
Abstract
Progestins are synthetic compounds that mimic the effects of progesteron. For over 50 years, oral progestins have been demonstrated to be effective in the treatment of endometriosis. They were reported to reduce or eliminate pain symptoms in approximately 90% of the patients. Progestins are available in many forms, including oral preparations, injections, subdermal implants and intrauterine systems. Continuous progestin use is an effective therapy for the treatment of painful symptoms associated with endometriosis but there had been no evidence of progestin use being superior to other types of treatment in endometriosis-related pain symptoms.
Endometriosis is defined as ‘the presence of viable, estrogen sensitive, endometrial-like glands and stroma associated with inflammatory response outside the uterus’ [1]. Endometriosis affects 6–10% of women in reproductive age and it has been reported to be found in women between 12 and 80 years old [2]. The average of diagnosis is approximately 28 years old [3]. It is reported in 21–47% of women with subfertility, 71–87% of women with chronic pelvic pain [4,5].
Pain is the major symptom in endometriosis. It was reported in 92% of the patients [1]. The pelvic pain due to endometriosis may be in the form of dysmenorrhea, dyspareunia or pelvic pain. Typically the pain precedes the onset of menses and lasts for the duration of the cycle. Less commonly patients also present with cyclical pain at other sites, relating to endometriosis at extrapelvic sites.
Endometriosis has a multifactorial etiology [1]. The theories on the disease include retrograde menstruation and refluxed endometrial tissue implanting on pelvic structures; metaplasia of the coelomic pluripotent mesothelial cells in the peritoneum and implantation of cells via hematogenous or lymphatic embolization.
The discovery of the molecular mechanisms associated with endometriosis improved the understanding of the traditional theories. Recently discovered features of endometriosis are chronic inflammation with increased cyclooxygenase activity and increased local aromatase activity, increased amount of activated macrophages and proinflammatory cytokines. Concomitant immune dysfunction impairs the clearance of the refluxed endometrial tissue and promotes the progression of the disease with aiding adherence and invasion, angiogenesis, sensory (sympathetic and parasympathetic) innervations [1].
The most important issue about medical treatment of endometriosis is the alternate treatments are all effective but the symptoms tend to recur after the discontinuation of the treatment [1]. Whatever the treatment is chosen, often long-term or repeated medication is necessary. Therefore, not only the efficacy, but also the tolerability and costs of a drug are relevant. First-line medical treatment should focus on the drugs that can be used for long term with minimal adverse effect profile.
NSAIDs may be utilized to control the pain due to endometriosis. On the failure of NSAID treatment, suppressive treatment should be initiated. The main principle is to induce amenorrhea. The first-line treatment choices are oral contraceptives and oral progestins. The GnRH analogs follow these drugs. Danazol has been shown to be effective to control endometriosis related pain. Levonorgestrel-containing intrauterine system (Mirena) can be used for the endometriosis-related pain so as antiprogesterone gestrinone and aromatase inhibitors such as letrozole and anastrozole (Table 1).
Noretistherone acetate (NETA), depot medroxyprogesterone acetate (DMPA), GnRH analogs and danazole are US FDA approved drugs in the treatment of endometriosis.
Progestins in the treatment of endometriosis
Progesterone is a steroid hormone which is the main source of production in ovaries, adrenal glands and placenta. During the menstrual cycle, with the effect of estrogen endometrium proliferates and following ovulation, secretion of progesterone from the corpus luteum inhibits proliferation of the endometrium and it enters into the secretory phase in which tissue remodeling is stimulated until the pregnancy or the menstrual shedding.
Progestins are synthetic compounds that mimic the effects of progesterone. The progestins differ with respect to their profile and potency of action on the hypothalamic–pituitary axis, metabolic processes, breast tissue and genital organs.
For over 50 years, oral progestins have been demonstrated to be effective in the treatment of endometriosis. They were reported to reduce or eliminate pain symptoms in approximately 90% of the patients [6].
Mechanism of action
The exact mechanism of action of progestins in controlling endometriosis related pain is still unknown since the basic mechanism of the endometriosis related pain is unexplained.
There are three main mechanisms suggested for the pain in endometriosis:
The effect of active bleeding from the endometriotic lesions;
The overexpression of the growth factors and proinflammatory cytokines in the ectopic endometrium;
The irritation or direct invasion of pelvic nerves.
The progestins stimulate atrophy or regression of endometrial lesions. The effectiveness of progestins for treating endometriosis is not just related to its growth inhibiting actions, but also to its induction of anovulation, inhibition of blood vessel growth and anti-inflammatory actions [7].
The common characteristic of progestins is the secretory transformation of estrogen-primed uterine endometrium, but the doses required to achieve this effect differ among the different derivatives [7]. Progestins also reduce the frequency and increase the amplitude of pulsatile gonadotropin-releasing hormone (GnRH) release, resulting in a reduction in follicle-stimulating hormone (FSH) and luteinizing hormone (LH) secretion. As a result of this effect, continuous application of progestins leads to the suppression of ovarian steroidogenesis with anovulation and low serum levels of ovarian steroids [7].
The long-standing hypo estrogenic and hypergestagenic state causes decidual transformation of the eutopic endometrium, and to some degree, the same effect is observed in ectopic lesions. In order to induce decidual transformation with resultant necrosis and resorption of the implant, however, concomitant estrogen action is required. As continuous progestin therapy results in low serum estradiol levels, breakthrough bleeding is a common occurrence.
Molecular effects on target tissue
The mode of action of the progestins on the endometriotic implant is still an unsettled issue.
Earlier studies postulated activity via the steroid receptor mechanism that secretory changes in ectopic lesions were followed by decidual transformation and atrophy. Later studies did not confirm this hypothesis. Endometriotic foci either contain progesterone receptors in very low concentrations or do not contain progesterone receptors (mainly PR-β is undetectable and PR-α is markedly reduced), and the function of the enzyme systems differ widely between eutopic and ectopic endometrial tissue [8]. As a contradiction, progestins cause the downregulation of their effects by reducing the synthesis of the receptors and as a result of all these alterations sensitivity of the implants decrease during long-term treatment.
Endometriosis has different patterns of action: some implants remained unchanged at the end of long-term progestin treatment; in some implants an arrest of growth was observed and some had secretory changes, but the expected decidual reaction and necrosis could not be revealed [9]. On the comparison of ultrastructural changes between eutopic and ectopic endometrium, endometriotic foci are found to remain proliferative in the luteal phase [10]. This insensitivity to the effect of progestins (progesterone blockage) may be as a result of alterations in enzyme or reduced receptor concentrations systems in the ectopic endometriotic implants [10].
Medical treatment alternatives for endometriosis-associated pelvic pain.

CPA: Cyproteone acetate; DNG: Dienogest; GI: Gastrointestinal; GnRH: Gonadotropin-releasing hormone; IUS: Intrauterine sysytem
LNG: Levonorgestrel; MPA: Medroxyprogesterone acetate; NETA: Noretistherone acetate.
In ectopic endometrium, 17-β-hydroxysteroid-dehydrogenase type 2 is defective and cannot be activated by progestins, resulting in increased proliferation, as estradiol is not inactivated [10]. Furthermore, aromatase in ectopic implants has been found to have a pathologic activity [10]. It is known that the endometriotic foci produce more estradiol, converting androgens to estrogens. A new mechanism of controlling the growth of endometriosis by progesterone and progestins was proposed recently, which postulates progestins were found to reduce TNF-α-induced NF-κB which in turn inhibits the proliferation of endometriotic stromal cells [11].
Moreover, progestins suppress the matrix metalloproteinases, which enable the implantation and progression of ectopic endometriotic implants [12]. In a rat endometrial autograft model, it was demonstrated that progestins (dienogest) inhibited the process of angiogenesis in the ectopic endometrium that reduced the development and progression of endometriotic implants. In addition, progestins were found to inhibit the proliferation of endometrial stromal cells in vitro due the arrest of cells in the G0/G1 phase of the cell cycle [13].
Another mechanism of action could be progestins' direct effect on nerve fibers. Progestins and combined oral contraceptives were found to reduce nerve fiber density and nerve growth factor and nerve growth factor receptor p75 expression in peritoneal endometriotic lesions [14].
The suggested mechanisms of progestins in resolving endometriosis-related pain are summarized as [6,7]:
Ovarian suppression;
Effects on endometrial morphology (desidualization, atrophy and alteration in steroid receptor ligand binding);
Local modulation of immune response (suppression of IL-8 production, increase of nitric oxide production, reduction of TNF-α induced nuclear factor-χ-β);
Effects on angiogenesis (suppression of transcription of bFGF, suppression of VEGF and cysteine rich angiogenic inducer [CYR61]);
Progesterone receptor expression and progesterone resistance;
Direct effect on nerve fiber intensity.
Route of administration
Different forms of the C-21 progesterone (medroxyprogesterone acetate [MPA] and dydrogesterone) or C-19 nortestosterone (norethisterone, lynestrenol, desogestrel and dienogest) have been widely utilized in treatment of endometriosis [6].
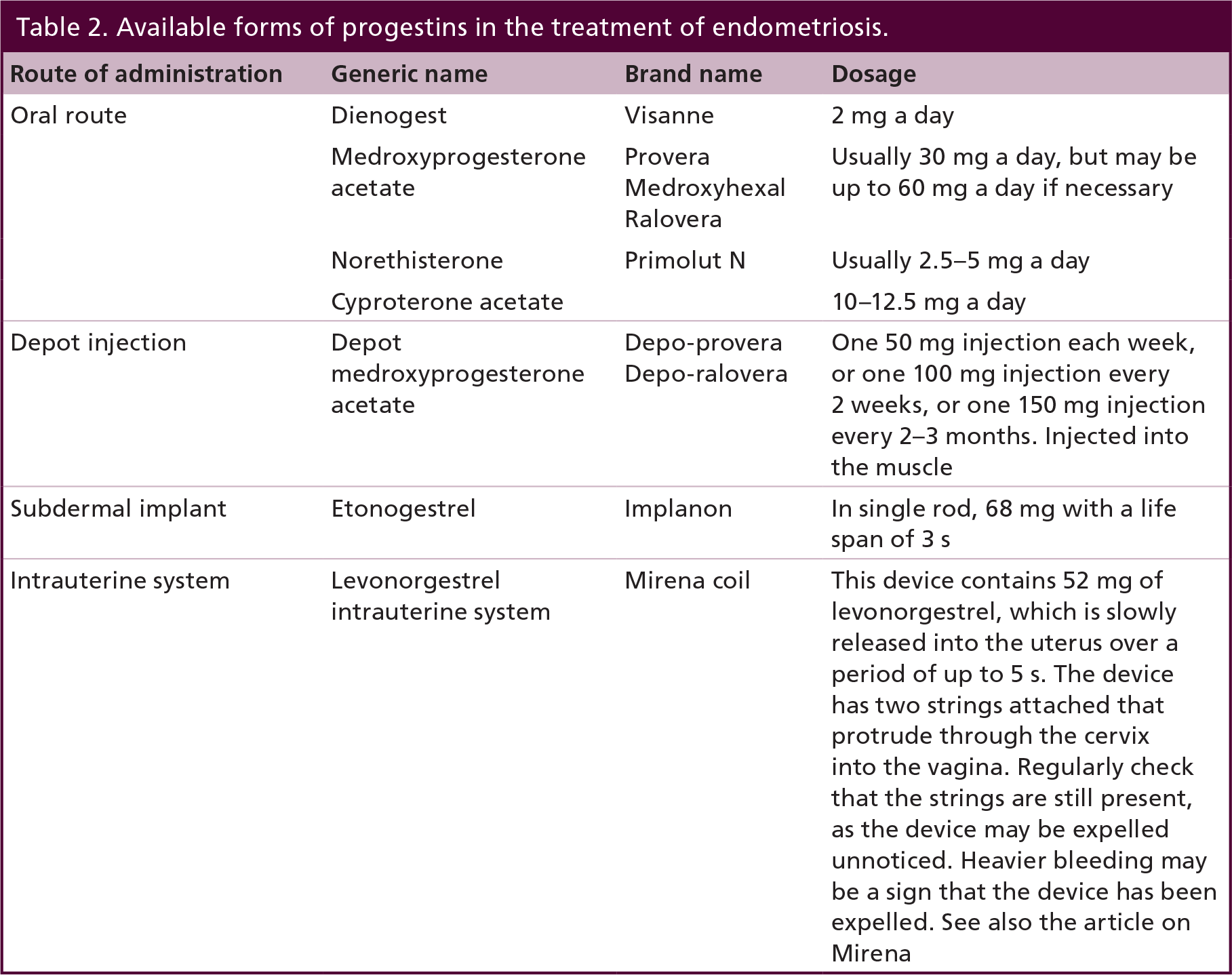
Progestins can be administered as oral preparations, injections, subdermal implants and intrauterine systems (Table 2) [7].
Citing all of the treatment alternatives is beyond the scope of this review but main routes and substances are briefly summarized below.
Oral route
Norethisterone (norethindrone) acetate
NETA is a C-91-nortestesterone derivative. It has been approved for the treatment of endometriosis (2.5 mg daily continuous administration) by FDA. In randomized controlled trials, NETA has been shown to be effective in endometriosis-related pelvic pain [15,16]. The advantages of NETA are control of uterine bleeding, positive effect on calcium metabolism and lack of negative effect on lipoprotein profile [16]. There is also increasing data on the effective use of NETA in rectovaginal endometriosis [7,15].
Medroxyprogesterone acetate
Medroxyprogesterone acetate (MPA) is a C-21-progestogen derivative. It has been studied comparing to placebo and GnRA agonist (Nafarelin) in 15–50 mg doses daily in continuous administration [17]. MPA has been shown to have greater efficacy at alleviating the pain and improving the quality of life against placebo but the effectiveness was found to be equivalent to GnRH agonist [17]. MPA causes breakthrough bleeding in long-term use.
Cyproterone acetate
Cyproterone acetate (CPA) is a C-21-progestogen derivative. It is mainly an anti-androgen with weak progestational activity CPA in 10–12.5 mg daily in continuous administration has been studied comparing to oral contraceptive (desogestrel and ethinyl estradiol) for treatment of endometriosis [18]. Both study groups have been found equally improved due to pain, sexual satisfaction and quality of life after 6 months of treatment [18]. The side effects of CPA are main drawback of its generalized use. It is associated with depression, decreased libido, hot flushes and vaginal dryness.
Dieonogest
Dienogest (DNG) is a C-19-nortestosterone progestogen derivative. It is well tolerated and has an antiandrogenic effect and also a weak antigonadotropic activity. Like the other 19-norprogestins, it enables the suppression of the endometrium in low doses, having a short half-life and high bioavailability. Dienogest is bound to albumin and does not accumulate in oral doses of 2 mg/day.
It has been shown to be effective with good tolerability with doses 2–4 mg daily in continuous administration for 3–24 months in patients with endometriosis [19–26]. DNG has been found to be effective to control endometriosis-related pelvic pain many randomized controlled trials [19–26]. DNG has been compared with GnRH agonists (Buserelin acetate and leuprolide acetate) [25]. DNG has been found to have a lower adverse effect profile. The main side effects were the bleeding problems that were observed in 80% of patients within the first 3 months of treatment, which later on were reduced [25]. It has a good safety and efficacy profile, with a progressive decrease in adverse effects and bleeding irregularities, and the decrease in pain for at least 6 months after cessation of the treatment [26].
Available forms of progestins in the treatment of endometriosis.
Prospective randomized studies that evaluated dienogest 2 mg daily against placebo or versus leuprorelin depot showed a significant improvement in endometriosis-related symptoms with a comparable effectiveness to GnRH agonist treatment [23,24].
Other routes of application
Depot injections
Depot injections of MPA are very effective in suppressing endometriosis-related complaints. Depot MPA (DMPA) has been studied in doses 150 mg intramuscularly or 104 mg subcutaneously in 3 months. It was compared with combination of oral contraceptive with danazol and GnRH agonist (leuprolide acetate) [27,28]. No differences were observed in the reduction of pain symptoms, but demineralization of bone and hypoestrogenism side effects were found in the GnRH agonist group and bleeding problems were frequent in the MPA group. DMPA achieved good pain relief and minimal side effects (bloating and spotting). The optimum interval for administration should be every 3 months.
In long-term use of DMPA, prolonged delay of resumption of ovulation is a major concern in women desiring pregnancy. Therefore, this type of application is recommended only in elderly patients, who do not desire pregnancy. Breakthrough bleeding is an important side effect that interferes with the quality of life. Furthermore, bone demineralization due to hypoestrogenism may be detrimental for the long-term use.
Subdermal implants
A new approach to improve the use of progestins in endometriosis is the development of subcutaneous implants. Subdermal implants (etonogestrel contraceptive implant/Implanon-68 mg in single rod with a life span of 3 years) have been found to be equally effective compared with DMPA in pain relief in 12 months use [29]. It is a safe, well-tolerated alternative for the treatment of endometriosis and achieving long-term contraception.
Intrauterine systems
To reduce the adverse side effects of medical treatments, a new aspect is the intrauterine administration of progestins, which can be an effective treatment of symptomatic endometriosis. The precise mechanism of action of levonorgestrel intrauterine system (LNG-IUS/Mirena-releasing 0.02 mg levonorgestrel/day with a lifespan of 5 years) in the treatment of endometriosis is unclear. However, the patients with pelvic pain due to endometriosis have been shown to be improved after LNG-IUS administration, and antiproliferative effects in the ectopic endometrium have been shown [30].
LNG-IUS was compared with depot GnRH agonist and has been shown to have similar efficacy to control the pain related symptoms [31]. It has also been suggested to be effective against the pain in rectovaginal endometriosis [30]. LNG-IUS has been found to be effective in the treatment of adenomyosis [32]. Main advantages of LNG-IUS are lack of necessity for repeated administrations, institution of highly effective contraception and minimal hypo estrogenic side effects. As the disadvantages, the cost and the probability of unexpected bleeding should be noted. Irregular bleeding during the initial months of application is frequent side effect of the device, but 70% of the women will be amenorrheic in 6 months.
Results for treatment for pain
Observational & retrospective studies
Different progestins at low doses (5–20 mg/day) were studied in mainly retrospective studies with different results. The results, in general, were similar to the results obtained with continuous use of oral contraceptives (estrogen–progestin combination therapy). Symptom improvement reported between 60% and 94% [6,7].
The advantages of progestins are related to the escaping of estrogen-based side effects. The disadvantages are the bleeding problems such as spotting, which can be managed with increasing dosages, adding estrogen or discontinuing the progestin for 5–7 days [7].
Prospective & randomized studies
In a prospective, randomized trial with MPA, regression rate of ectopic implants was reported as 50% and partial regression rate as 13% in the treatment group which was 12 and 6%, respectively, in the placebo group. Pain reduction with MPA was found as effective as danazol [33].
The prospective randomized studies in the literature comparing GnRH analogs with low-dose progestins are limited [16,25,34,35]. Vercellini et al. used a monthly combination of ethinyl estradiol 0.02 mg and desogestrel 0.15 mg versus goserelin 3.6 mg, while Regidor et al. compared daily lynestrenol 5 mg versus monthly leuprorelin 3.7 mg and Strowitzki et al. studied dienogest 2 mg daily versus leuprorelin depot monthly injections [25,34,35].
In a double-blind study, a significant reduction of pain was found during and 1 year after treatment, but there were no difference between the medications used. In the aforementioned study, Vercellini et al. found a significant reduction of deep dyspareunia and cyclic pain in both groups, with goserelin superior to the oral contraceptive [34]. Nonmenstrual pain was diminished in all of the treatments [34]. Utilizing the repeat laparoscopy, Regidor et al. observed a significant reduction of endometriotic implants in the leuprorelin group (r-American Fertility Society score were reduced from 21.8 to 11.5 points with leuprorelin and from 27.2 to 25.5 points with lynestrenol; p < 0.000014 Wilcoxon test). There were no significant improvement of symptoms such as chronic pelvic pain and dyspareunia [35].
In a recent Cochrane review in which 11 RCTs were included, the authors concluded that both continuous progestins (especially continuous high-dose progestin (in the form of MPA) and the antiprogestin, gestrinone are effective therapies for the treatment of painful symptoms associated with endometriosis but there had been no evidence of progestin use, either in oral or depot form, being superior to other types of treatment in endometriosis-related pain symptoms [36]. This conclusion should be treated with caution particularly in light of the absence of suitable placebo-controlled trials.
In conclusion, pain relief established with utilizing acceptable dosages of progestins is indistinguishable with the results of danazol or GnRH analogs. Systematic investigations of various progestins in altered dosages are lacking and there is no conclusive data from prospective randomized placebo-controlled trials up to date.
Patients with rectovaginal endometriosis
In deep-infiltrating rectovaginal endometriosis, the guidelines recommend complete excision but treatment symptomatically with progestin is also possible [6]. In a prospective randomized controlled trial comparing NETA versus a combination of estrogen and CPA, the symptom reduction was proved to be feasible [15]. In both treatment groups, dyschezia, pelvic pain, deep dyspareunia and dysmenorrhea were reduced significantly [15]. A study comparing NETA alone versus NETA combined with an aromatase inhibitor in symptomatic pain relief has confirmed NETA's effects [37]. The positive effect of CPA was also observed in a prospective randomized controlled trial comparing CPA for 6 months versus an oral contraceptive, the quality of life and psychiatric profile improved significantly in the treatment group [18]. LNG-IUS was also proposed to be effective in rectovaginal endometriosis in observational studies [30].
Patients with infertility
The reported rates of pregnancy following progestin treatment (MPA, lynestrenol or norethisterone acetate) vary from 5 to 90% depending on the stage of endometriosis. Lynestrenol 5–10 mg daily was reported with 60% subjective improvement and 5% pregnancy rate. On the contrary, 40% failure and recurrence rate was observed [38].
A distinct potential is projected for dydrogesterone in patients desiring pregnancy since it does not inhibit ovulation. It can be used for symptomatic treatment of pain and for reduction of bleeding problems. The studies utilized dydrogesterone in doses of 10–60 mg/day, for various numbers of days per cycle, and for periods of 3–9 months [39]. The majority of women turned out to be symptom-free or experienced a significant reduction in the symptoms. These outcomes were supported by laparoscopic examination. In addition, cyclic administration of dydrogesterone has also been revealed to establish regular menstruation with reduced blood loss and fewer days of bleeding, combined with exceptional symptomatic relief in dysmenorrhea [39].
All of the publications summarized above are observational or retrospective studies. There is no randomized controlled trial which demonstrated an improvement in fertility after any progestin treatment.
Side effects
The main side effects of progestins can be listed as:
The disturbances of lipid and carbohydrate metabolism and the clotting system, observed more with C-19-derivatives;
Negative influences on mood swings and depression, experienced more with C-17-derivatives.
The individual reactions to the progestins differ depending on the type and dosage of the progestin [40–42].
Levonorgestrel is the cause of spotting, breakthrough bleeding, bloating, weight gain and headache in up to a third of the patients.
Lynestrenol is responsible for the hot flushes, acne and sweating were the main problems in up to 59% of the patients.
MPA use may result with spotting, bloating and weight gain occurred in almost two-thirds of the treated women.
Dienogest is blamed for acne, hot flushes, headache, breast tenderness, loss of libido and fatigue between 10 and 38% of the patients.
Weight gain and bleeding problems with any kind of progestin, are further causes for the cessation of long-term medication [6,7].
Recurrence
Endometriosis is a chronic disease, and progestins as well as other medical treatments do not eradicate the disease. Long-term medication is required to eliminate the symptoms, but no data are currently available for progestin therapy lasting longer than 6–12 months.
There are only a few follow-up studies that have been published concerning the recurrence rates after termination of progestin treatment. These studies reported a quite high rate of symptomatic recurrence especially in the first year following the termination of the treatment. Long-term follow-up propose recurrence rates approximately 50% [1].
Similarly, the data regarding the requirement of surgery for endometriosis subsequent to progestin therapy are limited. The published studies mainly focus on the postsurgery medication with aim to reduce recurrence rates, in particular postsurgical removal of ovarian endometrioma. There were two observational studies showing significant reduction in ovarian endometriotic cyst recurrences following laparoscopic surgery with the use of cyclic, low-dose, monophasic oral contraceptive. In a recent prospective randomized study compared cyclic use of oral contraceptive, continuous use and observation for 2 years after endoscopic cystectomy it was found a significantly lower recurrence rate in continuous (8.2%) and cyclic (14.7%) use of oral contraceptive, compared with 29% in nonusers [43–45].
Conclusion
New effective substances have been introduced for the medical treatment of endometriosis in the last 50 years. Although there have been few studies with limited number of subjects on progestin use in endometriosis, the beneficial effect of progestins for the treatment of endometriosis-related complaints was confirmed.
Progestins are accepted to be one of the major treatment choices in the management of pain and other symptoms related to endometriosis. They are exceptionally useful especially when long-term treatment is indicated and repeated courses of treatment are necessary.
Future perspective
Further studies are essential to reveal the length of treatment, type of progestin, dosage used, intermittent medication and combinations with other drugs, effective in the reduction of endometriosis. Because endometriosis needs a long-term or intermittently repeated medication, and because progestins are relatively well tolerated, having limited metabolic side effects and being inexpensive, there may be more interest in the use of progestins for the treatment of endometriosis-related symptoms in the future.
No writing assistance was utilized in the production of this manuscript.
Executive summary

The most important issue about medical treatment of endometriosis is the alternate treatments are all effective but the symptoms are tending to recur after the discontinuation of the treatment.
First-line medical treatment should focus on the drugs that can be used for long term with minimal adverse effect profile.
The first-line treatment choices are oral contraceptives or oral progestins.
Progestins are available in many forms, including oral preparations, injections, subdermal implants and intrauterine systems.
Different derivatives of the C-21 progesterone (medroxyprogesterone acetate and dydrogesterone) or derivatives of C-19 nortestosterone (norethisterone, lynestrenol, desogestrel and dienogest) have been used in treatment of endometriosis.
Continuous progestins are effective therapies for the treatment of painful symptoms associated with endometriosis but there had been no evidence of progestin use, either in oral or depot form, being superior to other types of treatment in endometriosis-related pain symptoms.
Negative side effects of progestins are disturbances of lipid and carbohydrate metabolism and the clotting system, more seen in C-19-derivatives, as well as negative influences on mood swings and depression, more seen in C-17-derivatives. The individual reactions to the progestins differ depending on the type and dosage of the substance.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.