
Abstract
The US FDA has recently approved the combination of carboplatin and gemcitabine as a second-line therapy for recurrent platinum-sensitive ovarian cancer. This article briefly reviews the pharmacokinetics and mechanism of action of gemcitabine and its synergistic effect with platinum. An overview of the literature on the role of gemcitabine in the treatment of epithelial ovarian cancer is also presented.
The majority of patients with epithelial ovarian cancer experience a complete clinical response after their initial treatment with surgical debulking and platinum-based chemotherapy. However, more than 75% of the patients with a complete response will suffer from recurrence within 5 years [1,2]. If recurrence occurs more than 6 months after the last platinum treatment, patients are considered to have a potentially platinum-sensitive disease [3,4], which exhibits a 30% response rate to single-agent carboplatin and carries an overall better prognosis [5,6]. On the other hand, if recurrence occurs less than 6 months after the last platinum treatment, patients are considered to have platinum-resistant disease, which is less likely to respond to second-line regimens and carries a poor prognosis [7].
Current treatment goals for recurrent ovarian cancer include: treating symptoms if present and prolonging the progression-free survival (PFS), with an aim to improve the overall survival (OS) of patients. This needs to be done whilst carefully balancing chemotherapy-related toxicity, patient's quality of life and the expected survival benefit from therapy. In order to achieve these goals, new cytotoxic agents and combination chemotherapy regimens are being investigated.
Gemcitabine is a synthetic nucleoside analog of cytidine with broad activity in solid tumors. Over the last 10 years, studies have confirmed the potential role of gemcitabine in the treatment of ovarian cancer. These studies led to the European (2004) and US (2006) approval of carboplatin plus gemcitabine for patients with ovarian cancer recurring more than 6 months after the completion of platinum therapy. Other studies have explored the role of gemcitabine in platinum-resistant recurrent ovarian cancer and as part of the first-line regimen for newly diagnosed patients.
Gemcitabine
Introduction to gemcitabine
Gemcitabine (2′-deoxy-2′,2′-difluorocytidine monohydrochloride) is a pyrimidine analog (Figure 1) with broad activity in solid tumors, including lung, pancreatic and breast cancers [8]. Gemcitabine is cell-phase specific, killing cells in the S phase and blocking the progression from G1 to S. Intracellularly, gemcitabine is transformed into two active metabolites: diphosphate (dFdCDP) and triphosphate (dFdCTP) nucleosides. Gemcitabine diphosphate inhibits ribonucleotide reductase, causing a reduction in the concentrations of deoxynucleotides, while gemcitabine triphosphate competes with dCTP for incorporation into DNA and stops further elongation of the DNA strand (Figure 2) [9,10].

Gemcitabine.

Metabolic pathways for self-potentiation of gemcitabine nucleotides.
Gemcitabine is administered intravenously with a volume of distribution that increases with the length of infusion. The half-life of gemcitabine for short infusions ranges from 42–94 min, and for long infusions varies from 245–638 min, depending on the patient's age and gender. Gemcitabine is mainly excreted through the kidneys and its clearance is lower in women and the elderly [11].
Combination of gemcitabine & platinum
Villella and colleagues reported a 55% response rate using gemcitabine plus carboplatin in patients with recurrent ovarian cancer. Even patients with initial platinum resistance experienced a 42% overall response rate [17].
Gemcitabine for recurrent ovarian cancer
Single-agent gemcitabine in recurrent ovarian cancer
Studies have shown that single-agent gemcitabine is active against recurrent ovarian cancer [18–26] (
Single-agent gemcitabine for recurrent ovarian cancer.
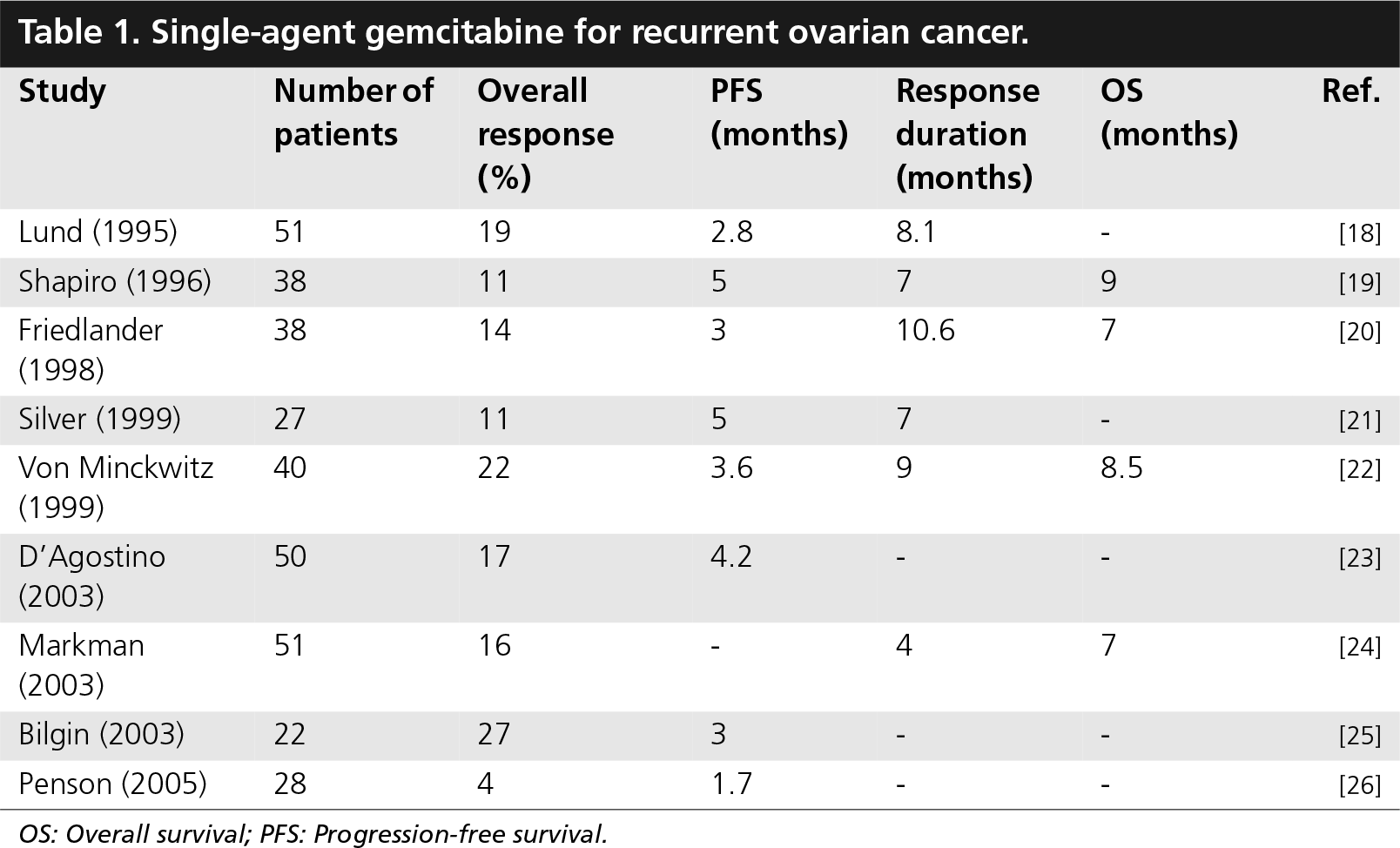
OS: Overall survival; PFS: Progression-free survival.
In the study by Penson and colleagues, which reported the lowest response rate, the patients received 700–800 mg/m2 only on days 1 and 8 of a 21-day cycle, which is less than what patients received in the other trials, while 50% of them had liver metastatic disease [26].
Combination gemcitabine & platinum in platinum-sensitive recurrent epithelial ovarian cancer
A Phase I/II dose-escalating study was conducted by the Arbeitsgemeinschaft Gynäkologische Onkologie studiengruppe Ovarialkarzinom (AGO-OVAR) investigators using gemcitabine plus carboplatin in patients with platinum-sensitive recurrent ovarian cancer. The dose-limiting toxicity was myelosupression, mostly thrombocytopenia. The maximal tolerated dose of gemcitabine was 1000 mg/m2 given on days 1 and 8 of a 3-week schedule combined with carboplatin area under the curve (AUC) 4 given on day 1 [32]. This study was followed by two Phase II trials that confirmed the efficacy and tolerability of this regimen (
Gemcitabine plus carboplatin in patients with platinum-sensitive recurrent ovarian cancer.
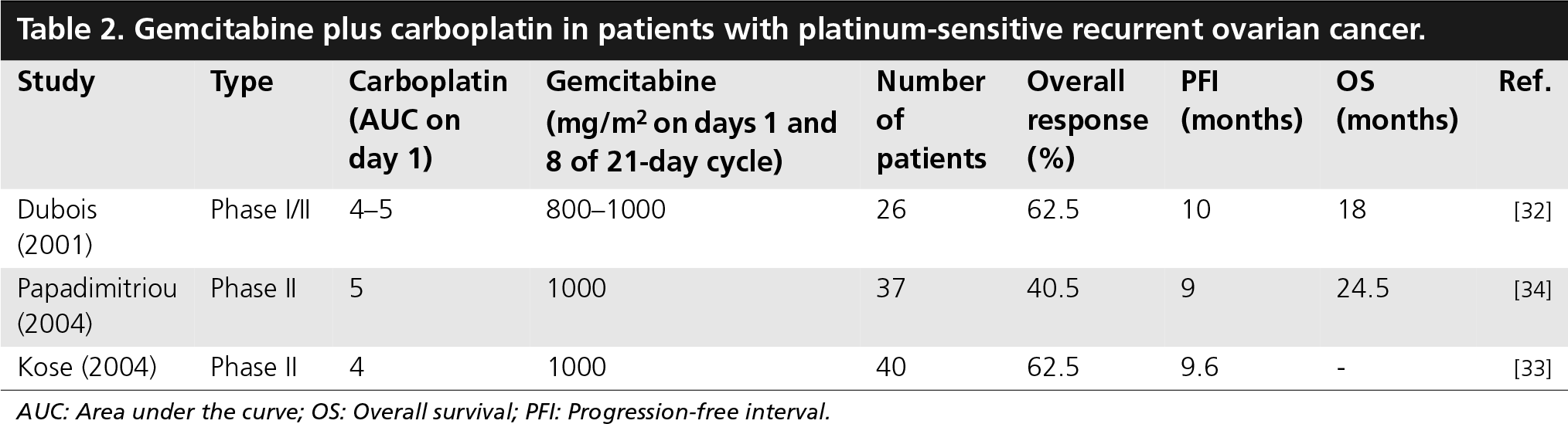
AUC: Area under the curve; OS: Overall survival; PFI: Progression-free interval.
A large, intergroup, randomized, controlled trial comparing gemcitabine plus carboplatin with carboplatin alone in patients with platinum-sensitive recurrent ovarian cancer has recently been completed (
Summary of the randomized, controlled trial comparing carboplatin plus gemcitabine with carboplatin alone in patients with platinum-sensitive recurrent ovarian cancer.
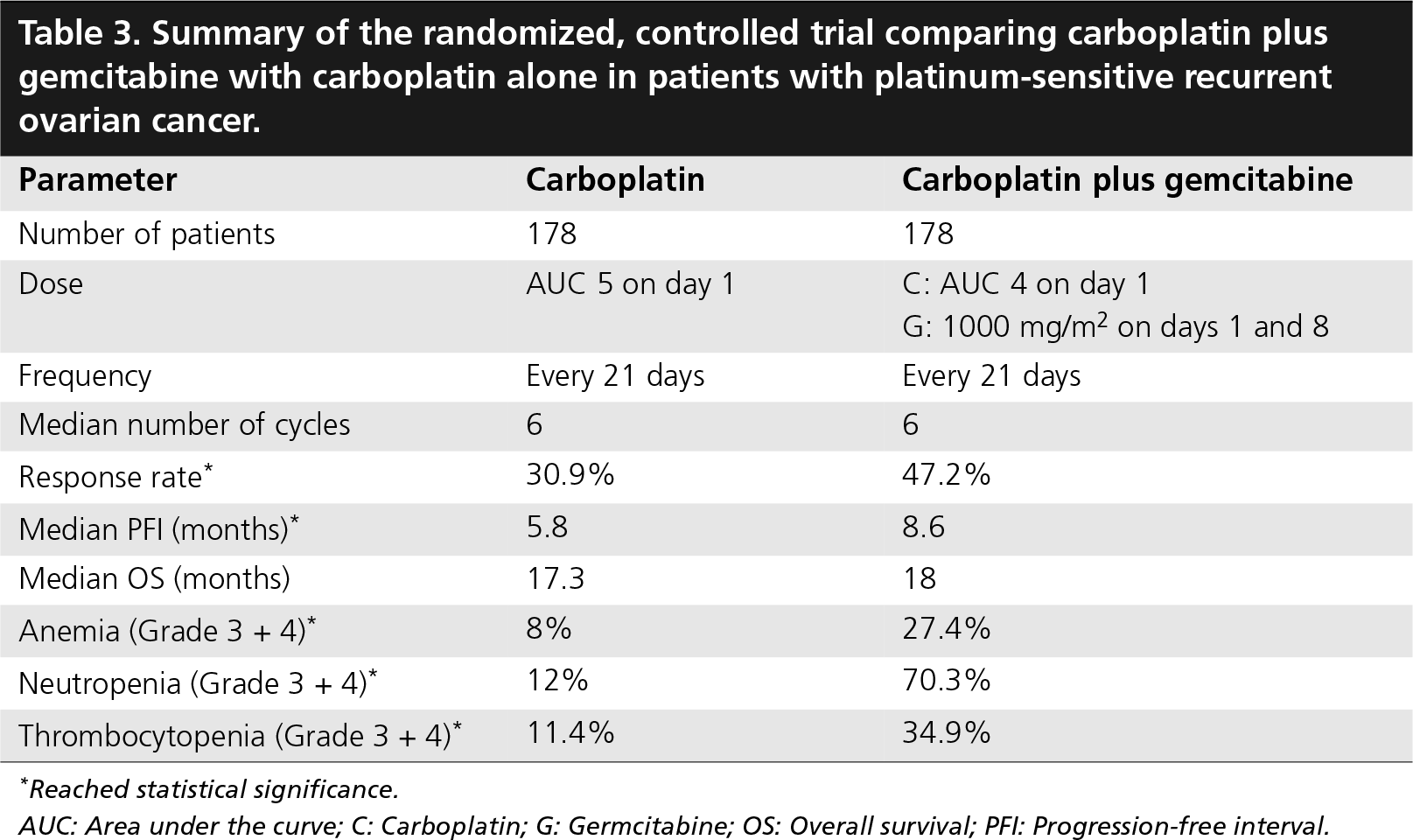
Reached statistical significance.
AUC: Area under the curve; C: Carboplatin; G: Germcitabine; OS: Overall survival; PFI: Progression-free interval.
Combination gemcitabine & platinum in platinum-resistant recurrent ovarian cancer
Given the rising evidence of the synergistic cytotoxicity of cisplatin plus gemcitabine in ovarian cancer cell lines, and the ability of gemcitabine to overcome platinum resistance by inhibiting DNA repair [12–16], the combination of gemcitabine plus platinum was used in patients with platinum-resistant ovarian cancer (
Gemcitabine plus cisplatin in patients with platinum-resistant recurrent ovarian cancer.

mg/m2 on days 1 and 8 of 28-day cycles.
OS: Overall survival; PFI: Progression-free interval.
In another study, a more intense regimen consisting of biweekly gemcitabine 1000 mg/m2 and cisplatin 40 mg/m2 on days 1 and 15, repeated every 4 weeks, was well tolerated and effective (response rate [RR] = 31.5%) in 35 evaluable patients with platinum-refractory ovarian cancer [41]. The authors found that patients with a progression-free interval less than 3 months after platinum-therapy had lower response rates to gemcitabine and cisplatin (15.8 vs 50%, p = 0.03) than patients with longer intervals. Recently, Lehoczky and colleagues published their experience using carboplatin plus gemcitabine in 22 heavily pretreated patients (median of four regimens) with recurrent platinum-resistant ovarian cancer. Carboplatin was given at a dose of AUC 4 on day 1, and gemcitabine was given at a dose of 1000 mg/m2 on days 1 and 8 of a 3-week cycle. The authors reported a 39% overall response rate with only one complete response and a median progression-free interval of 3 months [42].
Combination gemcitabine & paclitaxel in recurrent ovarian cancer
A Phase I dose-finding study by Iaffaioli showed the feasibility and safety of combination gemcitabine and paclitaxel in 14 patients with advanced recurrent ovarian cancer. The investigators used a fixed dose of gemcitabine of 1000 mg/m2 on days 1 and 8 of a 21-week cycle, and an escalating dose of paclitaxel starting at 90 mg/m2 on day 1 of the cycle. The maximum tolerated dose was 240 mg/m2 of paclitaxel. All patients received granulocyte colony-stimulating factors [44].
In another Phase I study, the sequence and dose of the regimen were evaluated. The administration of gemcitabine before paclitaxel resulted in the elevation of liver enzymes, which prompted the investigators to abandon this sequence in favor of administering paclitaxel prior to gemcitabine [45]. Table 5 summarizes the studies evaluating gemcitabine plus paclitaxel in patients with recurrent ovarian cancer [44–46].
Gemcitabine plus paclitaxel in patients with recurrent ovarian cancer.

OS: Overall survival; PFI: Progression-free interval.
Other combination chemotherapy regimens that contain gemcitabine for recurrent ovarian cancer
Preclinical
Gemcitabine plus liposomal doxorubicin in patients with recurrent ovarian cancer.
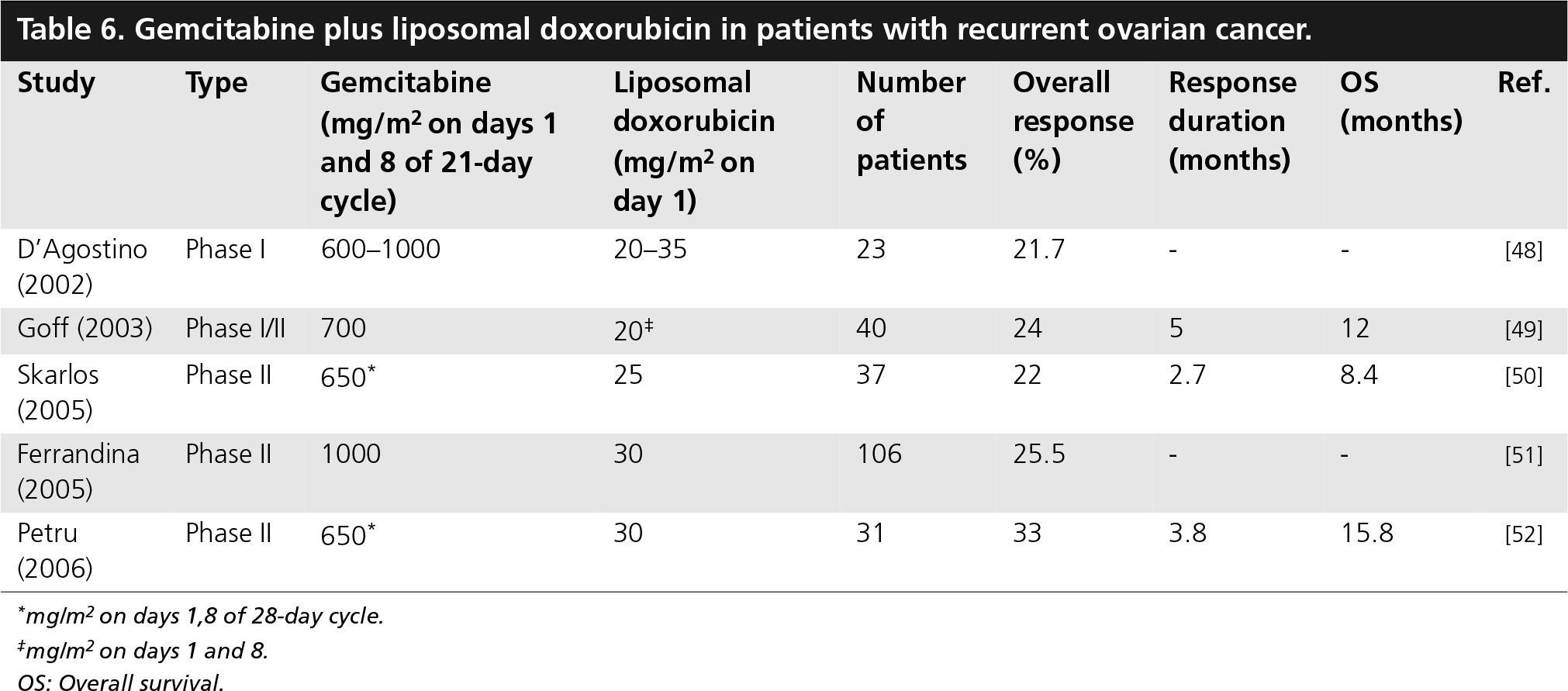
mg/m2 on days 1,8 of 28-day cycle.
mg/m2 on days 1 and 8.
OS: Overall survival.
Trials using combination gemcitabine and topotecan for patients with recurrent ovarian cancer used different regimens and had variable results [53–55]. The GOG Phase I trial by Chen and colleagues was closed early owing to the high rates of neutropenia, thrombocytopenia and stomatitis (
Gemcitabine plus topotecan in patients with recurrent ovarian cancer.

OS: Overall survival.
Triplet therapy with gemcitabine, carboplatin and paclitaxel for patients with recurrent ovarian cancer showed very promising results in several studies, with overall response rates between 75 and 100% [56,57].
Gemcitabine as a first-line therapy for epithelial ovarian cancer
Single-agent gemcitabine was evaluated in previously untreated patients with Stage III/IV ovarian cancer. The response rate was limited to 18% [58]. A Phase I GOG trial showed that combining paclitaxel 135 mg/m2, carboplatin AUC 5, and gemcitabine 800 mg/m2 is feasible, with an acceptable toxicity profile [59]. Several Phase II studies evaluated different combination (
Gemcitabine in first-line regimens for epithelial ovarian cancer.

OS: Overall survival; PFS: Progression-free survival.
Gemcitabine in sequential (doublet) regimens as first-line therapy for epithelial ovarian cancer.

PFS: Progression-free survival.
These overall encouraging results led to the GOG 182/ICON5 study [72]. This is an international collaborative multicenter randomized, controlled trial that evaluated four new combination chemotherapy regimens as first-line therapy for patients with Stage III and IV ovarian cancer. Two of the five study arms contained gemcitabine. One was the combination of gemcitabine with carboplatin and paclitaxel. The second was a doublet regimen, where patients receive four courses of carboplatin and gemcitabine followed by four cycles of carboplatin and paclitaxel. The preliminary results of this trial showed that adding a third cytotoxic agent did not prolong progression-free or OS. Two other Phase III studies for previously untreated patients are currently in progress and have completed enrollment. The AGO-OVAR 9 study is comparing carboplatin plus paclitaxel with or without gemcitabine [73], and the Eli Lilly-sponsored S302 study is comparing carboplatin plus paclitaxel versus carboplatin plus gemcitabine, with or without consolidation therapy. Results of both studies are awaiting data maturation.
Conclusion
In order to achieve better response rates and disease progression survival, new agents and different combination therapy regimens are being evaluated in patients with epithelial ovarian cancer. Gemcitabine showed activity in primary and recurrent ovarian cancer, in both platinum-sensitive and -resistant disease. The toxicity of gemcitabine is well tolerated overall when given alone or in combination with other regimens, even in heavily pretreated patients. The commonly reported toxicities of gemcitabine include nausea and vomiting, abnormal liver enzymes, fever and edema, with myelosupression being the dose-limiting toxicity. The rare incidence of neurotoxicity allows gemcitabine to be used in combination with paclitaxel and in patients with paclitaxel-related neurotoxicity.
In patients with platinum-sensitive recurrent ovarian cancer, the International Collaborative Ovarian Neoplasm (ICON)4/AGO-OVAR trial showed that paclitaxel plus platinum-based chemotherapy results in a higher response rate and longer PFS and OS when compared with single-agent platinum (carboplatin or cisplatin). However, despite the fact that only 34% of the patients had received prior taxanes, the combination regimen was associated with high (20%) neurotoxicity, which may limit its use in patients with residual neurotoxicity from their primary therapy [74]. In another randomized, controlled trial, the combination of carboplatin and gemcitabine was superior to single agent carboplatin in terms of its response rate and PFS, with an equivalent quality of life [35]. This trial was not powered to detect differences in survival, which as an end point may be confounded by subsequent treatments.
Given the proven survival benefit for carboplatin plus paclitaxel, it is considered to be an acceptable choice in patients with recurrent platinum-sensitive ovarian cancer. However, carboplatin plus gemcitabine represents a very attractive alternative given the proven efficacy and the lower toxicity (less neurotoxicity and rare alopecia). It should be strongly considered for patients with significant residual neuropathy, those who do not tolerate paclitaxel and those who refuse paclitaxel therapy because of potential undesirable side effects like alopecia. Table 10 summarizes the results of the combination arm of each of the two trials.
Comparing the intervention arms of the two randomized, controlled trials evaluating combination regimens versus conventional single-agent platinum in patients with platinum-sensitive recurrent ovarian cancer.

HR: Hazard ratio.
For patients with platinum-resistant ovarian cancer, combination regimens containing gemcitabine are well tolerated and seem to have higher response rates than single-agent therapies. However, these conclusions are based on retrospective and Phase II studies. Thus, randomized comparative trials are needed to determine the role of combination regimens containing gemcitabine in this group of patients.
The role of gemcitabine as a first-line therapy for ovarian cancer was evaluated in many Phase I and II studies using different combinations and doses. Despite the encouraging results of these studies, adding gemcitabine to first-line regimens offered no PFS or OS benefit in the GOG/ICON5 trial. Therefore, carboplatin plus paclitaxel remains the standard therapy for previously untreated patients with advanced ovarian cancer.
Future perspective
Chemotherapy strategies for recurrent ovarian cancer are gradually shifting towards using combination regimens as opposed to single-agent therapies. This is based on the improved response rates and PFS noted with several combination regimens in platinum-sensitive patients. In platinum-resistant patients, increasing numbers of Phase II trials evaluating combination regimens have been conducted or are on the way. However, combination chemotherapy may be associated with broader and more severe toxicities, which may limit its utility in some patients, such as elderly, heavily pretreated patients, or those with renal or liver dysfunction. Individualizing chemotherapy would allow clinicians to choose the regimens that are most likely to be effective for the individual patient's tumor, avoiding all the risks, toxicities and costs associated with the current treatment strategies that are based on treating the patient with the agents that have been shown in population-based studies to be the most effective. Genetic and epigenetic prognostic markers are being investigated. The development of markers predictive of response may allow a more educated guess when several options for planning chemotherapy are available. Agents that selectively target aberrant or overactive cell-signaling elements, apoptotic pathways, regulators of protein trafficking, and epigenetic DNA modifications are under investigation. Some of these agents may become an important adjunct to current treatment strategies of ovarian cancer.
Executive summary
Gemcitabine is a pyrimidine analog with proven activity against both platinum-sensitive and -resistant ovarian cancer.
Gemcitabine inhibits DNA repair, resulting in a synergistic activity when combined with platinum.
Combination gemcitabine and carboplatin is approved by the US FDA for treatment of platinum-sensitive recurrent ovarian cancer. The recommended dose is gemcitabine 1000 mg/m2 on days 1 and 8 of a 21-day cycle, and carboplatin area under the curve 4 on day 1.
Both regimens (carboplatin plus paclitaxel and gemcitabine plus carboplatin) are acceptable choices for platinum-sensitive recurrent ovarian cancer. However, gemcitabine plus carboplatin is preferred in patients with residual neurotoxity or those who do not tolerate or refuse paclitaxel.
Adding gemcitabine to first-line regimens offered no progression-free or overall survival benefit in the GOG/ICON5 trial. The results of two more Phase III trials are still pending.