
Abstract
Chronic pelvic pain (CPP) is common in women of reproductive age and has a significant impact on quality of life, work efficiency and healthcare utilization. CPP can be a manifestation of many different, often multifactorial conditions, and in the absence of an identified cause, the management can be particularly challenging. High quality epidemiological studies would improve the understanding of CPP and identify risk factors which may be targeted for the development of appropriate management strategies. This review focuses on what is known about the prevalence, risk factors, individual and societal burden of CPP and outlines important management strategies.
Chronic pelvic pain (CPP) in women can be an incapacitating condition with a significant impact on health-related quality of life, work efficiency and healthcare utilization [1–4]. Nevertheless, CPP is frequently neglected by healthcare professionals due to lack of clear understanding of the condition and paucity of good quality epidemiological data [4,5]. The etiology of CPP, which involves a complex interplay of physical and psychological factors, is not fully understood and there is no standardized approach to its definition, evaluation and treatment [6]. While CPP could be a symptom of an underlying pathology of various organ systems, it can be argued that it is a syndrome in its own right [7]. This review describes the current epidemiological knowledge of CPP in women, highlights areas for further research and also outlines current management strategies.
Definition
Sound epidemiological research requires an explicit and consistent definition of the health problem being studied. The heterogeneity of the definitions used for CPP introduced challenges for comparing results across different studies [8]. Some definitions include a measure of severity of symptoms. The American Congress of Obstetricians and Gynecologists defines CPP as noncyclical pain in the pelvis, severe enough to require medical attention, located below the umbilicus in the region of the anterior abdominal wall, lumbosacral back or buttocks lasting for at least 6 months [9]. The value of such definitions in epidemiological studies remains debatable, particularly when severity is measured by disability or need for medical attention. Psychological, social and demographic factors could also influence disability and treatment seeking behavior [10–12]. Most population-based epidemiological studies have defined CPP as “cyclical or noncyclical lower abdominal pain of at least 6 months duration, which is unrelated to pregnancy and not exclusively due to dysmenorrhea or dyspareunia” (see Table 1). This definition is consistent with the one adopted by the Royal College of Obstetricians and Gynecologists (RCOG), and is used in this review [13].
Population-based studies of chronic pelvic pain in women.

CPP: Chronic pelvic pain.
Prevalence
A number of studies have reported the prevalence of CPP in women but most of them have used sampling frames such as hospital patients which are unable to provide accurate estimates of the prevalence of CPP in the general population [20–25]. The relatively few population-based studies have reported prevalence ranging from 6.4% in Mexico [16] to 25.4% in New Zealand [3] (see Table 1). The studies were conducted using randomly selected women from representative sampling frames with sample sizes ranging from 1160 [3] to 5263 [1]. It is worth noting that differences in study designs, case definitions and survey methods may have contributed significantly to the variation in reported prevalence rates across different countries.
The earliest population survey for CPP, conducted in the USA in 1994 found a prevalence of 14.7% [1]. Studies from the UK, New Zealand and Australia reported prevalence of 24, 25.4 and 21.5%, respectively [2–3,15]. The prevalence rates in the last three studies were higher than that reported in the first study, possibly because women with mid-cycle pain were excluded from the USA study. Exclusion of women with mid-cycle pain from the UK and New Zealand studies reduced the prevalence rates to 16.9 and 16.5%, respectively. Mexican data obtained in 2005 based on face-to-face interviews of relatively older (25–54 years) women showed a 12-month period prevalence of 6.4% [16], which is the lowest prevalence rate identified, despite the use of a similar definition of CPP as the previous studies.
All the aforementioned studies were conducted among women of reproductive age. Older women who are believed to be less susceptible to CPP have been traditionally excluded from prevalence studies. In 1994, a cross-sectional analysis of a primary care database in the UK found higher rates of CPP in women aged 61–73 compared with women in younger age groups (monthly prevalence of approximately 27/1000 vs 21/1000) [26]. More recent population studies have also confirmed significant reporting of CPP among older women [17–19]. While the highest rate reported in one of the studies was in women aged 18–25 years (17%), women older than 75 years had a rate of 13% [19].
Individual & societal burden
CPP has a considerable impact on the well-being of women and is a cause of significant distress and disability [27]. It has been reported to be associated with poor quality of life, fatigue, depression, anxiety, marital and sexual dysfunction [1–3,14,28–29]. Loss of working days and diminished work capacity were reported by 15 and 45% of affected women, respectively, in a study from the USA [1]. Patients with CPP tended to spend days in bed due to illness and report poorer physical and mental health compared with the general population [30]. In the absence of a specific diagnosis, women often experience despair, lose personal confidence, become increasingly isolated and may even be suicidal [31].
Influences of psychological factors on the experience of pain are also important. Generally, quality of life in chronic pain has been shown to be considerably associated with beliefs about pain than the pain intensity [32]. A prospective study of 115 women with endometriosis-associated CPP showed that catastrophizing (i.e., negative cognitive and emotional coping response including amplification of pain and feeling of helplessness) had a significant impact on the experience of pain [33]. A cross-sectional study showed that a diagnosis of endometriosis did not influence quality of life or anxiety-depression symptoms in women with CPP but higher pain intensity was associated with lower quality of life [34]. Similarly, post-traumatic stress disorder has been found to be related to poor health status in women with CPP [35].
The majority of women with CPP do not seek medical advice. A study in the UK in 2001 showed that only 32% of women with CPP had sought medical advice in the past year (recent consulters), 41% had never done so (nonconsulters) while about 27% had sought medical help early, but not within the past year (past consulters) [36]. This study also found that while recent consulters had more severe symptoms, all were affected by their pain and many, including nonconsulters, remained anxious about the cause of their pain. Forty-three per cent of past consulters reported that their activities were restricted by their pain. It is not clear why women do not seek medical help or discontinue contact with their healthcare providers despite the persistence of their symptoms. The authors suggested that the reason for this could either be because women continue to favor self-medication or because they are dissatisfied with the treatment provided [36]. These suggestions are supported in other studies. A study showed that 58.4% of women with CPP reported that they use analgesics and/or nonsteroidal anti-inflammatory drugs on a weekly or daily basis without medical prescription [18].
Furthermore, a focus group study involving a total of 36 women in New Zealand reported that many of the women seeking medical input from General Practitioners and/or gynecologists experienced problems with their consultations [37]. These problems include difficulties with communication with the healthcare provider, diagnosis, diagnostic procedure, referral, medication and surgery. Another study also reported problems with the doctor–patient relationship mainly due to communication problems which led to women feeling devalued and dejected and unwilling to reengage with the consultation process despite the persistence of their pain [38]. The studies highlighted the need for healthcare providers to develop communication strategies, so that the patients do not feel that their symptoms are dismissed. Improved communication skills are also fundamental for providing the patient with sufficient information about diagnosis and treatment options to ensure that the patients are involved in making informed decisions and are considered as equal partners in their care. A study of primary care practitioners’ perspectives showed a lack of awareness of how the condition should be diagnosed and treated which also threatens the practitioners’ perceptions of their own clinical competencies [39]. Additional education and training is needed for primary care practitioners to effectively prepare them in helping women with CPP.
CPP accounts for about 40% of gynecological laparoscopies, making it the most frequent indication for referral to women's health services [40]. Unsurprisingly, it has major financial implications. In the UK, care for women with pelvic pain was estimated to cost the National Health Service (NHS) more than $$158 million in 1992 [41]. The equivalent cost today is estimated at approximately $326 million based on the inflation indices from the hospital and community services index [42]. In the USA, the total annual direct cost for physician visits and out-of-pocket cost was estimated to be USD$2.8 billion in 1996 [1]. This is equivalent to USD$5.68 billion today according to the figures in the medical care component of the Consumer Price Index [43]. A study found that loss of work productivity in endometriosis was majorly driven by pelvic pain and disease severity [44]. This work productivity loss translated into substantial cost per woman per week ranging from USD$4 in Nigeria to USD$456 in Italy [44].
Etiology & risk factors
Prospective cohort studies which allow exploration of the temporal relationship between a risk factor and a disease are ideal for identifying factors responsible for CPP. As such studies are expensive and time consuming, the majority of the risk factors for CPP reported in the literature are derived from cross-sectional studies. Due to variations in health seeking behavior and referral patterns, risk factors identified from primary or secondary/tertiary care settings may differ from those identified in the community setting [45].
Underlying etiology of CPP has been described in various literatures [27,46–48]. CPP can be a manifestation of urological, gastrointestinal, musculoskeletal, gynecological, neurological and psychosocial conditions with often more than one contributory factor and a range of diverse risk factors
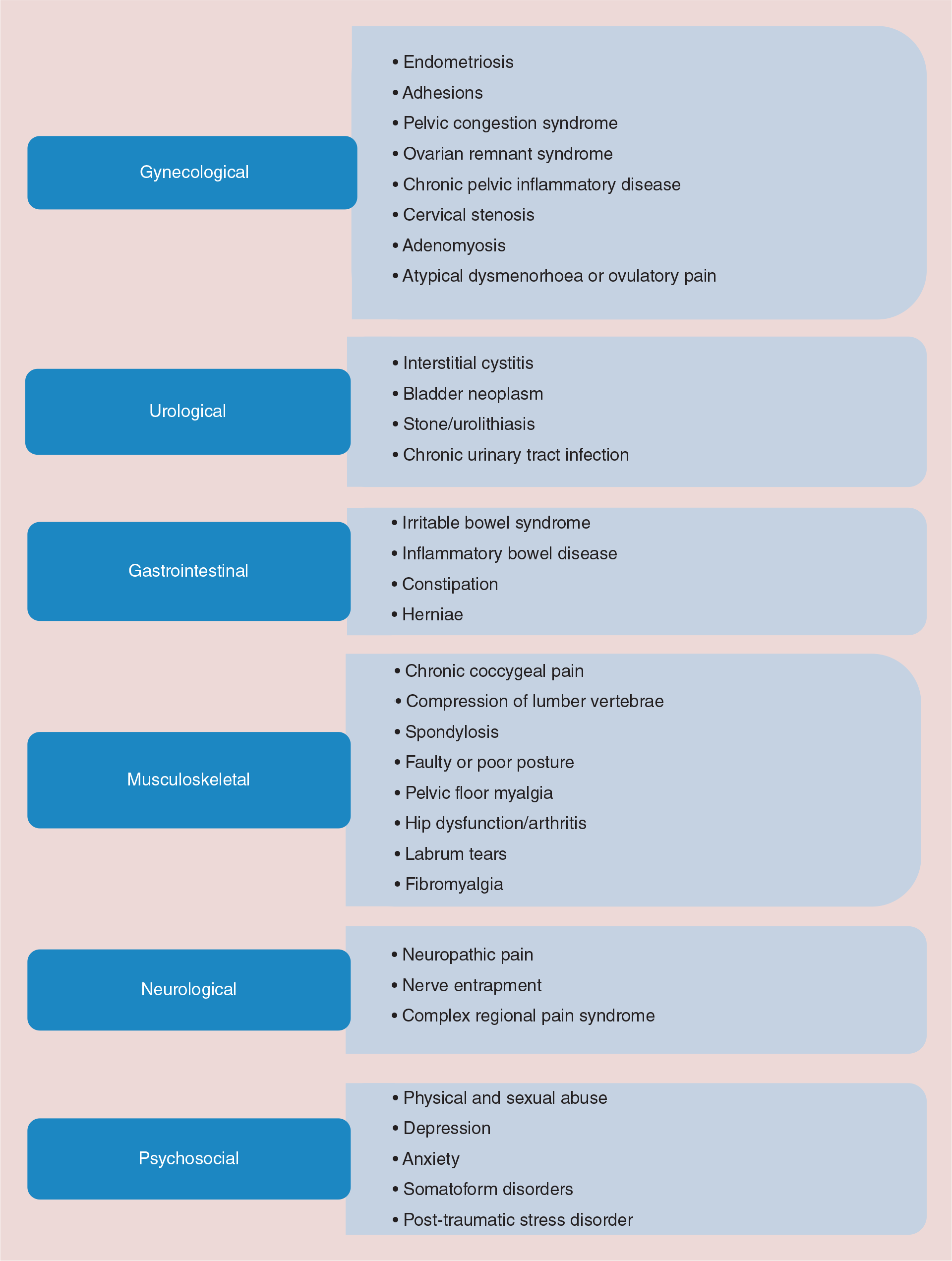
Examples of conditions that may be associated with chronic pelvic pain in women.
Traditionally, clinicians often sought to identify a visceral origin of CPP while musculoskeletal sources were frequently overlooked [49]. In a cross-sectional study, abnormal pelvic musculoskeletal findings were significantly more common among women with CPP compared with healthy women [50]. These musculoskeletal findings included higher pelvic floor tenderness scores (3/24 vs 0/24), poor control of pelvic floor (78 vs 20%), pelvic girdle instability (asymmetric iliac crest [61 vs 25%], pubic symphysis heights [50 vs %], positive posterior pelvic provocation testing [37 vs 5%]) [50]. Another study found that when compared with healthy controls, women with CPP had more postural changes in the cervical spine (odds ratio [OR]: 4.1; 95% CI: 1.6–10.7) and the scapulae (OR: 2.9; 95% CI: 1.1–7.6) [51]. Thus, musculoskeletal conditions among women with CPP are common and need to be more recognized.
CPP may also be neuropathic (pain resulting from nerve damage) or of mixed origin. Neuropathic pain has been defined by the Special Interest Group on Neuropathic Pain of the International Association for the Study of Pain as “pain arising as a direct consequence of a lesion or disease affecting the somatosensory system” [52]. This suggests that neuropathic pain can originate from a lesion of either the peripheral or the CNS [53]. Neurological pain may be a result of a wider neurological disorder or secondary to nerve entrapment in scar tissue or fascia following surgery resulting in pain along the distribution of nerve [54]. CPP, like many other chronic pain conditions, involves significant changes in the CNS [55,56]. Such changes may lead to hyperalgesia (heightened awareness of pain) or allodynia (pain in response to stimuli that does not normally provoke pain) [56]. Evidence supporting neuropathic features (including symptoms like burning, tingling and pins and needles) in some CPP cases is increasing. In a study using the Self-Administered Leeds Assessment of Neuropathic Symptoms and Signs (S-LANSS) as a screening tool, 31% incidence of neuropathic pain was reported among a sample of 142 CPP patients (both men and women) visiting two tertiary referral centers [57]. Poorer quality of life was reported by those with neuropathic pain symptoms compared with those without. Unfortunately, outcomes relating to women with CPP were not reported separately. Higher pain intensity, rates of co-morbid conditions and impact on daily life have been reported among participants who have chronic pain with neuropathic features compared with those with non-neuropathic features [58,59]. These highlight the importance of considering chronic pain with neuropathic symptoms and those without neuropathic symptoms separately.
Psychological factors are also important risk factors for CPP. A meta-analysis revealed that the majority of the strong correlates identified were within the abuse/psychological factors domain (particularly psychosomatic symptoms, depression, anxiety, physical and sexual abuse) when compared with obstetric, gynecological, environmental and demographic factors [60]. Other risk factors for CPP include previous caesarean section and previous pelvic trauma [19,61]. A significant overlap between CPP, dysmenorrhea and dyspareunia has been reported in various population-based studies. For instance, about 80% of women with CPP also reported dysmenorrhea and/or dyspareunia in the UK, New Zealand and Australian studies [2–3,15]. A study reported that those who report CPP were about four-times more likely to also report dyspareunia and about two-times more likely to report dysmenorrhea [18].
There is no clear pattern of association of CPP with socio-demographic factors. A lower risk was reported in non-Caucasian women compared with Caucasian women in the UK (OR: 0.4; 95% CI: 0.2–0.8) and USA (OR: 0.7; 95% CI: 0.5–0.95) [1,2]. The prevalence of CPP has been reported to vary across age groups, although the patterns were inconsistent [1–3,15]. Compared to single women, women who were divorced, separated or widowed were more likely to report CPP in one population-based study (OR: 1.51; 95% CI: 1.12–2.04) [1] but not in some others [2–3,16]. In New Zealand, CPP was more common in women with higher qualifications (33.0%) than in women with school qualifications (21.5%) or no qualifications (23.2%) (p = 0.02) [3]. However, CPP was associated with low educational level in another study in Brazil [17]. There was no significant association found between education level and the risk of reporting CPP in some other studies [1,15,18]. CPP was also not significantly associated with employment status or social class [2,3,18].
Diagnosis & management
An in-depth description of diagnosis and management strategies for CPP is beyond the scope of this review. Current approach to initial assessment and management of CPP is discussed below.
As mentioned earlier, some of the conditions manifesting as CPP have overlapping symptoms, thus initiating appropriate investigations to identify the cause of CPP can be challenging. The diffuse nature of pain can make it difficult to localize its origin, adding to the complexity of diagnosis [62]. Laparoscopy is unable to identify an obvious cause for pain in about half of all women with CPP [63]. An initial history and clinical examination can help to select appropriate strategies for investigation, initiation of treatment or referral to an appropriate specialty. Professional bodies representing various clinical specialties have published guidelines on the management of CPP [9,13,64–66]. A multidisciplinary approach is frequently recommended, where a team of specialists including physiotherapists, psychologists, gynecologists and pain physicians are involved in the care of the patient. It is vital that a single clinician orchestrates the multidisciplinary team to streamline and individualize care. This minimizes the risk of women being seen and given potentially conflicting advice from multiple specialists.
The high disease burden, wide variations in care and uncertainty regarding the evidence base underpinning some of the interventions have led to the development of an integrated care pathway by the Map of Medicine and British Pain Society (BPS) [6,66]. The BPS pathway and the RCOG provide comprehensive guidance that focuses on a holistic approach (i.e., management which takes into account the biological, psychological and social aspects of the person) with initiation of treatment in primary care and timelines for onward referral to secondary and tertiary care. The BPS pathway has divided CPP into two distinct entities; CPP where an organic cause can be attributed needs to be distinguished from CPP syndrome where no obvious pathology is identified. CPP syndrome may exist as a part of a multisystem disorder with complex interactions of psychosocial, behavioral and sexual factors. A caveat with CPP is that pelvic pathology may co-exist with CPP syndrome. At the initial visit, an in-depth history of physical, social, psychological, sexual factors and fertility desires should be sought accompanied by general physical and pelvic examination. The identification of any ‘red flag’ symptoms such as postcoital or postmenopausal bleeding, bleeding in stools, large pelvic mass, hematuria or signs of major depressive disorder should prompt urgent referral to secondary care to exclude any sinister pathology [66]. Appropriate investigations should then be instituted to confirm or refute these clinical findings.
Common gynecological pathologies which can present with CPP include endometriosis, adenomyosis, ovarian cysts and also sexually transmitted infections. Noninvasive investigations such as pelvic swabs, ultrasound or magnetic resonance imaging can identify sexually transmitted infections (such as uncomplicated lower genital tract chlamydia and gonorrhea), PID, ovarian cysts and adenomyosis. In women who do not wish to conceive, empirical treatment with hormonal preparations can be commenced in primary or secondary care before embarking on laparoscopy to exclude endometriosis. Previously considered to be a gold standard in evaluating CPP, laparoscopy is now seen more as a second line intervention when other therapeutic measures fail [13]. Endometriosis may be treated laparoscopically by excision or ablation. It is a condition prone to recurrence and often medical hormonal suppressive treatment is prescribed to reduce the risk of recurrence. Any endometriotic or nonendometriotic ovarian cysts can be treated during laparoscopy by cystectomy or oophorectomy depending on the age of the woman, nature of the cyst and future fertility intentions. Laparoscopy also permits identification and division of adhesions and drainage of tubo-ovarian abscesses that may occur secondary to PID. Pelvic pain may be the long term sequela of PID. Hence, a low threshold for empirical treatment of PID is recommended using broad spectrum antibiotics [67]. Dyspareunia as a symptom is more complex. Previous sexual experiences, abuse, termination of pregnancy and other psychosocial factors can have a disproportionate influence on the experience of dyspareunia especially when associated with vaginismus. These factors should be explored during initial assessment and role of psychosexual counseling considered in selected cases.
Gastrointestinal conditions like inflammatory bowel disease or IBS may cause or contribute to the pelvic pain symptom complex. IBS is a chronic functional bowel disorder characterized by abdominal pain or discomfort and associated with bowel dysfunction. It can be reliably diagnosed using the Rome III criteria [68,69]. An improvement in symptoms can be achieved by a combination of dietary modifications and pharmacological therapy.
With bladder pain syndrome or interstitial cystitis, there is an increased association with other coexisting conditions like IBS, fibromyalgia and chronic fatigue syndrome [70,71]. The history may point toward lower urinary tract symptoms of pain, pressure or discomfort associated with urinary frequency, urgency and pain that improves after voiding. Cystoscopy and/or biopsy may be required in selected cases. Cystoscopy can be combined with laparoscopy as interstitial cystitis and endometriosis are often considered as the ‘evil twins’ of CPP in women [72]. Interstitial cystitis/bladder pain syndrome is difficult to treat. The American Urological Association recently published updated guidance for management ranging from first line to sixth line treatments [73]. A multimodal management strategy using pharmacological, manual therapy and stress management is advocated. Pharmacological treatments include use of amitryptiline, cimetidine, hydroxyzine or pentosan polysulphate orally. Alternatively, intravesical instillation of various agents, cystoscopy and cystodistension may be considered.
Pain of musculoskeletal origin arising from pelvic joints or pelvic floor muscles could be attributed to CPP. Pelvic examination should include palpation of pelvic floor muscles for any trigger points or tender areas. It is unclear whether these musculoskeletal anomalies are the primary cause of pain or secondary phenomenon elicited by poor posture associated with CPP [13,73]. Levator ani spasms, ilio-psoas complex pain and pain arising from piriformis or obturator muscles may present as pelvic pressure, midvaginal dyspareunia, pain shooting down the leg or groin pain. The mainstay of treatment for musculoskeletal pelvic pain is physiotherapy by trained professionals. Muscle relaxants and botulin may sometimes be used [47].
Some women, especially those who have undergone multiple pelvic surgeries but still continue to have pain, may be experiencing neuropathic pain [54]. Recognizing patients with CPP whose symptoms are suggestive of neuropathic components could help healthcare providers plan the most suitable management strategy and prevent inappropriate surgery. Diagnosis and management of various peripheral neuropathies that may cause CPP have been previously described [54]. Assessment tools are available to distinguish whether pain is nociceptive or of a possible neuropathic origin [74–78]. Neuromodulating agents such as tricyclic antidepressants or anticonvulsants are often used for treating the neuropathic component of the CPP [57]. Initial reports on the use of gabapentin for CPP are promising [79]. Further studies to evaluate the use of gabapentin for CPP are underway [80].
Psychological disorders like anxiety, depression and sleep disorders are common in women with chronic pain conditions but it is difficult to ascertain whether these are a consequence of, or contributory to, the experience of pain. Sexual issues associated with CPP can have a debilitating effect on relationships and self-esteem. As a part of multidisciplinary team, pain psychologists and psychosexual counselors can help address the influence of these factors on perception of pain and quality of life.
This review emphasizes the need to acknowledge the multifactorial nature of CPP. The diagnosis of ‘CPP syndrome’ should be reserved for women in whom a thorough evaluation has been performed to exclude any treatable pathology. Referral to regional pain management centers and pain management programs may be required for refractory cases. Pain management programs comprise methods to promote behavior change and consequent well-being by educating women on pain physiology, pain psychology, general health and self-management of pain [81]. Complex cases warrant an individual case management approach with interdisciplinary and multispecialty assessment. The entire concept of CPP management reflects a shift in para digm. There is a move from assigning causality to recognizing CPP in its totality with management focusing on multidisciplinary input, educating and empowering women and working in partnership with them.
Conclusion
CPP is a disabling condition, often without an obvious identifiable cause. This poses a major challenge for patients, clinicians and researchers. Clinicians often approach CPP from the perspective of their own specialty but it is best managed through a holistic multidisciplinary approach working closely in partnership with women. The epidemiological characteristics of CPP need to be further established to enable in-depth understanding of the burden of CPP in the general population and individuals. This requires accurate ascertainment of the prevalence of CPP and associated risk factors. Understanding the factors that influence how women are affected by CPP is an essential step toward developing and evaluating effective management strategies.
Future perspective
Our understanding of CPP will improve as the syndrome continues to attract more research interest. Epidemiological studies, which have traditionally focused on women of childbearing age, are increasingly including older women. This is likely to improve our understanding of the etiology of CPP – especially factors such as hernias, spondylosis, constipation and pelvic floor dysfunction, which are common at older age. This will also aid comparison of CPP studies with other chronic pain conditions to help us appreciate the similarities between CPP and other regional pain syndromes because epidemiological studies of other regional pain syndromes have shown strong similarities in etiology, irrespective of the site of pain. Prospective studies are important for identifying etiology but in order to recruit subjects prior to onset of CPP they need to be recruited at young ages and long-term follow-up is required. Newer epidemiological study designs, such as case-crossover studies, particularly focused on studying episodes of pain rather than first onset, may be more feasible.
While CPP, like other chronic illnesses, may cause anxiety and depression, a number of studies have suggested that such psychosocial factors can actually predict the onset of various pain symptoms [82–88]. Prospective studies are needed to help determine temporal relationships between these factors and CPP. Prospective data would also help to improve the understanding of the natural history of CPP in women especially in cases where no known cause is identified.
To our knowledge, no population-based study has aimed to identify women who have CPP with neuropathic pain features, and consequently the true prevalence of neuropathic symptoms among women with CPP is yet to be known. There may be a need for a tool to be developed and validated specifically for the identification of pelvic pain with neuropathic features in the near future. Such tool may become a useful component of CPP evaluation.
Executive summary
Definitions of CPP are mostly based on the duration and localization of pain.
Most frequent definition used in research is “cyclical or noncyclical lower abdominal pain of at least 6 months duration, which is unrelated to pregnancy and not due exclusively to dysmenorrhea or dyspareunia.”
Prevalence ranges from 6.4 to 25.4% in different countries.
Variation in prevalence is influenced by study design and case definitions.
Most population-based studies determining prevalence have been limited to women in their reproductive years.
Poor quality of life.
Psychosocial distress, marital problems and sexual dysfunction.
Significant economic burden, including direct and indirect costs as well as loss of working time from paid work.
Etiology and risk factors for CPP are not fully understood.
CPP may be a manifestation of one or more disorders of various organ systems and also involves psychosocial conditions.
More epidemiological studies are needed to identify etiological and risk factors for CPP. Diagnosis & management
Specific diagnosis made in only about half of CPP cases.
Management is challenging and a multidisciplinary approach to the management of CPP is highly recommended, particularly when no particular cause is identified and when pain persists even after the underlying pathologies have been treated.
Treatment should be directed at underlying cause of CPP if any is found.
The management of CPP can be particularly challenging for healthcare providers as well as patients. Unfortunately, many reviews of management strategies for CPP have shown that there is a paucity of evidence-based options, making it more difficult for both parties to make informed decisions [89–91]. More clinical trials are necessary to evaluate medical, lifestyle and psychological interventions for CPP [90]. It would be important for studies to evaluate the effectiveness of chronic pain management strategies which have been shown to be beneficial for other chronic pain syndromes but have not been extensively evaluated for the management of CPP in women. For example, cognitive interventions and exercise used for several chronic pain conditions including: fibromyalgia, chronic low back pain and other widespread/regional pain conditions [92,93]. In the meantime, multidisciplinary care for patients with CPP, especially where no known cause is identified, should be promoted.
Footnotes
AA Ayorinde holds a funded PhD studentship at the University of Aberdeen. GJ Macfarlane is a member of Pfizer's Inflammation Competitive Research Programme (I-CRP) grant awarding panel for which he receives an honorarium. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.