
Abstract
Migraine is a common headache disorder, particularly for women, that usually has early onset and lasts well into middle age, with episodes of varying frequency and intensity. The link between migraine and ischemic stroke (IS) is supported by evidence, particularly for migraineurs that have migraine accompanied by aura (MA), which are transient focal neurological abnormalities, usually of the visual field, prior to onset or during headache. The association between MA and other cardiovascular diseases (CVD) such as myocardial infarction (MI) and angina is less clear, as is the causative pathway of any associations, and whether frequency or severity of migraine is a contributing factor [1].
Approximately 18% of American women are affected by migraine each year, whereas the prevalence in men is approximately 6% [2], and 43% of all women will suffer a migraine in their lifetime [3]. The proportion of migraineurs who report MA is between 15 and 30% of all migraine sufferers [4–7]. Migraine has been reported as most prevalent in younger white women of low socioeconomic status, with peak prevalence (∼27%) at the age of 40 years [2,5,6]. The occurrence and degree of severity of migraine aggregates within families [8]. Migraine accounts for high morbidity in the USA, with one estimate that 4.7 h of productive time is lost per 2-week period in migraine sufferers [9], whilst the cost of services used per migraineur per year varies from US$ 522 to 7089 [3]. However, it is generally accepted that migraine is underreported, with up to 66% of sufferers not seeking medical attention [3]. In cross-sectional studies, migraneurs have a higher incidence of depression and anxiety disorders than control groups [2], and one prospective cohort study has shown that depression and migraine have a bidirectional association, although it did not differentiate between MA and migraine without aura (MO) [10]. Cross-sectional and prospective studies report higher incidence of musculoskeletal pain in those reporting all headaches, but no prospective trials have demonstrated an association with migraine [2].
The association of MA and IS has been well documented, and has been found in crosssectional, case–control and prospective cohort studies [11–15]. The mechanism underlying this link is unknown, but may be the result of an increased prevalence of other conditions that have been associated with MA such as vasculopathies, hypercoagulable states and patent foramen ovale [16,17]. It has been hypothesized that migraine may be a local manifestation of a systemic vascular abnormality [18]. MA is due to cortical spreading depression, which is a short-lasting depolarizing wave that moves across the cortex, inciting a cascade of neurological excitation, inflammation and metabolism. More recently, other CVDs, including MI and angina pectoris, have been associated with migraine in prospective studies [19–21].
Women's Health Study
The Women's Health Study (WHS) is an epidemiological study that has increased understanding of the relationship between IS and other CVDs with migraine in women. It is one of the few prospective cohort studies that has information on migraine status at the beginning of the observation period and has investigated the association with CVD outcomes after adjustment for other cardiovascular risk factors. Other prospective studies including women have been the UK General Practice Research Database [21], the US Atherosclerosis Risk in Communities [15,20], the US United Healthcare cohort [22], the Australian Blue Mountains Eye Study [14] and the US Kaiser-Permanente Medical Care Program [19]. Many cross-sectional studies and case-control studies have also reported an association, but have less validity in suggesting a potential causal relationship [23].
The WHS is a cohort of 39,876 apparently healthy US female health professionals aged 45 years and over that was established to test the benefits and risks of low-dose aspirin and vitamin E in primary prevention of CVD and cancer. Participants were questioned at baseline on their history of migraine headaches, the frequency of headaches in the previous year, and whether they were accompanied by aura. Migraine history and blood samples were available on 27,798 of the women, and this cohort has been the basis of the publications on migraine and cardiovascular diseases produced by the research group. They have studied the association of migraine and MA at baseline with biomarkers for CVD [24], Framingham risk score for CVD [25], and occurrence of cardiovascular events (defined as major CVD [first instance of nonfatal IS, nonfatal MI, or death due to ischemic CVD], first IS, MI, coronary revascularization and angina) [26]. After a mean follow-up of 10 years, the group found MA was associated with a higher risk for all cardiovascular events (HR: 2.15; 95% CI: 1.58–2.92; p < 0.001), when adjusted for other cardiovascular risk factors, hormone therapy use and family history of MI prior to 60 years of age [26]. The cumulative incidence of CVD did not diverge until 6 years of age into follow-up, suggesting there was no difference in risk in initial years [25]. When looking at association of MA and CVD stratified for Framingham risk score, women with MA in the lowest risk category (<1%) had the highest risk of IS (HR: 3.88; 95% CI: 1.87-8.08; p < 0.001), but those in the highest risk group (>10%) had the highest risk of MI (HR: 3.34; 95% CI: 1.50–7.46; p = 0.003) [25]. When stratified by risk factor, it was the younger women and the nonsmokers that had highest risk for both MI and IS, suggesting that migraine is an important risk for women with otherwise low-risk profiles. This is in contrast to case-control studies that suggest the risk of IS for women with MA was greatest in young women taking oral contraceptives that smoked [13,27]. However, Kurth and co-authors did not show absolute risk for migraineurs in each Framingham score, only relative risk. Nor did they include tests for interaction across the strata of scores [28].
Results
In the current study, the researchers from the WHS focus on the association between the frequency of migraine headaches (less than monthly, monthly and at least once per week) and risk of a major cardiovascular event, MI, IS, coronary revascularization and angina amongst 27,798 women working in health, free of CVD and apparently healthy at baseline [1]. Over a mean follow-up period of 11.9 years, the study found a J-shaped association, with an increased hazard ratio for major CVD amongst women who had migraine less than monthly at baseline and those with migraine weekly or more at baseline when compared with those women without a history of migraine, when adjusted for age, other CVD risk factors, hormone therapy use and family history of MI prior to 60 years of age (1.55 [95% CI: 1.22-1.97; p < 0.001] and 1.74 [95% CI: 0.78–3.89; p = 0.11], respectively; see Table 1). The lack of dose response, and lack of a convincing biological explanation of a J-shaped association, is suggestive of a lack of causal relationship between migraine frequency and CVD [23], although confidence intervals are wide.
Hazard ratio (95% CI) for cardiovascular disease by migraine frequency in the Women's Health Study.
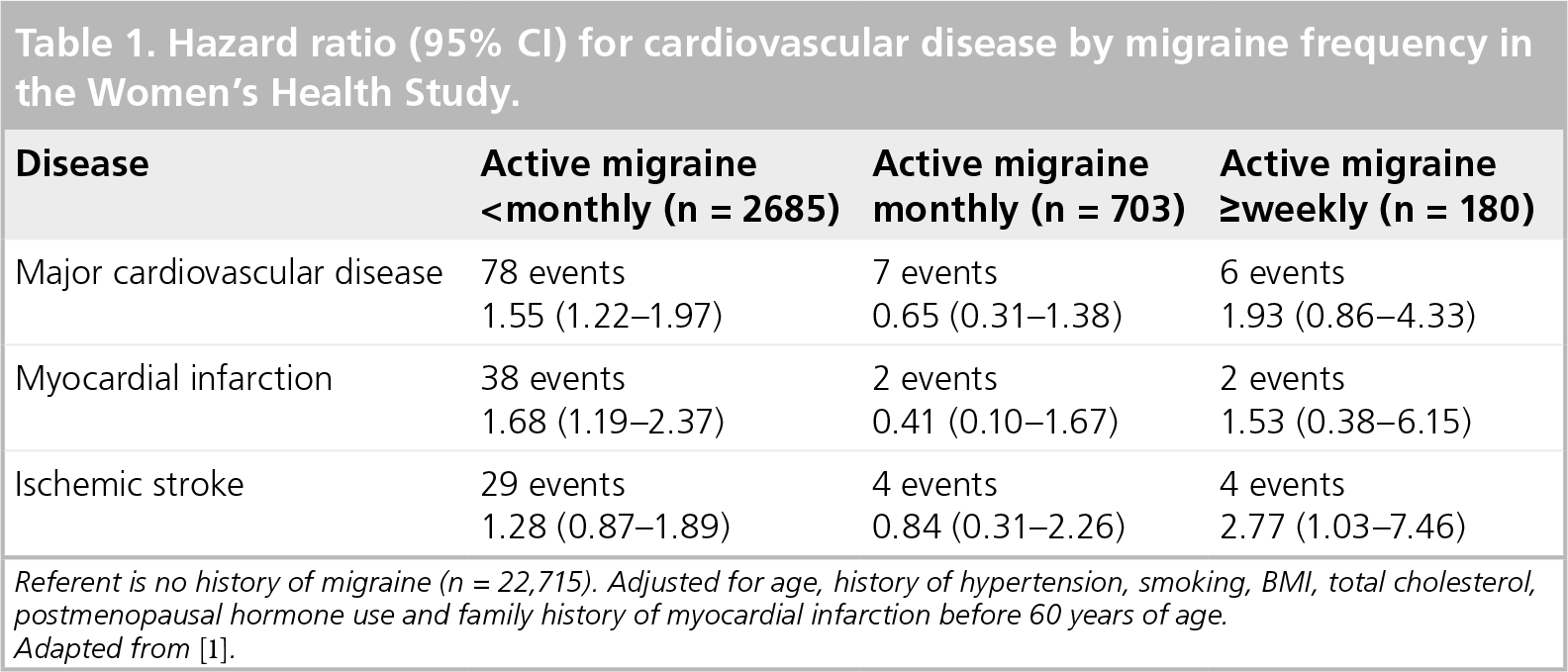
Referent is no history of migraine (n = 22,715). Adjusted for age, history of hypertension, smoking, BMI, total cholesterol, postmenopausal hormone use and family history of myocardial infarction before 60 years of age.
Adapted from [1].
When looking at consistuent CVD end points, significant results were an increased risk of IS in women who reported migraine frequency of weekly or greater (2.77; 95% CI: 1.03–7.46) and greater risk for MI amongst women with the least frequent migraine of less than monthly (1.68; 95% CI: 1.19-2.37), compared with those with no history of migraine. When migraineurs were stratified according to aura status, there was increased risk for women with MA of monthly or less, compared with women free of migraine, for all of the outcomes. Frequency greater than weekly was significantly associated with IS only (4.25; 95% CI: 1.36-13.29; p < 0.001). Again, no interaction across the doses was reported.
Conclusion & future perspective
The latest work from the WHS adds to the body of literature they have produced on migraine as a risk for CVD events. To our knowledge, this is the first prospective study to have looked at the association between frequency and CVD to date, and the WHS results suggest that frequency of attacks could be a moderating factor in the risk of migraine for CVD. The most limiting factor in the latest study from the WHS is the low number of outcome events in each subgroup, making the results far from convincing, as is witnessed by the wide confidence limits in Table 1. There are no data on the frequency of migraine during the follow-up period, or how recently women had migraine relative to the cardiovascular event. This may have varied a great deal within the subgroups and have a potential influence on the risk of CVD for women, although migraine frequency tends to decrease with age over 45 years, as all these women were. The WHO Collaborative Study of CVD and Steroid Hormone Contraception, a hospital-based, case-control study, found that time since onset of migraine was associated with IS [29]. The association was U-shaped, with those of most recent onset (within 2 years) and longest onset (more than 12 years) at greatest risk. They found no significant association with change of frequency of migraine, but women with initial frequency of 13 or more per year had increased risk.
There is a paucity of good epidemiological studies on migraine and CVD, with the most complete review of the literature to date identifying that the WHS is the best prospective study to evaluate the importance of migraine and CVD [30]. More epidemiological studies are required before frequency of migraine can be said to be important in the risk of CVD, especially in younger women who are likely to have more frequent migraine attacks.
Executive summary
Migraine with aura and cardiovascular disease are associated.
The causal pathway remains unclear.
Frequency of migraine attack may be a moderating factor in the association, but no dose response is evident.
No information exists on the impact of severity of migraine attacks on cardiovascular risk.
Footnotes