA study revealed a 2.2% risk for gastrointestinal perforation with the addition of bevacizumab, however the risk for perforation was lower than expected, given that patients with ovarian cancer are at a higher risk for perforation than other solid organ malignancies. Overall, increased risk for perforation with addition of bevacizumab is small and does not outweigh its clinical benefit. Likewise, preliminary results from a Phase II study showed similar response rates and safety profile in patients treated with aflibercept, a VEGF monoclonal antibody [31]. Following these encouraging findings, Phase III trials are in progress involving VEGF inhibitors singly or in combination with chemotherapy (Table 1).
The success with use of bevacizumab for treatment of ovarian cancer has provided a useful platform for the introduction of other antiangiogenic agents. Targeting the intracellular tyrosine kinase component of VEGFR has been assessed in Phase II studies of pazopanib, sunitinib, sorafenib and cediranib (Table 1). They have demonstrated activity in patients with recurrent ovarian cancer, resulting in tumor responses and stabilization of disease, delaying tumor progression. In particular, pazopanib is an angiogenic multikinase inhibitor with broad spectrum activity against all three VEGF receptors, PDGFR and c-Kit [32]. This was demonstrated in a Phase III study of 940 women with advanced ovarian cancer where pazopanib prolonged disease-free survival by 5.6 months compared with placebo [33]. The PFS was 17.9 months for the patients receiving pazopanib and 12.3 months for the placebo group after 24 months. Pazopanib may be an effective agent as maintenance therapy, with manageable adverse events including nausea and neutropenia [34]. One key limitation of clinical studies involving newer targeted agents in ovarian cancer is the relatively small number of patients enrolled. Larger studies are required to provide more definitive demonstration of efficacy in combination with chemotherapy for the treatment of ovarian cancer. Furthermore, reported outcomes in the different trials included various response and survival measures. Hence, methodological differences between clinical studies and nonstandardized methods in evaluation of patient outcomes warrant caution when interpreting their findings.
Combinations of targeted antiangiogenic agents are also being explored. A Phase I and II study of bevacizumab and sorafenib showed six Response Evaluation Criteria in Solid Tumors (RECIST) partial responses in 13 ovarian cancer patients, with response duration from 4 to 22 months [35]. However, severe toxicities were reported with combination of bevacizumab and sorafenib, including grade 4 hypertension, proteinuria and two fistula formation at sites of disease response. These adverse events led to use of lower doses of both agents in a subsequent Phase II study [36]. By contrast, preliminary results from a Phase I study of bevacizumab and vascular disrupting agent (VDA) combretastatin 4A phosphate showed no additive toxicity and evidence for efficacy was encouraging, offering a potential treatment approach to be further evaluated [37].
Non-VEGF angiogenic inhibitors
Targeting the angiopoietin axis with non-VEGF inhibitors is an alternate strategy in ovarian cancer and is still undergoing early clinical trials [38]. Trebananib, a peptide-Fc fusion protein (peptibody) inhibiting the interaction of angiopoietin-1 and -2 to the Tie2 receptor, has been evaluated in combination with paclitaxel in recurrent ovarian cancer [39]. The results of a Phase III trial have been promising. Participants were treated with paclitaxel alone or paclitaxel and trebananib [40]. Notably, PFS was significantly longer in the combination therapy group at 7.2 months compared with 5.4 months for those treated with paclitaxel alone. Angiogenic inhibition via Tie2/angiopoietin pathway inhibition may offer effective treatment for advanced recurrent ovarian cancer. Further exploration within the TRINOVa-3 trial of trebananib in combination with carboplatin and paclitaxel is underway.
PARP inhibitors
PARP is a key enzyme involved in the repair of DNA single-strand breaks using the base excision repair pathway [41]. PARP inhibition results in accumulation of DNA single-strand breaks, which lead to DNA double-strand breaks at replication forks [42]. Double-strand breaks are effectively repaired in normal cells by homologous recombination (HR) DNA repair mechanisms [43]. In the absence of functional BRCA1 or BRCA2 proteins, alternative DNA repair pathways such as nonhomologous end joining are used, resulting in chromosomal instability and cell death [44]. As such, women with inherited mutations in
Clinical trials in recurrent ovarian cancer have demonstrated single-agent activity of PARP inhibitors [47–49]. The first Phase I trial of olaparib was evaluated in patients with
Several Phase II and III trials are currently evaluating olaparib in combination with chemotherapy [54–56]. PARP inhibition in combination with DNA-damaging agents may enhance the effects of chemotherapy and potentially delay treatment resistance [57]. A recent Phase II trial demonstrated olaparib in conjunction with paclitaxel and carboplatin followed by maintenance monotherapy significantly improved PFS compared with paclitaxel and carboplatin alone [58]. The greatest clinical benefit was seen in
PARP inhibitors in ovarian cancer.

b.i.d: Two-times a day; iv.: Intravenous; OS: Overall survival; PFS: Progression-free survival; RR: Response rate.
The use of PARP inhibitors could also be extended to sporadic ovarian cancers with HR defects due to loss of function of DNA repair proteins, including RAD51, ATM and ATR [65]. These sporadic tumors appear to phenocopy BRCA1- or BRCA2-deficient tumors although they do not possess germline mutations in either gene, a phenomenon termed ‘BRCAness' [66]. Further studies are required to identify patients with HR-defective tumors who are most likely to benefit from this new therapy. A randomized placebo-controlled trial of olaparib as maintenance therapy in patients with sporadic ovarian cancer is ongoing (NCT00753545).
EGFR inhibitors
The EGFR is overexpressed in up to 70% of ovarian cancers and is associated with poor prognosis and chemoresistance [67]. Responses to EGFR inhibitors in recurrent ovarian cancer are infrequent and dependent on a mutation in the EGFR catalytic domain [68]. Studies of EGFR tyrosine kinase inhibitors (erlotinib and gefitinib) and monoclonal antibodies against EGFR (cetuximab, panitumumab and matuzumab) have shown only modest efficacy (Table 3). For example, a Phase II trial of 837 patients with ovarian cancer treated with anti-HER2 monoclonal antibody, trastuzumab, showed only 7.3% of the 41
EGFR inhibitors in ovarian cancer.

AUC: Area under curve; iv.: Intravenous; OS: Overall survival; PFS: Progression-free survival; PLD: Pegylated liposomal doxorubicin.
Folate receptor inhibitors
The αFR is overexpressed in ovarian cancer and represents a potent target for therapy [82]. An overexpression might confer a tumor growth advantage by increasing folate availability to cancer cells where the degree of αFR expression has been shown to correlate with the grade of malignancy [83]. Farletuzumab, a monoclonal antibody to αFR, inhibits the growth of cells that overexpress αFR and activates antibody-dependent cell-mediated cytotoxicity and complement-mediated cytotoxicity [84]. In a Phase II study of 54 patients with platinum-sensitive relapsed disease, in which farletuzumab was given in combination with chemotherapy, there were encouraging signs of benefit [85]. Specifically, 37 patients showed normalization of CA-125 levels while 12 demonstrated a longer period of remission than their previous remission. Moving forward, larger randomized trials of farletuzumab are anticipated.
αFR is also being investigated as a selective drug target for a series of new quinazoline anti-folates. These include BGC945, a potent inhibitor of thymidylate synthase and highly selective for αFR [86]. Encouraging data from Phase II trials showed an improvement in PFS from 2.7 to 5 months. Similarly, selectively therapy targeting the folate receptor is being developed by using EC145, a conjugate of desacetylvinblastine monohydrazide linked through a peptide spacer to folate receptor targeting moiety [87]. The first study, PRECEDENT comparing EC145 and PLD with PLD alone showed an improvement in PFS of 20% [88]. Folate targeted agents have shown promising antitumor activity in ovarian malignancy and their continual development remains an active area.
IGFR inhibitors
IGF-1 is involved in inhibition of apoptosis, tumor progression and metastases [89]. Support for a role of IGF-I in ovarian cancer progression arose from a recent study which showed high free IGF-I protein expression in ovarian tumor tissue was independently associated with disease progression [90]. Moreover, IGF-I mRNA expression levels were positively associated with ovarian cancer progression, suggesting endocrine and paracrine regulations of IGF-I activity are involved in this disease [91]. As such, IGF-1 is a potential effective therapeutic target. In particular, aMG 479 is a monoclonal antibody that is a potent inhibitor of the IGF-1 receptor and a randomized Phase II study of aMG 479 added to first-line chemotherapy in patients with optimally debulked ovarian cancer is underway (NCT00719212).
Limitations & challenges
Despite promising results of established targeted agents, including PARP and VEGF inhibitors, there remain several challenges to further refine their clinical development. These include the identification of the correct population to treat as well as a clearer understanding of mechanisms underlying drug resistance. In particular, PARP inhibitors have demonstrated maximal effect in germline
In addition to difficulties in identifying appropriate patient candidates, there are patients with HR-deficient tumors who do not respond or develop resistance to PARP inhibition [94]. This suggests tumors can have both
Additional challenges facing the success of targeted therapy include identification of biomarkers to guide management and assess response. The complexity of signaling cascades and lack of specificity of small molecules make it difficult to predict which therapy will be successful or identify appropriate patient populations. Although a range of predictive biomarkers have been proposed, such as the plasma levels of circulating VEGFA, soluble VEGFR and basic fibroblast growth factor, none have proven to be robust [102,103]. A potential alternative is to use functional imaging techniques, such as diffusion contrast-enhanced magnetic resonance imaging and fluoro-
Conclusion
In conclusion, ovarian cancer remains a therapeutic challenge due to advanced disease at presentation and limited success of traditional treatment approaches. Understanding molecular changes driving ovarian cancer is critical for selection of appropriate candidate agents and success of these agents in improving clinical outcome. This allows for the development of effective targeted therapeutic approaches demonstrated by the various clinical trials discussed above. These therapies facilitate a shift in ovarian cancer management from empirical cytotoxic therapies to individualized approavhes targeted against specific pathological features of each tumor.
Future perspective
Several emerging targeted therapies have been highlighted in this review. Of the various targeted therapies under evaluation in Phase II and III studies, the most promising strategies developed thus far are antiangiogenic agents and PARP inhibitors. Therapies targeting specific molecular features as strategies in the treatment of ovarian cancer have been clearly demonstrated with PARP inhibitors. Specifically, this has been exemplified by addition of olaparib in the maintenance treatment of women with platinum-sensitive
In addition to PARP inhibitors, angiogenic inhibitors may similarly be incorporated into clinical practice in the future. One of the most important cytokines responsible for tumor-mediated angiogenesis is VEGF. Efforts to block this pathway have arisen as attractive strategies for ovarian cancer treatment. The most promising antiangiogenic agent to date is bevacizumab. As discussed above, studies have shown a significant improvement in PFS with concurrent use of bevacizumab and chemotherapy in comparison with chemotherapy alone. However, several studies have demonstrated mixed results with addition of bevacizumab to chemotherapy. The GOG-218 study reported improvement in OS with bevacizumab which was not statistically significant, with median OS of 38.6 months on standard chemotherapy compared with 42.1 months on combined therapy [15]. Similarly, in the ICON-7 study, there was no OS difference with the combination treatment regimen in the overall study population with a mean survival of 44.6 months with standard chemotherapy compared with 45.5 months with addition of bevacizumab [16]. Notably, there was an OS benefit in a high-risk subset of 502 patients with inoperable or suboptimally cytoreduced stage III or IV disease, with mean OS of 34.5 months in the chemotherapy alone group compared with 39.3 months with bevacizumab. When considering the balance of clinical benefit, quality of life preservation and tolerability of bevacizumab in combination with chemotherapy, this treatment regimen could be appropriate as a front-line option for advanced ovarian cancer supported by consistent clinical evidence. Although adverse events are not commonly observed with use of bevacizumab, those that occur can usually be managed with close monitoring and dose adjustment. In addition, significant activity demonstrated with concurrent targeted treatment suggests it could be an alternate therapeutic approach to standard chemotherapy. Strategies such as combining multiple antiangiogenic agents or the concurrent use of antiangiogenic agents with chemotherapy may overcome resistance [105]. Combinatorial targeted therapies could involve either vertical or horizontal pathway blockade and is useful in counteracting negative feedback loops. Notably, the combination of bevacizumab and sorafenib is an example of vertical pathway blockade [106]. This combination is noteworthy for its substantial efficacy and favorable safety profile compared with either of the single agents. Moreover, use of PARP inhibitors with antiangiogenic agents may circumvent increased VEGFR2 phosphorylation and subsequent activation of endothelial cell survival, seen in PARP inhibitor monotherapy [107]. Care must be taken to appropriately manage toxicities demonstrated with combination therapy, especially with increased myelosuppression seen with these regimens. This may involve patient stratification based on altered oncogenic pathways or intermittent dosing strategies. New targeted approaches, including immune checkpoint inhibitors, are also being examined and have shown promising potential [108,109]. This includes nivolumab which is a human IgG4 monoclonal antibody that targets PD-1 and stimulates antitumor immune responses. A Phase II study of nivolumab has demonstrated encouraging clinical efficacy and tolerability in patients with platinum-resistant ovarian cancer with median PFS of 3.5 months and OS of 20.0 months [108]. Further clinical trials are underway to establish the clinical use of these targeted agents. Alternate routes of administration may also be considered to ensure effective delivery of drugs to the intended site of action. The advantages of administering chemotherapy into the peritoneal cavity are supported by both preclinical and clinical trials [110–113]. In comparison with iv. treatment, ip. administration achieves a fourfold increase in drug concentration within the abdominal cavity [110]. In addition, long-term results from two studies demonstrated the benefits of ip. administration of chemotherapy over iv. administration following surgery in patients with advanced ovarian cancer [113,114]. The data arise from a 10-year follow-up of patients involved in GOG trials 114 and 172.
Executive summary
Of the VEGF-targeting therapies, the most thoroughly investigated targeted drug is bevacizumab, a recombinant monoclonal anti-VEGF antibody. Phase III trials (ICON-7 and GOG-218) showed substantial benefit in progression-free survival (PFS) in the bevacizumab maintenance arm compared with standard chemotherapeutic regimen in stage 3–4 ovarian cancer. In relapsed disease, both OCEANS and AURELIA trials have demonstrated an improvement in PFS with addition of bevacizumab to chemotherapy in elapsed platinum-sensitive ovarian cancer. Success witnessed with bevacizumab has provided a useful platform for introduction of other antiangiogenic agents, including pazopanib, sunitinib and sorafenib.
Trebananib, a peptibody inhibiting the interaction of angiopoietin-1 and -2 to the Tie2 receptor, has been evaluated in combination with paclitaxel in recurrent ovarian cancer. The results of a Phase II trial have been promising, where study participants were treated with paclitaxel alone or paclitaxel and Trebananib. PFS was significantly longer in the combination therapy group at 7.2 months compared with 5.4 months for those treated with paclitaxel alone.
PARP inhibitors in Olaparib maintenance therapy significantly prolonged PFS compared with placebo in patients with A Phase II trial demonstrated olaparib in conjunction with paclitaxel and carboplatin followed by maintenance monotherapy significantly improved PFS compared with paclitaxel and carboplatin alone, with greatest clinical benefit seen in Combinations of olaparib with other chemotherapeutic agents are underway (NCT01445418, NCT01237067, NCT00516724, NCT01081951).
Responses to EGFR inhibitors in recurrent ovarian cancer are infrequent and dependent on a mutation in the EGFR catalytic domain. Studies of EGFR tyrosine kinase inhibitors (erlotinib and gefitinib) and monoclonal antibodies against EGFR (cetuximab, panitumumab and matuzumab) have shown only modest efficacy.
In a Phase II study of 54 patients with platinum-sensitive relapsed disease, in which farletuzumab was given in combination with chemotherapy, 37 patients showed normalization of CA-125 levels while 12 demonstrated an extended period of remission than their previous remission. αFR is also being investigated as a selective drug target for a series of new quinazoline antifolates, including BGC945 and EC145.
High free IGF-I protein expression in ovarian tumor tissue was independently associated with disease progression. A Phase II study of aMG 479, a monoclonal antibody of IGF-1 receptor, added to first-line chemotherapy in patients with optimally debulked ovarian cancer is underway.
PARP inhibitors: urgent need for validated biomarker for HR-deficient ovarian cancer predictive of response to PARP inhibition and understanding drug resistance mechanisms underlying drug resistance. Differences between different PARP and VEGF inhibitors have yet to be fully defined. Use of new targeted agents will be improved by development of multiple biomarkers to identify patients most likely to benefit and monitor treatment response.
Of the various targeted therapies under evaluation in Phase II and III studies, the most promising strategies developed thus far are antiangiogenic agents and PARP inhibitors. When considering the balance of clinical benefit, quality of life preservation and tolerability of bevacizumab in combination with chemotherapeutic agents, this treatment regimen could be appropriate as a front-line option for advanced ovarian cancer. Combinatorial targeted therapies could also involve either vertical or horizontal pathway blockade and is useful in overcoming drug resistance. Possibility of treatments targeted to specific groups of patients on the basis of robust predictive biomarkers.
After 876 women from the two trials had undergone primary surgical cytoreduction, they were randomized to receive either ip. or iv. chemotherapy. There was a significant improvement in OS with the ip. route compared with iv. administration. Specifically, median OS with ip. therapy was 61.8 months compared with 51.4 months for patients treated with iv. chemotherapy. This difference resulted in a 23% decreased risk for death. Moreover, ip. therapy was also associated with improved survival among those patients with gross residual disease. Similarly, a review of ip. chemotherapy in women undergoing treatment for advanced ovarian cancer reported a 21% decrease in the risk of death in patients undergoing combined ip. and iv. therapy compared with those undergoing iv. therapy alone [115]. Additional trials are underway to define the optimal number of cycles of ip. chemotherapy while minimizing treatment-related toxicity and infection risk. Furthermore, recent advances in nanotechnology enable various types of nanoparticles to improve the therapeutic efficacy of anticancer drugs [116,117]. Their properties can be designed for targeted delivery to tumors and remain a new area of study to modulate ip. therapy [116]. These include multifunctional polymer micelles, lipid nanoparticles and polymeric nanoparticles. The delivery and therapeutic efficacy of majority of nanoparticles are still under investigation, and studies are primarily limited to preclinical stages currently [118–120]. For example, a preclinical study using a lipidoid ip. delivery system to deliver small interfering RNA (siRNA) to PARP1 in a
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.