
Abstract
Maternal cardiac disease is a very significant cause of both maternal morbidity and mortality in westernized countries. An effective treatment program must tackle all of the contributing components, including those due to public health issues, poorly coordinated healthcare systems and inadequate medical education. Even with optimal care, many of these patients remain at high risk. In this setting, it is the role of the multidisciplinary team to counsel women regarding these risks and to proactively institute treatment algorithms that will optimize maternal and fetal outcomes.
 Medical Education Online
Medical Education Online
This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of Medscape, LLC and Future Medicine Ltd. Medscape, LLC is accredited by the ACCME to provide continuing medical education for physicians.
Medscape, LLC designates this Journal-based CME activity for a maximum of 1
All other clinicians completing this activity will be issued a certificate of participation. To participate in this journal CME activity: (1) review the learning objectives and author disclosures; (2) study the education content; (3) take the post-test with a 70% minimum passing score and complete the evaluation at www.medscape.org/journal/wh; (4) view/print certificate.
Learning objectives
Upon completion of this activity, participants should be able to:
Distinguish the type of cardiac disease responsible for the most morbidity during pregnancy
Analyze the diagnosis and management of ischemic heart disease during pregnancy
Evaluate best practices regarding the management of aortopathies during pregnancy
Assess the clinical impact and management of arrhythmias and valvular heart disease in pregnancy
Financial & competing interests disclosure
CME Author
Authors & Credentials
Editor
The importance of maternal cardiac disease in pregnancy is well recognized. Concern regarding this has, by and large, focused on data regarding maternal mortality and its recent increase in westernized countries [1]. Despite being the most common cause of maternal death in the UK, deaths due to heart disease are still rare, with only 53 deaths in the last 3 years covered by a maternal confidential enquiry (2006–2008) [2]. However, mortality is only the tip of a large iceberg of morbidity. The study of this morbidity and of ‘near-miss’ events reveals a more comprehensive picture of ongoing cardiovascular pathology and psychological disability, as well as highlighting the societal impact of this issue. The aim of effective treatment of cardiac disease in pregnancy must be to address all of these components.
One of the most informative studies of cardiac morbidity in pregnancy comes from a national cohort study in The Netherlands (the LEMMoN study) [3]. This is a registry covering all of the country's 98 maternity units that serve a population of 17 million. As well as documenting maternal cardiac deaths, the investigators report on all cardiovascular events that are significant enough to trigger admission to hospital. This study again demonstrates that maternal cardiac death is rare (three deaths per 100,000 deliveries). The equivalent rate of significant morbidity was 23 per 100,000 deliveries, giving a case–fatality rate of 13%. The most common causes of maternal cardiovascular morbidity were ischemic heart disease, cardiomyopathy, arrhythmia, valve disease and aortic dissection (Figure 1).

Maternal cardiac morbidity and mortality per 100,000 deliveries.
Pregnancy is a challenge to even a healthy cardiovascular system. There are significant changes in circulating volumes, arterial resistances and the heart rate, as well as structural changes in both the heart and great vessels [4,5]. These adaptive changes to pregnancy can become maladaptive in a compromised circulation. Superimposed are the risk of bleeding and thrombosis and a myriad of iatrogenic challenges, such as surgical procedures and the use of drug therapies. A barrier to optimal care has been the misconception that a young woman of child-bearing years must be healthy, rather than perceiving pregnancy as being a time of increased risk.
When describing the best treatment pathways for women, two distinct groups should be considered: those with known heart disease prior to pregnancy and those with a new cardiac diagnosis during pregnancy.
Pregnancy in women with known heart disease
By definition, these are the women that fill the specialist cardiac disease and pregnancy clinics. The majority of these women will have congenital heart disease, rhythm disorders or degrees of ventricular dysfunction. The aim of excellent care is to proactively discuss pregnancy with all women who have known heart disease who are of child-bearing age, including ‘older’ women contemplating assisted fertility techniques. Unfortunately, not all of these women are given specialist support prior to considering a pregnancy. At times, advice is given by nonspecialists that is either vague (e.g., “You should be alright”) or actively unhelpful (e.g., suggesting high-risk women should not be taking the combined pill, but not identifying any effective alternative methods of contraception). The aim of prepregnancy counseling is to empower women to make informed choices about their plans to have a family and to attempt to optimize both maternal and fetal outcomes. Risk stratification will be based on the nature of the underlying condition, the current hemodynamic status, the functional capacity of the patient and a preconception history of cardiac events. Several risk-scoring systems have been developed in order to further communicate the risk of an adverse outcome. Two of the most common are the Cardiac Disease in Pregnancy Score (Box 1) [6] and the ZAHARA study score [7]. Although these patients form the majority of patients attending specialist cardiac and pregnancy clinics, they are not the majority of patients who develop life-threatening or fatal cardiac complications in pregnancy (Figure 2) [8].
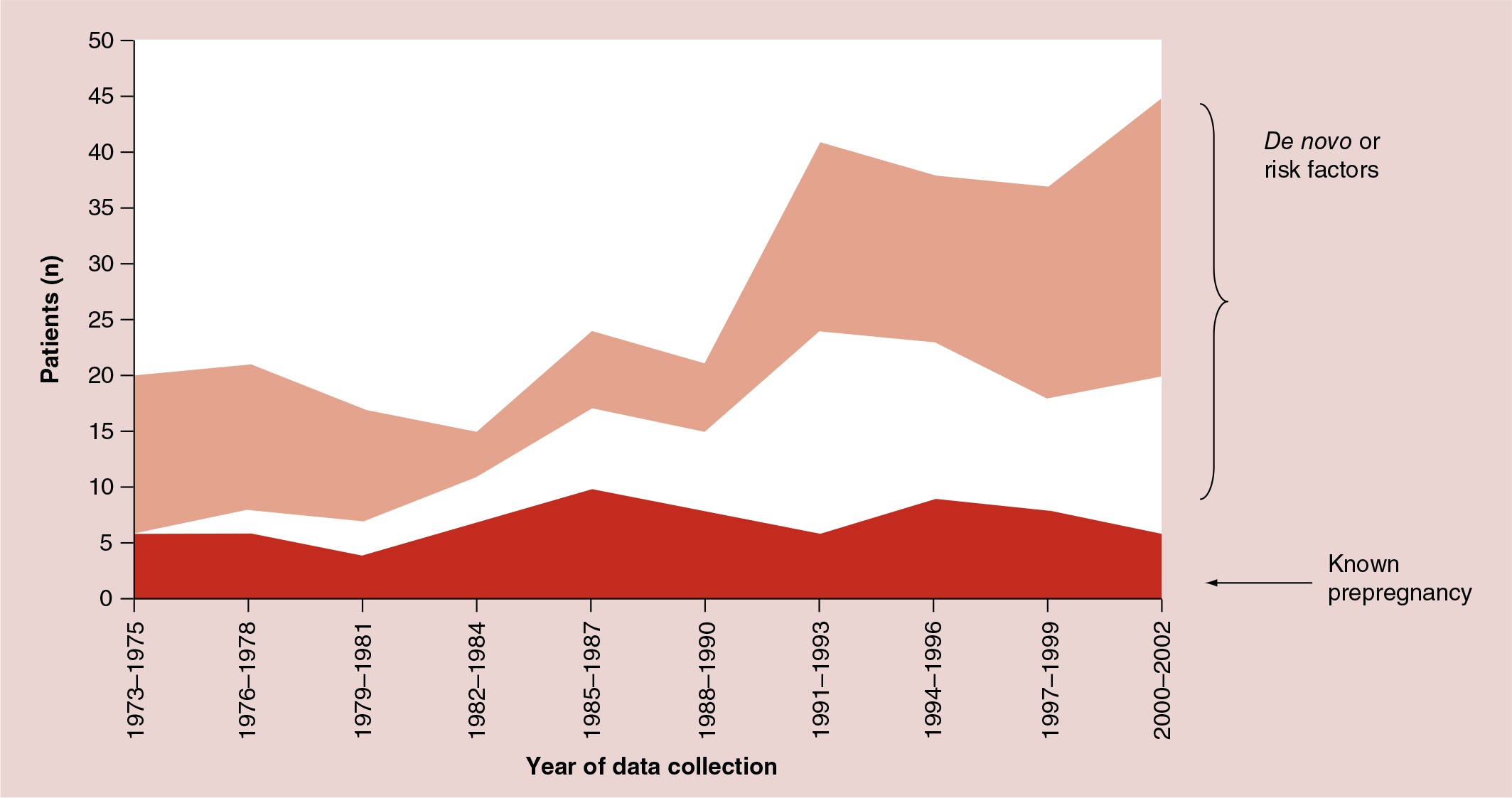
Maternal deaths in the UK due to cardiac disease.
Newly diagnosed cardiac disease in pregnancy
The majority of women who die from cardiac disease in pregnancy are not known to have heart disease before they present as acutely unwell. They were, therefore, not able to access any preconception counseling or have any therapeutic interventions in order to minimize risk. The Netherlands registry estimated that two-thirds of women with significant morbidity were not known to have cardiac disease prior to pregnancy [7]. This group includes those with undiagnosed pre-existing disorders, such as congenital heart disease (Figure 3), valve lesions and Marfan syndrome, as well as those with newly developing issues, such as new arrhythmia, peripartum cardiomyopathy and acute ischemia. The key for the optimal treatment of these patients is rapid diagnosis and access to specialist care. In this context, pregnancy should be identified as a reason for aggressive care and not as an excuse for only partial investigation or treatment.

Ischemic heart disease
Acute coronary ischemic events formed 20% of the morbidity in the Dutch registry and 6% of the mortality [7]. It is estimated that these events complicate five to six deliveries per every 100,000, and it is thought that pregnancy itself increases the risk of an acute coronary event by a factor of three- to four-times. This risk is particularly true for women over the age of 40 years. The majority of these women have identifiable cardiac risk factors, including hypertension, diabetes, smoking, obesity and thrombophilias [2]. The increasing incidence of coronary events in pregnancy reflects the changing demographics of pregnancy, with an increase in the numbers of older mothers and those with elevated BMI values. This is a recognized phenomenon in the west that is rapidly spreading to other less-developed nations [9,10].
The diagnosis of acute ischemia is the same as for nonpregnant patients, using the key components of clinical history, ECG changes and elevated cardiac enzymes (e.g., troponin). Pregnancy can lead to ECG changes with variations in the QRS axis and subtle ST shifts, but any ECG changes should be carefully considered before being dismissed as normal for pregnancy. Importantly, the cardiac enzyme troponin does not change throughout pregnancy (unless complicated by pre-eclampsia) and patients with troponin-positive chest pain should normally undergo invasive assessment with coronary angiography. Close liaison between the obstetrician and cardiologist will be necessary, but percutaneous coronary intervention (PCI) can be performed safely and effectively, ideally from the radial route, with techniques to minimize fetal radiation exposure [11].
The use of drug-eluting stents will require the patient to be on dual antiplatelet therapy and, therefore, if within a few months of the estimated delivery date, bare-metal stents may be preferable. Aspirin and clopidogrel can be used in pregnancy, but both will significantly increase the risk of obstetric hemorrhage. Thrombolysis is a less attractive option than PCI for acute infarction, but it can be used if there is no alternative available. The complication rate of major obstetric bleeding is difficult to determine and will relate to gestation and proximity to delivery.
It is extremely unusual for a pregnant patient to present with an acute coronary syndrome that is not amenable to PCI, but in these rare occasions, unstable patients should be offered cardiac bypass grafting with techniques to minimize the impact of cardiopulmonary bypass on the fetus. Even with these maneuvers (avoiding hypothermia and hypotension), the risk of fetal loss is approximately 30% [12]. Currently, many coronary artery bypass grafts can be performed off-bypass, which varies between centers. Although there are a few case reports published in the literature demonstrating a good outcome in patients undergoing off-bypass surgery during pregnancy [13], this is still a high risk for the fetus. If the gestation allows, delivery before cardiac surgery is preferable.
Predictors of maternal cardiovascular events.
Prior cardiac event (e.g., heart failure, transient ischemic attack, stroke before pregnancy or arrhythmia; score: 1 point if present)
Baseline NYHA functional class >II or cyanosis (score: 1 point if present)
Left heart obstruction (i.e., mitral valve area <2 cm2, aortic valve area <1.5 cm2 or peak LVOT gradient >30 mmHg; score: 1 point if present)
Reduced systemic ventricular systolic function (ejection fraction <40%; score: 1 point if present)
0 points: 5%
1 point: 27%
>1 point: 75%
Assessing patients with possible stable angina can be difficult in pregnancy. Functional tests either involve some form of exercise testing or the use of compounds (e.g., radioactive isotopes or gadolinium) that may present risks to the fetus. A practical solution is the use of the clinical history, risk-factor profile and exercise stress echo in order to risk stratify patients. There should be a low threshold for invasive angiography in those deemed to be at risk, with the option of proceeding to PCI at the same sitting. Computed tomography (CT) coronary angiography is a useful tool for delineating the coronary anatomy, but this also exposes the fetus to the risks of radiation exposure, and invasive angiography may still be required if the CT is equivocal or abnormal. The medical treatment for ischemia should include aspirin and β-blockers. Nitrates and certain calcium channel blockers may also be useful, but statins should be avoided until after delivery. There are few safety data regarding nicorandil and ivabradine, but if the patient is requiring multiple antianginal agents, an invasive strategy is preferable.
Only occasionally will women with known coronary disease present for preconception counseling. In this settling, the key components are whether there is a persisting ischemic burden or whether there is important left ventricular dysfunction. Further risk stratification can be simply performed utilizing a functional test (e.g., an exercise test, myocardial perfusion scan, cardiac magnetic resonance perfusion imaging or stress echo) and an assessment of the ejection fraction (e.g., echo or MRI). Prior to pregnancy, cardiac function should be optimized and plans made for the withdrawal of teratogenic drugs.
Kawasaki disease is one of the most common vasculitic diseases of childhood. It is known that coronary artery aneurysms develop in 15–25% of untreated children with Kawasaki disease; however, in the current era, where early intravenous immunoglobulin is the standard therapy, the number of patients who develop coronary artery aneurysms has fallen to 2–6%, the vast majority of which are transient small aneurysms [14]. Although there are only few data, it seems that pregnancy in Kawasaki disease patients is not associated with increased risk [15]. However, mothers with persistent giant coronary artery aneurysms (>6 mm) should be treated with low-molecular-weight heparin and low-dose aspirin during the pregnancy [15].
Women with cardiovascular risk factors
There is much discussion regarding the increasing prevalence of cardiovascular risk factors in women contemplating pregnancy, and this remains an important public health issue. When considering an individual asymptomatic woman at booking (and these patients may form a reasonably sizable proportion of the antenatal population), there is little to be gained by complex cardiac investigations. Women should be encouraged to minimize their risk factors (e.g., to give up smoking or to optimize blood glucose control). They should also be warned about the symptoms of coronary ischemia and the tests they should have if they develop significant chest pain. There are no data to recommend routine medical intervention in this population. Unfortunately, these women will represent a sizable proportion of the antenatal clinical population in the years to come. There remains an important public health message to disseminate that women should optimize their physical fitness prior to pregnancy in order to give the best chance of having a healthy outcome.
Aortopathies & aortic dissection
Although rare in pregnancy, aortic dissection is the maternal cardiac condition with the highest case–fatality rate, in that over 80% of woman presenting with a dissection in pregnancy will die. Pregnancy
The majority of women who present with a dissection will have an underlying aortopathy, such as Marfan syndrome, Loeys–Dietz syndrome or vascular Ehlers–Danlos syndrome (type 4). Another population that is at risk includes patients with Turner's syndrome and a bicuspid aortic valve and/or coarctation who are undergoing assisted fertility treatment. Other rarer causes of dissection include cocaine use, previous trauma and atherosclerosis (Figure 4).

As mentioned earlier, once dissection has occurred, maternal and fetal outcomes are highly compromised. The key to ‘treatment’ is therefore prevention. This means ensuring that all women with known or suspected familial aortopathies receive a specialist review prior to pregnancy. In women who are at high risk of dissection, pregnancy may be deemed to be contraindicated or the women may need to consider aortic surgery prior to pregnancy. An example of this would be a woman with Marfan syndrome and an aortic root of greater than 42 mm. Replacement of the dilated component of the aorta does not remove the risk of dissection, but it does ameliorate it [18].
Given the inherited nature of many of these conditions (e.g., Marfan syndrome is an autosomal-dominant disorder that results from mutations in the fibrillin gene on chromosome 15), women should be reviewed by a geneticist. If there is a positive genotyping result, then certain countries will offer preimplantation or prenatal diagnosis if the patient wishes.
In women with known aortopathies, imaging should be performed regularly throughout pregnancy (usually an ECG every 4–6 weeks) and hypertension should be treated aggressively. β-blockers are commonly employed, even in normotensive women, in order to help reduce aortic wall stress. The effectiveness of this is not clear and it is likely that angiotensin receptor blockers may be superior in slowing aortic progression – these agents are, however, contraindicated in pregnancy.
When a woman presents with severe chest pain, hemoptysis or syncope during pregnancy, dissection should be considered at the same time as acute ischemia or thromboembolism. CT scanning or cardiac MRI are both excellent modalities for diagnosing dissection. The small risk of radiation exposure is usually vastly outweighed by the benefits of accurate and early diagnosis. When dissection has occurred, its management is likely to be complex and will often involve either an urgent cardiothoracic operation (with proximal dissections) or a transcatheter hybrid-based procedure. The dissection may include vital arteries supplying the fetoplacental unit.
Detailed discussions regarding the optimal delivery strategy for these patients is beyond the scope of this article but it must be in the setting of a full multidisciplinary environment with input from the obstetrician, neonatologist, anesthetist, cardiologist and cardiac surgeon.
Cardiomyopathy
Cardiomyopathy was the most common cause of morbidity from the Dutch registry [3]. There are several types of cardiomyopathy, each of which has different implications during pregnancy. Pregnancy is of particular risk in symptomatic patients with dilated cardiomyopathy and severe left ventricular dysfunction, mainly due to progression of heart failure. In patients with hypertrophic cardiomyopathy, pregnancy can not only lead to hemodynamic deterioration, but also induce life-threatening arrhythmias.
In the latest UK confidential enquiry, 13 women died over a 3-year period [2]. Of these 13 deaths, nine had either suspected or proven peripartum cardiomyopathy. Peripartum cardiomyopathy is a rare complication of pregnancy and is a diagnosis of exclusion. It has four key features: development of heart failure in the last month of pregnancy or within 5 months postdelivery; absence of another identifiable cause of heart failure; absence of underlying heart disease prior to the last month of pregnancy; and evidence of left ventricular systolic dysfunction [19]. There are many known risk factors for this condition, including maternal age, obesity, hypertension, multiparity, multiple gestation, use of β-agonists and black race [20].
Treatment for all types of myocardial dysfunction is improving, with a case–fatality rate of only 10%. Standard therapies include diuretics, β-blockers and occasionally hydralazine and nitrates. Angiotensin-converting enzyme inhibitors should be started postnatally. When there is acute severe heart failure, inotropic support, mechanical support (balloon pump or ventricular assist device) and transplantation may all be required. Delivery is indicated if cardiac failure cannot be treated adequately. The other specific treatment for peripartum cardiomyopathy is the dopamine antagonist bromocriptine, and early data suggest that this may significantly improve maternal outcome [20].
As with all other cardiac conditions presenting in pregnancy, early diagnosis is crucial. The onset of new asthma in pregnancy (particular in the third trimester or just following delivery) should be viewed with suspicion, and there should be a low threshold for either carrying out a brain natriuretic peptide blood test or performing an ECG.
Valvular heart disease
The most common causes of maternal valve disease are congenital heart lesions in the west and rheumatic disease worldwide. In general, stenotic valve lesions are tolerated less well than regurgitant lesions due to a fixed limitation to cardiac output and peripheral vasodilatation. Valve disease may present for the first time in pregnancy, particularly if it is rheumatic in origin – most commonly mitral stenosis. As the circulating blood volume increases and heart rate increases, there may be elevation of the left atrial pressure and reduced left ventricular filling time. Symptoms may include effort intolerance, the presence of pulmonary edema or of a new atrial arrhythmia.
The optimal treatment for mitral stenosis in pregnancy will depend on the anatomy of the valve, the degree of hemodynamic upset and the gestation. β-blockers, diuretics and anticoagulants can improve symptoms, but balloon valvuloplasty may be required (if the valve anatomy is suitable). Early delivery is another potential therapeutic maneuver. Cardiac surgery should also be considered when the patient is unstable and balloon valvuloplasty is not technically possible.
Metal heart valves continue to represent a particular challenge in pregnancy, with a complication rate in excess of 10%. The choice of anticoagulants is a difficult one, as there is no perfect anticoagulant with maximal maternal efficacy and minimal fetal risk. The incidence of valve thrombosis is lower with oral anticoagulants (warfarin), but fetal risk is higher. Warfarin embryopathy occurs in 4–10% of cases and appears to be dose dependent [21]. The fetus may be at risk of bleeding at any gestation. This bleeding usually leads to the death of the fetus. The European Society of Cardiology Pregnancy and Heart Disease guidelines give a good overview of this topic and optimal treatment algorithms [22].
Arrhythmias & sudden death
It is known that heart rate increases during pregnancy, which results in decreased PR, QRS and QT intervals [23]. The average heart rate increase between the 4th and 16th week of pregnancy is in the region of 20% and palpitation (the awareness of one's heart beat) is extremely common in pregnancy. The majority of palpitations are at the benign end of the spectrum, but some forms of arrhythmia may be associated with maternal morbidity and even mortality. A key component of optimally treating these palpitations is to establish whether there is an underlying structural cardiac abnormality.
Most arrhythmias in pregnancy are benign ectopies or short runs of various types of atrial arrhythmias. When the heart is structurally normal, these can often be managed conservatively (having excluded any other contributing factor, such as thyroid disease). When there is a high arrhythmic burden, antiarrhythmic drugs may be required – these should be drugs with the safest teratogenic profile used in the smallest dose needed to render the patient symptom free. Anticoagulation is rarely required, but might be needed for the patient with a persistent arrhythmia or with recurrent symptoms.
If a patient presents with an acute arrhythmia, all the usual therapeutic options are available, including the use of adenosine (to aid diagnosis of a supraventricular tachycardia), electrical cardioversion, pacing and even ablation. All of these should only be performed in close discussion with cardiologists with expertise in pregnancy.
Women with pacemakers and defibrillators may also wish to become pregnant. Outcomes in these women are predominantly driven by their underlying cardiac diagnosis. If a pregnant patient does receive a defibrillator shock or require cardioversion, then the fetal heartbeat should be documented before (if applicable) and after the shock. Fetal bradycardias have been reported postshock [24].
In the latest UK confidential enquiry, a new entity of sudden adult death syndrome has appeared [2]. This is a previously little-recognized condition of a presumed acute life-threatening cardiac arrhythmia in someone with a structurally normal heart. In pregnancy, this entity has been associated with maternal obesity and the finding of mild left ventricular hypertrophy at post-mortem. It is unclear whether this condition is related to an undetected genetic channelopathy or a new arrhythmic entity.
Pulmonary vascular disease
Pulmonary vascular disease is one of the most feared conditions in pregnancy, but thankfully, it is rare. It did not appear in the Dutch registry, and from the UK Obstetric Surveillance Study registry, there were only six cases per year in the UK [3]. The mortality associated with pregnancy is determined by many factors, in particular the pulmonary vascular resistance and right ventricular function. Patients are quoted to have pregnancy-related mortalities rates of approximately 20–50%. Despite the rarity of this condition, several units have published management guidelines with treatment algorithms, which include phosphodiesterase-5 inhibitors and prostacyclin (endothelin receptor antagonists are teratogenic and should be avoid during pregnancy), for these complex patients [18]. It is thought that these new treatment regimens and improved prepregnancy counseling are, in part, responsible for the observed reduction in maternal deaths [25]. However, pregnancy remains associated with a substantial mortality rate in pulmonary arterial hypertension, and although its outcome has improved [26], patients with pulmonary arterial hypertension should be advised against pregnancy.
Conclusion
The toll from maternal cardiac disease continues to rise, both in terms of morbidity and mortality. The vast majority of these conditions are eminently treatable and some of these deaths are preventable. In certain cardiac disorders, it is thought that a sizable proportion of deaths were in part due to substandard care.
Raising the awareness of heart disease as an important issue in pregnancy and of pregnancy as an important consideration for someone with a heart condition will go some way to improving care. An important rule is to see a timely and accurate diagnosis as being more important during pregnancy than in patients who are not pregnant. Pregnancy should not be used as an excuse to avoid treating important cardiac conditions, but rather as a reason to involve senior specialists as early as possible and accelerate treatment for this high-risk group.
The most common causes of cardiac morbidity and mortality are acquired – not congenital – heart problems that appear for the first time during pregnancy. It is, therefore, vital that the whole team – the general practitioner, midwife, general cardiologist, accident and emergency specialist and obstetrician – are aware of these conditions and know how to access the specialist care these women need. Each geographical region should have an established cardiac/obstetric care pathway in order to deal with the emergency patients.
Executive summary
Pregnancy implies multiple physiological changes (e.g., circulating volumes, vascular resistance and heart rate, among others).
Adaptive mechanisms to pregnancy may become maladaptive in a compromised circulation.
Management of the risk of bleeding, thrombosis and teratogenicity of different drugs may be a challenge.
Prepregnancy counseling is important in order to empower women to make informed choices and to attempt to optimize both maternal and fetal outcomes.
There are several risk score systems that can be used to estimate the risk of an adverse outcome (e.g., Cardiac Disease in Pregnancy and ZAHARA study score, among others).
Women who are not known to have pre-existing heart disease but who develop a cardiac condition during pregnancy have a worse outcome.
β-blockers and aspirin are the treatments of choice for cardiac ischemia symptoms during pregnancy.
Pregnant women with troponin-positive chest pain should undergo invasive assessment with coronary angiography, with close liaison between the cardiologist and obstetrician.
Drug-eluting stents can be used, but within a few months of delivery, bare-metal stent should be considered.
If primary percutaneous coronary intervention is not possible, thrombolysis can be used.
In women who are at high risk of aortic dissection, pregnancy might deemed to be contraindicated.
Aortic root replacement might be indicated before pregnancy (i.e., Marfan syndrome with an ascending aorta diameter of >42 mm).
Dissection should be ruled out at the same time as acute ischemia or thromboembolism in all women with severe chest pain, hemoptysis or syncope during pregnancy.
Different types of cardiomyopathy might have different implications during pregnancy.
During pregnancy, standard treatment includes diuretics, β-blockers and, occasionally, hydralazine and nitrates. Angiotensin-converting enzyme inhibitors should only be started after delivery.
Early data suggest that bromocriptine may significantly improve maternal outcomes in patients with peripartum cardiomyopathy.
Most arrhythmia can be managed conservatively during pregnancy; however, antiarrhythmic drugs may be needed.
In an acute setting, most of the available therapeutic options can be used. Adenosine and β-blockers can be use safely during pregnancy.
If cardioversion is required, the fetal heartbeat should be documented, ideally both before and after the cardioversion.
Patients with pulmonary arterial hypertension are quoted to have pregnancy-related mortalities rates of approximately 20–50%.
Future perspective
The issue of maternal cardiac disease is becoming increasingly recognized. This recognition is leading to additional drives towards improving evidence-based practice and medical education. The ongoing international registry on pregnancy and heart disease provides an excellent opportunity for enlightening both of these areas. In addition, there continues to be a step-by-step improvement in maternal outcomes due to the application of new technologies. An exciting area is that of the new anticoagulants. It is too early to consider using these newer agents in the clinic, but in theory, some of the larger-molecule therapies should not cross the placental barrier. It is, therefore, hoped that there will finally be a highly efficacious, but nonteratogenic anticoagulant in the near future. Despite all of these positive developments, there remains one overriding concern that is likely to increase in the next decade – the incidence of maternal obesity. This issue needs to be addressed urgently if maternal and fetal outcomes are to improve.
Footnotes
Treating cardiac disease in pregnancy
To obtain credit, you should first read the journal article. After reading the article, you should be able to answer the following, related, multiple-choice questions. To complete the questions (with a minimum 70% passing score) and earn continuing medical education (CME) credit, please go to www.medscape.org/journal/wh. Credit cannot be obtained for tests completed on paper, although you may use the worksheet below to keep a record of your answers. You must be a registered user on Medscape.org. If you are not registered on Medscape.org, please click on the New Users: Free Registration link on the left hand side of the website to register. Only one answer is correct for each question. Once you successfully answer all post-test questions you will be able to view and/or print your certificate. For questions regarding the content of this activity, contact the accredited provider, CME@medscape.net. For technical assistance, contact CME@webmd.net. American Medical Association's Physician's Recognition Award (AMA PRA) credits are accepted in the US as evidence of participation in CME activities. For further information on this award, please refer to http://www.ama-assn.org/ama/pub/category/2922.html. The AMA has determined that physicians not licensed in the US who participate in this CME activity are eligible for