
Abstract
Peripartum cardiomyopathy is a form of heart failure occurring at the end of pregnancy or early in the postpartum period. Women may recover, have persistent cardiac dysfunction or suffer complications and death. Women who are African-American, older, hypertensive or have multiple gestation pregnancies have increased risk. Diagnosis and treatment may be delayed due to similarities between symptoms of normal pregnancy and heart failure. Echocardiography is essential for the diagnosis, and B-type natriuretic peptide can be helpful. Treatment for systolic heart failure must be adjusted during pregnancy, and anticoagulation may be indicated. Even after recovery, subsequent pregnancy confers substantial risk of worsening heart failure. Further investigations into the etiology, duration of treatment and risks for relapse are needed.
Peripartum cardiomyopathy (PPCM) is a type of heart failure affecting childbearing women at the end of pregnancy or in the early postpartum period. Although some women have relatively mild disease and may recover completely, others suffer significant morbidity and mortality. The field of research is rapidly evolving but many questions remain unanswered. The goals of this review are to describe the clinical characteristics, risk factors and prognostic factors for short and long-term outcomes, current knowledge of the etiology and pathophysiology of the disease, recommendations for diagnosis and treatment, considerations for breastfeeding and subsequent pregnancies and unanswered questions and directions for future research.
Clinical definition
PPCM was previously defined as symptoms of heart failure presenting in the last month of pregnancy and up to 5 months postpartum [1,2]; however, Elkayam
Risk factors
Several associated conditions have been identified, including hypertension and pre-eclampsia, African–American race, older maternal age and multiple gestation pregnancies [4,6]. Some earlier studies of PPCM excluded women with hypertension due to concerns about misdiagnosing hypertensive heart disease, rather than true PPCM [8]. More recently, however, it has been recognized that hypertension and pre-eclampia are significant risk factors for the development of PPCM [8]. A meta-analysis of 22 studies revealed a striking correlation between pre-eclampsia and PPCM, suggesting there may be a shared pathological mechanism [8]. In addition, elevated rates of hypertension among women with PPCM have been identified in many studies [3,8–11]. African–American women have both a higher risk of developing PPCM and have a worse prognosis [10–15]. Women with PPCM tend to be older, with a higher incidence noted among women over age 30 years [3,9,14]. Multiple gestation pregnancies are also more common in women with PPCM [8,11,16,17]. Recently, Kao
Etiology & pathophysiology
The etiology and pathophysiology of PPCM is not fully understood, but several hypotheses have been studied. Viral myocarditis has been implicated and may be more prevalent among peripartum women [19,20], perhaps due to diminished immune response, but studies have been highly variable [21] and histologic diagnosis difficult [2]. Autoimmune or immune system dysfunction has been implicated and high levels of circulating cardiac antibodies have been identified [21,22]. Selenium deficiency was identified among women with PPCM from the Sahel region of Africa [23]; however, studies in other regions such as Haiti have identified no such deficiency [24]. Other micronutrients have been studied, including vitamin A, vitamin B12, vitamin C and β-carotene, but no clear connection has been established [24].
It has also been suggested that the hemodynamic changes and increased volume load of pregnancy place stress on the heart and lead to myocardial dysfunction. However, the greatest hemodynamic changes of pregnancy occur during the second trimester, whereas PPCM usually presents in the last month of pregnancy, with the majority of women presenting in the first month postpartum [6]. This is supported by data from the international Registry of Pregnancy and Cardiac Disease (ROPAC), which showed that heart failure complications among patients with other forms of cardiomyopathy developed at a median time of 31 weeks' gestation, with the highest incidence at the end of the second trimester [25]. Therefore, although hemodynamic changes may exacerbate heart failure from other causes, different mechanisms likely trigger the development of PPCM.
More recently, the role of oxidative stress and angiogenic imbalance has received attention. In mice, the specific deletion of cardiomyocyte STAT3 leads to increased oxidative stress and proteolytic activity of cathepsin D, which cleaves the nursing hormone prolactin into a pathogenic 16 kDa fragment that has antiangiogenic, proapoptotic and proinflammatory properties [26].
Additional mechanisms of PPCM may include the release of soluble Flt-1 (sFLT1; also called soluble VEGFR-1) from the placenta in the latter stages of pregnancy [27]. sFLT1 is an enzyme in the tyrosine kinase family which appears to be cardiotoxic and anti-angiogenic. Though it is not known for certain whether it is cardiotoxic in humans, sFLT1 is found in elevated levels in women with both PPCM [27] and pre-eclampsia [28].
Symptoms & diagnosis
Women presenting with PPCM often experience a delay in diagnosis due to the overlap of symptoms in late pregnancy, such as dyspnea, weight gain, lower extremity edema, fatigue, palpitations and orthopnea. Additional symptoms may include persistent cough, chest pain, lightheadedness and abdominal discomfort secondary to hepatic congestion [4]. Both patients and their medical caregivers may assume symptoms are related to the late stages of pregnancy, or to the exhaustion of having recently given birth and the sleeplessness of caring for a newborn. Physical examination findings typical of heart failure, such as elevated JVP, S3 gallop and edema, are also commonly seen in normal pregnancy. Therefore, many women experience a delay in diagnosis. Early diagnosis is essential to initiate timely medical management and can help to avoid serious complications [29].
Since survival and recovery are both improved by early diagnosis, a mechanism for quantifying the severity of various symptoms has been proposed and validated [30] (see
Self-test for early diagnosis of peripartum cardiomyopathy.
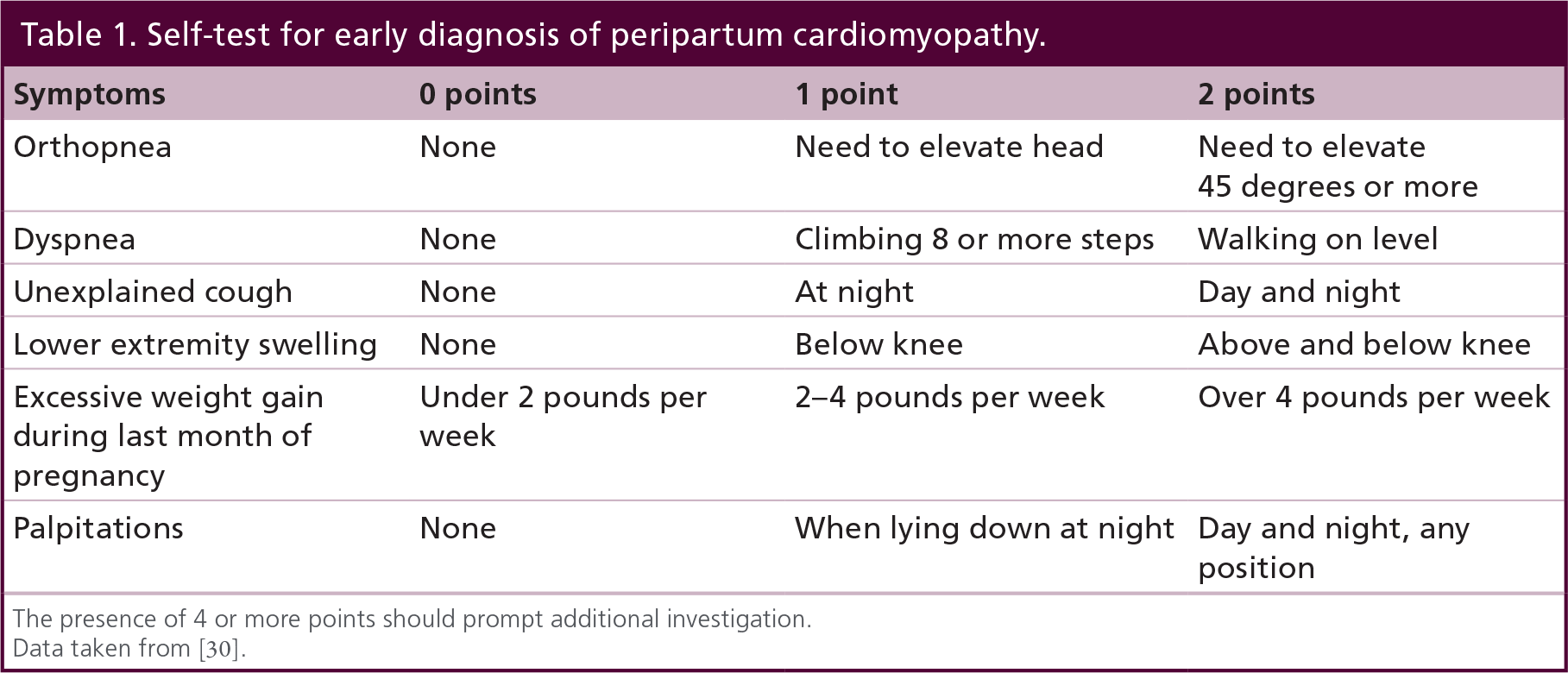
The presence of 4 or more points should prompt additional investigation.
Data taken from [30].
Treatment
Standard heart failure therapy should be initiated as soon as PPCM is diagnosed; however, special consideration must be given to the safety of medications during pregnancy or lactation. Typical heart failure therapy includes angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs), aldosterone antagonists, β-blockers and diuretics for the treatment of volume overload, in addition to digoxin, hydralazine and nitrates. In pregnant women, these typical therapies are used with notable exceptions, as follows.
Diuretics, such as furosemide, are indicated for the treatment of volume overload and congestion during pregnancy. In addition to standard side effects, including hypokalemia, azotemia, dehydration and hypotension, there is potential risk for decreased placental perfusion. Women are at increased risk for volume overload shortly after delivery as there is an increase in intravascular volume due to fluid resorption. Overly aggressive diuresis can lead to hypovolemia and hypotension, which may prevent appropriate up titration β-blockers and ACE-inhibitors/ARBs.
ACE-inhibitors and ARBs are contraindicated during pregnancy due to teratogenic effects, and may not be used [31]. For afterload reduction during pregnancy, a combination of hydralazine and isosorbide dinitrate can be used [6]. Spironolactone, an aldosterone antagonist, has been shown to have estrogenic effects in rats, causing feminization and endocrine dysfunction that persists into adulthood in both sexes [32,33]. For this reason, spironolactone is avoided during pregnancy. Eplerenone has not been studied during pregnancy. Postpartum, these medications are considered safe. For lactation, Captopril [34] and enalapril [35] have both been studied and are considered by the American Academy of Pediatrics to be safe for use while breastfeeding, without significant effects on the baby [36]. Spironolactone has also been shown to be excreted in a clinically insignificant amount in human breast milk [37].
β-blockers (category C) can be used both during and after pregnancy. Although Carvedilol, metoprolol succinate and bisoprolol are chosen for treatment of heart failure, these medications have not been studied in pregnant women. During pregnancy, metoprolol tartrate is commonly chosen because it has been used more often than other β-blockers during pregnancy [38]. Atenolol should not be used during pregnancy due to fetal growth retardation [39]. For the infant, β-blockers may be associated with smaller size for gestational age, hypoglycemia, bradycardia and respiratory depression upon birth; therefore, newborns exposed to β-blockers should be supervised for 24–48 h after delivery [40]. Metoprolol is also considered compatible with lactation [36]. Digoxin, hydralazine and isosorbide dinitrate are all category C medications and can be used during pregnancy when indicated; digoxin and hydralazine are also safe with lactation [36].
Pregnancy confers a hypercoagulable state which peaks during the third trimester and persists up to 8 weeks postpartum [41]. In a study of 100 women in South Africa with PPCM, 16% had presence of LV thrombi detected by echocardiography [42].
Therefore, in the setting of reduced EF, anticoagulation should be considered [40,43]. Atrial fibrillation, LV thrombus, systemic embolism, use of bromocriptine and EF less than 30% are all indications for anticoagulation [44]. Warfarin or low molecular weight heparin (LMWH) can be used, depending on the stage of pregnancy, and both can be used during lactation. If LMWH is used during pregnancy, monitoring anti-Xa levels is recommended [40].
Bromocriptine is a prolactin blocker, initially developed and marketed for lactation suppression. Based on the hypothesis that the 16 kDa form of cleaved prolactin has antiangiogenic and apoptotic mechanisms, blocking the release of prolactin was found to be an effective treatment for PPCM in a mouse model of the disease [26]. In the pilot pro of-of-concept study of bromocriptine in humans, it was given to ten women in South Africa and compared with ten women controls treated with standard therapy [45]. Women treated with bromocriptine (2.5 mg twice daily for 2 weeks, followed by 2.5 mg daily for 6 weeks) in addition to standard heart failure therapy had greater improvement in LV systolic function at 6 months (27–58%; p = 0.012) than the control group (27–36%). The composite end point was defined as death, NYHA functional class II/IV or EF < 35% at 6 months. Fewer patients in the bromocriptine group experienced the composite end point (n = 1; 10%) as compared with the control group (n = 8, 80%; p = 0.006). Despite these promising results, the following criticisms of this study have been noted: the study was small, with only ten women receiving therapy, only South African patients were studied, and the results may not apply to other races and geographic regions and the control group in this study had a much higher mortality rate than has been described in almost every other population of patients with PPCM and this may have skewed the results [46]. In an observational prospective registry of 115 German patients with PPCM, treatment with β-blockers and ACE-inhibitors/ARBs was associated with high rates of recovery [47]. There was no significant difference in recovery among patients also treated with bromocriptine, and further randomized multicenter trials are needed, such as the study ongoing in Germany [48].
Bromocriptine also has some safety concerns. In case reports, bromocriptine used for lactation suppression has been associated with myocardial infarction [49–52], stroke [53,54] and seizures [54]. If bromocriptine is used, full-dose anticoagulation is typically also implemented. In addition, since bromocriptine inhibits prolactin, women are unable to breastfeed, and these implications need to be considered (see ‘Lactation’ section below). Bromocriptine is not currently approved by the US FDA for the treatment of PPCM.
Implantable cardioverter defibrillator (ICD) placement for primary prevention of sudden cardiac death is indicated in nonischemic heart failure with EF less than 35% on optimal medical therapy for 3–6 months [43]. However, standard guidelines do not specifically address PPCM, which is unique in that many women will recover from myocardial function over time. In a small prospective study of women with newly diagnosed PPCM, three of seven patients with severely reduced EF who wore a wearable cardioverter/defibrillator were found to have ventricular fibrillation that was appropriately shocked [55]. Therefore, in women diagnosed with PPCM and severe LV dysfunction, wearable defibrillators should be considered during the first 6 months while heart failure therapy is initiated and while LV recovery is assessed. ICD therapy can then be offered to patients with persistent severe LV dysfunction, though it appears ICD therapy may be underutilized among women with PPCM [56].
Advanced therapies, including left ventricular assist devices (LVADs) and heart transplantation, are indicated for women with severe disease. Although heart transplantation for PPCM remains relatively infrequent, in a multicenter study of 69 women with PPCM who underwent heart transplantation, survival and freedom from allograft vasculopathy was similar to that of women who received a transplant for other cardiomyopathies [57].
Prognosis & outcomes
Within 2 to 6 months after diagnosis, a majority of women with PPCM have either partial or complete myocardial recovery [3,11]. The estimates of recovery rates are variable. In a study of 55 patients (51% African–American), 62% had some degree of LV recovery, and 45% recovered to an EF greater than 50%, with an average follow-up time of 29 months [11]. Among a group of 40 indigent (87.5% African-American) patients, only 35% recovered, with an average recovery time of 54 months [13]. In the prospective Intervention in Myocarditis and Acute Cardiomyopathy 2 (IMAC2) registry that included 39 women with PPCM with a mean initial EF of 0.27 ± 0.07, nearly half recovered normal cardiac function by 6 months [58]. Compared with other forms of cardiomyopathy, women with PPCM appear to have higher rates of recovery [58]. Among women who do not recover LV function, the prognosis is similar to other types of dilated cardiomyopathy [43], with worse outcomes and increased 5-year mortality [6].
Prognostic factors
Baseline EF is an indicator of the severity of myocardial insult, and patients with worse baseline function tend to have lower rates of recovery [3,13,16,59–61]; however, there are exceptions, and the sensitivity of baseline EF is not sufficient to dictate use of advanced therapies such as LVAD or transplant [16]. The presence of LV dilatation [9,11,59,62] and LV thrombus [11] have also been associated with worse outcomes. Chap a
African–Americans are also identified as having worse outcomes [15], though the reasons for this are not completely understood. Advanced maternal age has been associated with increased incidence of PPCM, but among women in South Africa, older age has recently been linked to higher rates of recovery [63]. Markers of inflammation (Fas/apo-1) [42], elevated troponin [64] and NT-proBNP [65] levels are associated with poor outcomes. Among 55 women with PPCM recruited through the Internet, breastfeeding was associated with recovery [17].
In a study of 100 South African patients, there was a 15% mortality rate that was associated with worse initial NYHA functional class, lower initial systolic blood pressure, increased end-diastolic and end-systolic dimensions, lower LV EF, higher AST and increased levels of circulating Fas/Apo-1 [42]. In multivariate logistic regression, only NYHA functional class and baseline plasma levels of Fas/Apo-1 predicted mortality [42].
Lactation
The WHO and the American Academy of Pediatrics recommend that infants receive breast milk exclusively for the first 6 months of life, with continued breastfeeding for the first 1–2 years or longer [66]. In developing countries where formula can be expensive and clean water is not readily available, not breastfeeding can pose a significant risk to the survival and well-being of the infant [67]. The 2010 European position statement on PPCM advises against breastfeeding based on the concern for propagating the pathogenic prolactin pathway by continual stimulation for release of prolactin [4]; however, no study has shown worse outcomes among women who breastfeed. On the contrary, a study of patients enrolled via the Internet indicated that women who breastfed had higher rates of recovery [17]. Although breastfeeding can increase metabolic demands and may not be appropriate in all cases, expert opinion suggests that women with PPCM who are clinically stable should not be discouraged from breastfeeding [38]. Since most medications for the treatment of heart failure can be given safely with breastfeeding, this should not be a reason to advise women against lactation.
Subsequent pregnancy
Appropriate counseling for women after a diagnosis of PPCM is critical. Women who do not have complete myocardial recovery should be advised to avoid future pregnancies [4,40]. The 2010 European position statement also recommends against repeat pregnancy if the LVEF was less than 25% at the time of diagnosis [4]. In a retrospective analysis of 16 women who did not recover LV function prior to subsequent pregnancy, 44% had symptoms of heart failure, 25% had a decrease in LVEF by more than 20%, 31% had persistent LV dysfunction after pregnancy and 19% died [68]. By combining these data with results from seven other studies of women with persistent LV dysfunction, it was found that in 93 pregnancies, nearly half had symptoms of heart failure and deterioration of LV function, 39% had persistent LV dysfunction at the time of follow-up, and 16% died [38].
Among women with complete LV recovery, the recommendations are less clear. In the retrospective analysis by Elkayam
Unfortunately, it remains difficult to predict which patients will experience a relapse during subsequent pregnancy. Prediction of relapse during subsequent pregnancy is generally best indicated by pre-pregnancy LVEF. Expert opinion suggests that risk of relapse is lowest among those who recover LVEF to at least 55%, without any deterioration in function after withdrawal of ACE-inhibitor/ARB, and possibly, among those with adequate contractile reserve on exercise echocardiography [69].
The use of treadmill stress echocardiogram to assess contractile reserve has not been studied in randomized trials and is largely based on a study of nine patients with recovered function who had normal cardiac reserve and no relapse during subsequent pregnancy [70]. Nevertheless, it seems reasonable that if there is inadequate contractile reserve with stress echocardiography, complete myocardial recovery has not occurred and the risk of relapse during a subsequent pregnancy may be increased [69]. Further studies are needed in order to determine whether other pre-pregnancy tests could predict the risk of relapse. Optimal medical therapy among women with recovered LV function during subsequent pregnancy is also unclear [38].
Conclusion
PPCM carries substantial risk for morbidity and mortality, with particularly high risk during repeat pregnancy. Early diagnosis is necessary for the prevention of complications. Use of echocardiography and B-type natriuretic peptide levels can aid in the diagnosis and management. Treatment with heart failure medications must be implemented, with particular attention to choosing those that are safe during pregnancy and lactation. Multidisciplinary expertise in both obstetrics and cardiology is essential for providing optimal care.
Future perspective
Many questions about PPCM remain unanswered. Prospective registries and multicenter studies are needed. One such initiative is the EURObservational Research Programme of the European Society of Cardiology, which has over 100 patients enrolled from 20 countries [71]. The goal is to enroll 1000 patients and to collect data on 6- and 12-month outcomes, as well as information regarding their offspring [71]. Future studies are needed to determine recommendations for the duration of medical therapy following recovery of LV function; the optimal medical therapy during subsequent pregnancy; and the use of diagnostic testing to improve the prediction of risk during subsequent pregnancy. Despite exciting advances in the pathophysiology of PPCM, the role of sFLT1 and prolactin and its inhibition, as well as the potential ‘triggers’ for PPCM are incompletely understood [72]. A genetic basis for PPCM has been proposed [73], and research is ongoing. Treatments specific to PPCM such as bromocriptine, pentoxyphylline and intravenous immune globulin, require further study. The use of biomarkers and risk prediction models to improve screening has the potential to improve outcomes through earlier diagnosis.
Executive summary
Peripartum cardiomyopathy (PPCM) is systolic heart failure (ejection fraction typically <45%) diagnosed in the latter stages of pregnancy or in the months following delivery, where no other cause of heart failure is found.
Most women present in the first month postpartum or in the last month of pregnancy.
Risk factors include African–American race, hypertension, pre-eclampsia, older age and multiple gestation pregnancy.
Diagnosis can be delayed due to overlap of signs and symptoms of heart failure mimicking those of late pregnancy.
Pathophysiology is not completely understood, but oxidative stress leading to pathologic cleavage of the nursing hormone prolactin into 16 kDa form that has antiangiogenic and proapototic actions may play a central role. Soluble FLT1 is an antivascular protein produced by the placenta during late pregnancy; it is found in higher concentrations in women with PPCM.
Standard heart failure therapy should be initiated, with the exception of angiotensin-converting enzyme inhibitors, angiotensin receptor blockers and aldosterone antagonists, which should not be used during pregnancy, but may be used postpartum, even in breastfeeding women. Hydralazine/dinitrate combination therapy can be used for afterload reduction during pregnancy.
Metoprolol tartrate is the typical choice of β-blocker during pregnancy and furosemide is used for volume overload. Atenolol should not be used.
Anticoagulation may also be indicated.
Bromocriptine is a promising treatment but has not been fully studied.
Treatment with heart failure medications should not preclude breastfeeding, as many medications are compatible.
Although myocardial improvement is typically seen in the first 6 months of diagnosis, women who do not fully recover are at increased risk for heart failure complications and mortality.
Women with persistent myocardial dysfunction should be counseled against subsequent pregnancy.
Women with complete myocardial recovery who have a subsequent pregnancy are at increased risk for heart failure symptoms with a substantial deterioration in ventricular function, which may be permanent; however, the risk of mortality during subsequent pregnancy is low.
Specific therapies such as bromocriptine, pentoxyphylline and immune globulin require further study.
The understanding of the pathogenesis of PPCM continues to evolve, and will help guide the use of future treatments.
After recovery, it is unclear how long medical treatment should be continued.
Additional information about how to predict the risks of subsequent pregnancy is also needed.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.