
Abstract
Greater than 70% of human breast cancers express the androgen receptor (AR). Emerging preclinical and clinical data suggest that AR may play a role in breast cancer pathogenesis and may serve as a therapeutic target in certain more difficult-to-treat breast cancer subtypes, such as triple-negative breast cancer. Although this is an area of active investigation, the clinical significance of this hormone receptor as a prognostic/predictive marker and its functional role in tumorigenesis is unclear. This review provides an update on the advances made in the last several years regarding the role of AR as a prognostic/predictive biomarker in breast cancer, the underlying biology of AR signaling in breast cancer development and the available clinical data for the use of androgen inhibition in the treatment of AR+ triple-negative breast cancer.
Keywords
Breast cancer is a heterogeneous disease characterized by various predisposing risk factors, clinicopathologic features and molecular characteristics. These differences lead to disparate clinical outcomes and distinct therapeutic strategies. Over recent decades, endocrine and targeted therapies have become integral components of breast cancer management. Tamoxifen and aromatase inhibitors have transformed the management of breast cancers that express estrogen receptors (ERs) and progesterone receptors (PRs). Trastuzumab and other agents, such as pertuzumab and trastuzumab emtansine, provide effective options to treat tumors that over-express HER2 with significant improvement in survival [1,2].
However, for individuals whose tumors are triple negative – that is, do not express the ER, PR or HER2, such effective and well-tolerated therapeutic alternatives to cytotoxic chemotherapy are lacking. Triple-negative breast cancer (TNBC) represents approximately 15–20% of all breast cancers and, generally, has a more aggressive clinical course with early onset of distant, often visceral, metastases and shorter overall survival [3–6]. An important point of clarification for any discussion of TNBC is to recognize that TNBC is an entity defined by the absence of immunohistochemical (IHC) markers for ER, PR and HER2. This is distinct from basal-like breast cancer, which refers to the subtype defined by a gene-expression profile associated with epithelial cells in the basal or outer layer of the adult mammary glands. Most, but not all, basal-like tumors lack surface expression of ERs and PRs, as well as HER2, and are thus triple negative. However, TNBCs are heterogeneous and include gene-expression signatures inclusive of the basal-like molecular subtype, in addition to others [7]. The discordance between IHC-determined receptor status and molecular subtype highlights the limitations of our conventional markers as a surrogate for breast cancer subtype.
The absence of validated, molecular targets renders TNBC ineligible for conventional endocrine and HER2-targeted therapies. Novel, potentially drugable targets have been identified; however, none have, as of yet, improved upon the established standard cytotoxic chemotherapy for the treatment of TNBC. One such target is the androgen receptor (AR). The AR is expressed in 70–90% of all breast cancers and is, thus, the most commonly expressed nuclear hormone receptor in breast cancer [8–11]. In retrospective analyses, expression of the AR in ER−/PR− tumors varies widely from 9 to 50% [12–14], and is highly expressed in the majority of ER− breast cancers with apocrine differentiation [15]. Recently, a prospective trial screened patients with metastatic ER−/PR− breast cancer for AR status and found that approximately 12% of these patients expressed AR >10% [16]. AR+ TNBC comprises a small percentage (~2%) of all breast cancers; however, as breast cancer is the most common malignancy affecting women in the USA (~230,000 new diagnoses in 2013), this small percentage translates into an absolute number of patients comparable to those annually diagnosed with chronic myelogenous leukemia. Given the emphasis oncologists place on precision medicine, focus on such a potential novel target makes it highly clinically relevant.
This review will summarize our current understanding of the role of the AR in TNBC. The narrow scope introduces the AR in a setting free from the influence of other steroid hormone receptors. It is recognized that the AR plays a part in ER- and HER2-dependent breast cancers. While a discussion of this role is beyond the scope of this review, the framework created may allow for a better understanding of the role of the AR in these other subtypes.
Structure & function of the AR
Androgens are steroid hormones that regulate male development and reproductive function, and have a key role in the growth of prostate cancer. The AR is a member of the steroid hormone receptor family and functions as a classic ligand-activated intracellular transcription factor [17]. The gene for the AR is found on chromosome Xq11–12 and encodes a 110 kDa cytoplasmic polypeptide that has four distinct functional regions [18]. These include a regulatory domain at the amino terminal (AF-1 site), a DNA-binding domain composed of two zinc fingers, a hinge region with a nuclear localization signal and a C-terminal ligand-binding domain (AF-2 site).
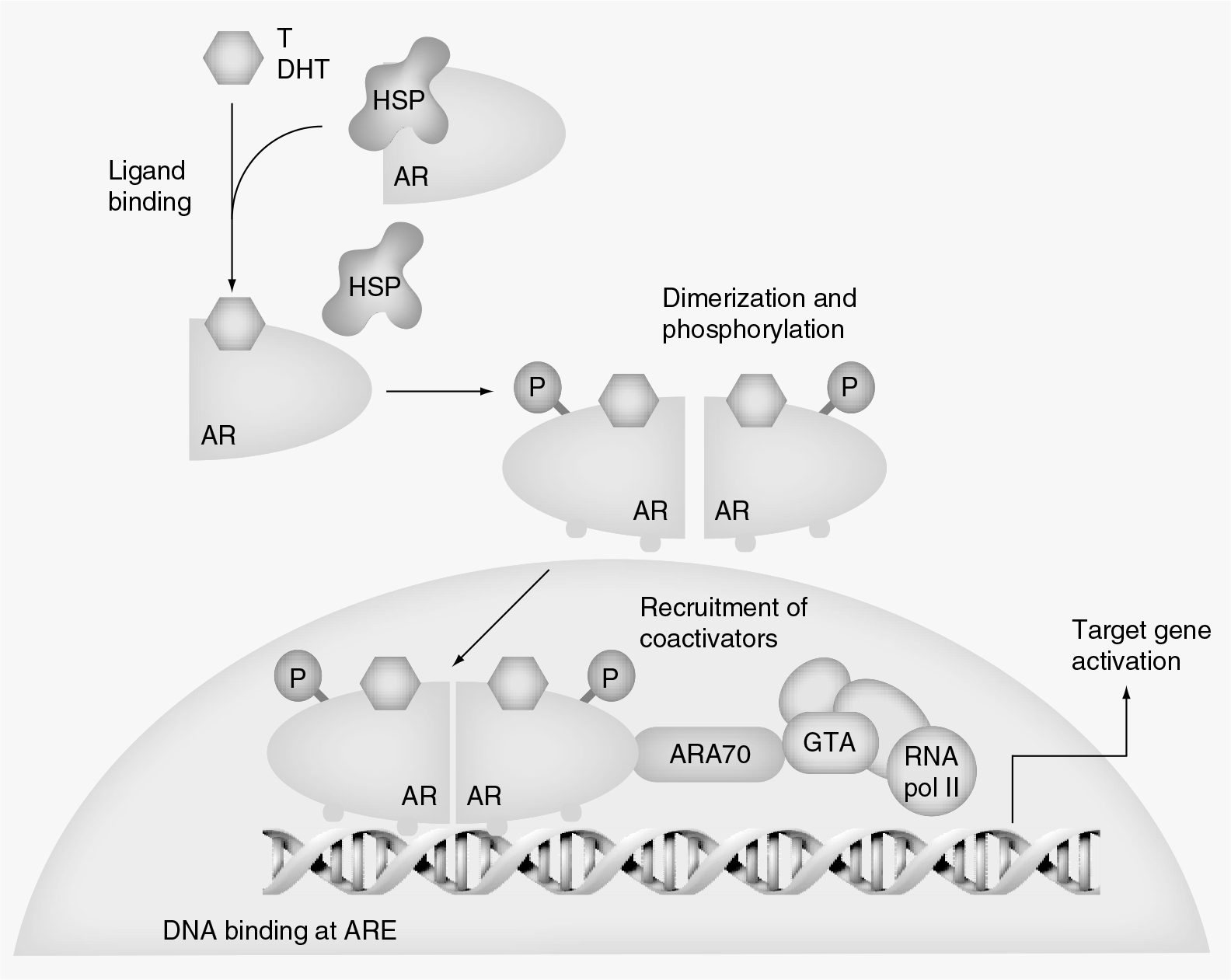
When inactive, the AR is bound to heat shock proteins (e.g., heat shock proteins 90, 70, 56 and 23) that stabilize it in such a way to expose the C-terminal ligand-binding domain. Circulating androgens, such as testosterone and dihydrotestosterone, bind to this C-terminal ligand-binding domain, displacing the bound heat shock proteins through conformational change. Androgen-bound AR leads to AR dimerization and the requisite phosphorylation of its tyrosine kinase, which in turn causes translocation of the AR complex to the nucleus. The DNA-binding domain of the AR then binds to androgen response elements in both the promoter and enhancer regions of target genes and creates an active transcription complex upon recruitment of coregulatory proteins (Figure 1). Literature reveals that AR-regulated genes vary widely between cell lines and disease context, for example, in prostate cancer, which has become castrate resistant. Representative AR-regulated genes in castrate-resistant prostate cancer (CRPC) tissue code for enzymes in steroid precursor synthesis, PSA, TMPRSS2, IGF-1 and MYC [19]. In addition to regulating target gene transcription, the AR also interacts with signal transduction proteins in the cytoplasm, such as Src and Akt, which play key roles in cell survival, proliferation, invasion and angiogenesis [18].
Prognostic & predictive utility of the AR in breast cancer
Several studies have examined the prognostic and predictive value of AR expression in breast cancer [12,13,20–36]. The majority of these studies conclude that the AR is a favorable prognostic marker, irrespective of hormone receptor status. Although a comprehensive recapitulation is beyond the scope of this review, selected recent studies that address TNBC in particular are discussed here.
Hu
By contrast, He
Sutton
To better characterize prognostic markers in TNBC, Rakha and colleagues examined a panel of markers, including the AR, in a series of primary, operable, invasive breast cancer from patients presenting to a single institution from 1986 to 1998 [21]. Of the 282 triple-negative tumors identified in this cohort, 36 (13%) demonstrated AR expression by IHC (AR+ ≥1%). Among individuals with TNBC, the absence of AR expression correlated with a higher histologic grade (p < 0.001), development of recurrence (p = 0.038) and the development of distant metastases (p = 0.049). However, this correlation was not confirmed in a multivariate analysis including age, tumor size, nodal status or basal phenotype [21].
Gonzalez-Angulo and colleagues, utilizing reverse-phase protein arrays to measure AR levels, demonstrated that higher AR expression was associated with an older age at diagnosis, coexpression of ER or PR (p < 0.001) and lower grade tumors (p < 0.001) [33]. The AR was prognostic for overall (p = 0.004) and recurrence-free survival (p = 0.0002). When controlled for ER/PR status, HER2 expression, presence of a <i>
To assess both the prognostic and predictive value of the AR in breast cancer, Loibl and colleagues evaluated 673 core biopsies on a tissue microarray constructed from a subset of 1711 patients with early-stage breast cancer who were treated with neoadjuvant docetaxel/doxorubicin/cyclophosphamide (GeparTrio) [28]. In the TNBC subgroup, AR expression was present in approximately 21% of patients and was associated with improved DFS (AR+ 86% vs AR− 66%; p = 0.0544) and overall survival (AR+ 95 vs AR− 76%; p = 0.0355). In patients with TNBC, who achieved a pathologic complete response, DFS was 100% for those with AR+ tumors versus 79% for AR− tumors (p = 0.197). In patients who were found to have residual disease after neoadjuvant therapy, DFS was 80% for AR+ tumors versus 59% for AR− patients (p = 0.104). Thus, patients with TNBC and AR+ tumors appeared to have a trend towards a superior prognosis compared with patients who had AR− tumors. A small sample size is a limitation of this study. These more recent data, discussed above, would suggest a place for the AR as a prognostic marker.
Loibl
By contrast, Koo
AR in breast carcinogenesis
Epidemiologic and preclinical studies suggest that androgens have a role in breast cancer development. An increased risk of breast cancer has been noted in postmenopausal women with elevated levels of circulating estrogen and androgens [22,38,39]. In addition, administration of androgens for cystic breast disease increases breast cancer risk [40]. Wong
Several studies correlate higher levels of the AR with a survival advantage and markers of low-grade disease and advanced differentiation. This would suggest that androgens have a tumor-suppressive, growth-inhibitory effect. Indeed, historically, early studies reported a 15–30% incidence of disease regression in breast cancer patients treated with androgens [44–46]. By contrast, AR antagonism has shown an efficacy signal when used for the treatment of AR-dependent advanced breast cancer. Furthermore, observational data, as discussed above, suggest that administration of androgens can be carcinogenic.
Reconciling these observations is complex. Emerging, albeit limited, data would suggest that the role of the AR in breast carcinogenesis depends, to a degree, upon the estrogen environment. Circulating androgens are often converted into estrogenic hormones (e.g., testosterone yields 17β-estradiol via the enzyme aromatase); however, they may also act directly as AR agonists. Relative levels of estrogen and androgen in women over time influence the growth and/or involution of breast epithelium. During menopause, when ovarian estrogens are absent, both testosterone and estrogen given individually can stimulate proliferation of breast epithelium, suggesting that testosterone is converted to estradiol. However, when testosterone is given concurrently with estrogen, the stimulatory effects of estradiol are blunted, suggesting that testosterone in this setting is exerting an antiproliferative effect [47,48]. The dual proliferative and inhibitory behavior of the AR within breast tissue leads to differing effects of AR signaling on gene expression [42,49,50]. Tumor proliferation may depend upon the breast cancer molecular phenotype and, specifically, the presence or absence of oncogenic ER signaling [51].
Although this review focuses on the role of the AR in hormone receptor-negative breast cancer, it is important to note that AR-regulated pathways are involved in stimulating the growth of ER−, HER2+ breast cancers. In ERα− breast cancers, AR+ disease tends to coexpress HER2 [22,52]. Using gene-expression microarray studies, Ni
AR as a therapeutic target in TNBC
Preclinical observations led investigators to explore the AR as a therapeutic target in TNBC. Through the use of molecular profiling, multiple groups have described a subset of ER− breast cancer that is characterized by AR expression [54,55].
Farmer
Doane
The MDA-MB-453 cell line is one of the most extensively utilized cell lines to evaluate the functional role of the AR in hormone receptor-negative breast cancer, and is representative of the molecular apocrine subtype described by Farmer
The heterogeneity within TNBC has been further examined by Lehmann and colleagues, who identified six distinct subtypes with unique gene-expression profiles [7]. In their series, 49% of TNBCs were classified as basal-like using an intrinsic gene set. One of the six molecular subtypes identified, luminal AR (LAR), was characterized by high AR mRNA and protein expression, AR downstream effectors/coactivators, and luminal cytokeratins/markers. To further understand the functional role of the AR in this subgroup, four breast cancer cell lines were identified with molecular phenotypes similar to that of the LAR tumors (MDA-MB-453, SUM185PE, CAL-148 and MFM-223). These cell lines were significantly more sensitive to the AR antagonist, bicalutamide, than the basal-like cell lines (IC50 = 227 μM vs IC50 > 600 M; p = 0.007). This observation was replicated in murine models. In addition, cell lines with knockdown AR expression demonstrated decreased cell growth and colony formation, Once again, these data confirm the underlying heterogeneity within the TNBC subgroup and that cell growth within the LAR subtype is driven by AR signaling. Moreover, as previously hypothesized, the AR may prove to be a novel therapeutic target for this subgroup with AR expression serving as a potential molecular marker for preselection of patients for this therapy.
Clinical experience with AR antagonists for the treatment of breast cancer
Bicalutamide
Antiandrogen therapy has previously been evaluated in relatively unselected breast cancer populations [58]. The first study evaluating androgen inhibition in a population of patients with ER−, PR−, AR+ metastatic breast cancer was conducted through the Translational Breast Cancer Research Consortium [16]. The primary objective of this multicenter Phase II study was to evaluate the efficacy of daily oral bicalutamide in patients with AR+, ER−/PR− locally advanced or metastatic breast cancer as defined by clinical benefit rate (stable disease, partial response or complete response for >6 months) [101]. Bicalutamide is an oral nonsteroidal antiandrogen approved by the US FDA in combination with a luteinizing hormone releasing hormone analog for the treatment of advanced prostate cancer. Bicalutamide competitively binds to the AR, stimulating the assembly of a transcriptionally inactive AR and increasing AR degradation [29]. In this study, women with ER−/PR− (<10%) advanced breast cancer were screened for AR status using IHC methods previously described by Doane
More than 400 individuals were screened for AR expression; 12% tested AR+. A total of 26 eligible patients with AR+ ER−/PR− breast cancer went on to the second stage of the study and received bicalutamide. The median age of study participants was 66 years. The median number of prior treatment regimens was one (ranging from zero to eight). The study met its pre-specified end point for efficacy. Clinical benefit rate was 21% (95% CI: 7.1–42.1%). Of the five patients with clinical benefit, one patient has stable disease for more than 4 years and remains on therapy. Another patient of interest had locally advanced breast cancer, which was unresectable after neoadjuvant dose-dense doxorubicin, cyclophosphamide and paclitaxel. Following 6 months of bicalutamide, the patient was able to proceed to curative surgery. Median progression-free survival in the study population was 12 weeks. Therapy was well tolerated, with no grade four or five events observed. The most common toxicities observed were hot flushes, fatigue and elevated transaminases.
This study was the first to specifically test AR inhibition in a population of patients selected for AR+, ER−/PR− breast cancer. Despite limitations inherent to any small single-arm Phase II trial, these results suggest anticancer activity and are hypothesis-generating for further study. Anti-androgen therapy is a potential, minimally toxic treatment option for a select group of patients with AR+ TNBC. Ongoing correlative research from this prospective study is examining potential biomarkers, such as endocrine pharmacodynamic markers, and molecular predictors of response to bicalutamide therapy.
Abiraterone acetate
Another androgen-directed therapy under investigation in AR+ breast cancer is abiraterone acetate. Abiraterone acetate is a potent, specific and irreversible inhibitor of CYP17A1, an enzyme that plays a role in adrenal and gonadal glucocorticoid biosynthesis, thus lowering levels of both androgen and estrogen. Abiraterone acetate is approved by the FDA in combination with prednisone for metastatic CRPC based on a demonstrated overall survival benefit [30,31]
A Phase I study of abiraterone acetate in ER+ or ER−/AR+ breast cancer was presented at the annual meeting of the American Society of Clinical Oncology in 2011 by Basu and colleagues [59]. A total of 25 patients were treated in the study with doses of abiraterone acetate between 250 and 2000 mg daily. With a median time on treatment of 1.8 months (range: 0.7–11.6 months), no dose-limiting toxicities were observed. The majority of adverse events were grade <2, including fatigue, nausea, anorexia, dyspnea, palpitations, dizziness and flushes. Grade 3 hypokalemia occurred in four patients with no reported clinical consequence. Two patients, whose tumors expressed both the ER and the AR, remained on abiraterone acetate for more than 11 months, one of whom achieved a radiological partial response.
Preliminary data from a combined Phase I/II trial of abiraterone acetate was presented at the 2012 Congress of the European Society for Medical Oncology. Similar to the Phase I trial, the Phase II included patients with ER+ or ER−/AR+ metastatic breast cancer [60]. At the time of presentation, enrollment was ongoing in the ER−/AR+ arm of the trial. However, prolonged disease stabilization ≥6 months was reported in one patient (n = 8) with AR+/ER−/HER2+ disease.
An international multicenter Phase II study of abiraterone acetate in ER+ metastatic breast cancer recently completed accrual [102]. This study included approximately 300 postmenopausal women with ER+, HER2− metastatic breast cancer that had been sensitive to a nonsteroidal aromatase inhibitor. Participants were randomized to abiraterone acetate (1000 mg) with prednisone, the combination with exemestane, or exemestane alone. This larger, multicenter Phase II trial may inform the field of the role of androgen in breast cancer through embedded correlative research, albeit for ER+ breast cancer rather than purely AR-dependent tumors.
Enzalutamide
Enzalutamide is an AR antagonist with significantly higher affinity for the AR than bicalutamide [61]. In addition, enzalutamide, a pure AR antagonist, also functions by blocking the nuclear translocation of the AR, inhibiting the recruitment of coactivators, and preventing binding of the AR to DNA and downstream effectors. A Phase III study demonstrated a statistically significant improvement in overall survival in men with metastatic CRPC who had received prior chemotherapy as compared with placebo [62]. As a result, enzalutamide was approved by the FDA for the treatment of patients with metastatic CRPC who have previously received docetaxel.
The effects of enzalutamide have been evaluated in preclinical models of ER−/PR− breast cancer [63,64]. In the ER−, AR+ MDA-MB-453 cell line and xenograft models, enzalutamide treatment caused decreased AR localization, increased apoptosis and tumor growth inhibition [63]. This was also consistently seen in models of dihydrotestosterone-induced tumor growth. Interestingly, enzalutamide also blocked androgen- and estradiol-mediated growth in both
Currently, a Phase I dose-escalation study is under way to establish the recommended Phase II dose and evaluate the safety, tolerability and pharmacokinetics of enzalutamide in women with metastatic breast cancer [103].
Conclusion
An emerging body of evidence indicates that the AR, similar to the ER, may play a significant role in breast cancer carcinogenesis and may thus be exploited for a novel, well-tolerated therapeutic option. This is of particular significance to individuals with TNBC for whom cytotoxic chemotherapy remains the standard, albeit inadequate, systemic treatment. AR-targeted therapies are currently undergoing clinical investigation; results from preclinical and clinical studies of bicalutamide, abiraterone acetate and enzalutamide are hypothesis-generating and warrant further study. Ongoing clinical investigations will continue to clarify the mechanism of the AR in tumor biology and, perhaps, the broader efficacy of AR-directed therapy.
Future perspective
The identification of TNBC as a unique entity of breast cancer has only occurred within the past 5–10 years. Since that time, molecular analysis has led to the rapid recognition that TNBC is marked by heterogeneity and may be further subclassified into subtypes with differing genomic drivers. The LAR subtype has now been described by multiple independent groups. The first clinical trial of androgen inhibition in a group of patients with AR+ TNBC demonstrated clinical benefit.
The coming years will bring improved therapeutic options for patients with TNBC, based upon molecular subclassification. Superior approaches to targeting the androgen-signaling pathway that have been developed for the treatment of prostate cancer may prove to benefit AR-dependent TNBC, such that agents like enzalutamide or abiraterone may find a place in the treatment of a select group of patients with metastatic breast cancer. As the role of the AR is better elucidated with respect to signaling pathway interactions with ER, HER2 and HER3, we may see the use of dual pathway inhibition of ER/AR or HER2/AR to overcome resistance to these fundamental therapies. In addition, we can look forward to a time when androgen antagonism demonstrates a reduction in the risk of AR-dependent TNBC recurrence, much in the same way that selective ER antagonists are a standard of care for ER-dependent cancers.
Financial & competing interests disclosure
Executive summary
The standard treatment of triple-negative breast cancer (TNBC) is limited to conventional cytotoxic chemotherapy.
The androgen receptor (AR) is a ubiquitous nuclear hormone receptor in breast cancer.
The AR has prognostic utility in individuals with TNBC and has been associated with favorable clinicopathologic features in most retrospective series.
A subset of TNBC is characterized by an androgen gene signature.
Preclinical studies have confirmed a subset of TNBC that exhibits AR-dependent, estrogen receptor-independent cell growth.
Early clinical trials have demonstrated clinical benefit with the use of the AR antagonist, bicalutamide, for the treatment of patients with AR+, estrogen receptor/progesterone receptor metastatic breast cancer.