
Abstract
Childbirth is an important event in a woman's life. Vaginal childbirth is the most common mode of delivery and it has been associated with increased incidence of pelvic floor disorders later in life. In this article, the authors review and summarize current literature associating pelvic floor disorders with vaginal childbirth. Stress urinary incontinence and pelvic organ prolapse are strongly associated with vaginal childbirth and parity. The exact mechanism of injury associating vaginal delivery with pelvic floor disorders is not known, but is likely multifactorial, potentially including mechanical and neurovascular injury to the pelvic floor. Observational studies have identified certain obstetrical exposures as risk factors for pelvic floor disorders. These factors often coexist in clusters; hence, the isolated effect of these variables on the pelvic floor is difficult to study.
 Medical Education Online
Medical Education Online
This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of Medscape, LLC and Future Medicine Ltd. Medscape, LLC is accredited by the ACCME to provide continuing medical education for physicians.
Medscape, LLC designates this Journal-based CME activity for a maximum of
All other clinicians completing this activity will be issued a certificate of participation. To participate in this journal CME activity: (1) review the learning objectives and author disclosures; (2) study the education content; (3) take the post-test with a 70% minimum passing score and complete the evaluation at www.medscape.org/journal/wh; (4) view/print certificate.
Learning objectives
Upon completion of this activity, participants should be able to:
Describe risk factors for pelvic floor disorders following vaginal childbirth, based on a review
Describe mechanisms of injury underlying pelvic floor disorders following vaginal childbirth, based on a review
Describe strategies for minimizing risk of pelvic floor disorders following vaginal childbirth, and directions for future research, based on a review
The term ‘pelvic floor disorders’ (PFDs) refers to stress urinary incontinence, overactive bladder syndrome, pelvic organ prolapse and fecal incontinence. These disorders are prevalent in adult women. For example, in the USA, 24% of women are affected by one of these disorders, with 16% of women experiencing urinary incontinence, 3% of women experiencing pelvic organ prolapse and 9% of women experiencing fecal incontinence [1]. The prevalence of these conditions increases significantly with age: 10% of women aged 20–39 years compared with 50% of women aged 80 years or older suffer from at least one of these disorders [1]. The number of American women with at least one PFD is estimated to increase from 28.1 million in 2010 to 43.8 million in 2050 [2]. The lifetime risk of undergoing a single operation for prolapse or incontinence by the age of 80 years in the USA is 11% [3], with a reoperation rate of 30%. Over 225,000 women underwent prolapse operations in the USA in 1997, making this one of the most common indications for surgery in women [4]. The financial burden of these disorders includes both direct (routine care, medical visits and medical treatments) and indirect (loss of productivity) costs. The cost of ambulatory care related to female PFDs is significant and is increasing. Using Medicare reimbursement to estimate medical care costs, the direct annual costs associated with ambulatory care for PFDs was estimated to be US$412 million in 2006 [4]. This was almost double the direct annual cost of US$262 million in 1997. Due to the increasing prevalence of PFDs, it is anticipated that these expenditures will continue to increase in the future. The estimated national annual direct cost for surgical management of pelvic organ prolapse operations was over US$1 billion in 1997 [5], while the annual direct cost of surgical treatment of urinary incontinence was US$1032 million in 1995 [6]. The annual direct cost of surgical treatment for female fecal incontinence was US$24.5 million in 2003 [7]. Although severe morbidity from PFDs is rare, these patients score significantly worse on the prolapse, urinary and colorectal scales and overall score of pelvic floor distress inventory [8]. In addition, pelvic organ prolapse negatively affects women's self-perception of their body image [9]. Thus, PFDs are common and have significant public health impact.
Risk factors for PFDs
Various studies have identified age [1,10,11], vaginal childbirth [12,13] and obesity [14,15] as risk factors for PFDs. Other studies suggest that some PFDs are associated with diabetes [16], connective tissue disorders [17] and neurological diseases [18–20]. Some women have a genetic predisposition to the development of PFDs [21,22].
Given that the biological causes of PFDs remain uncertain, the study of the association between childbirth and PFDs may offer important insights into the pathophysiology of these disorders and may lead to the development of prevention strategies. In this review, the authors focus on the accumulating evidence linking obstetrical events and the incidence of PFDs later in life. Since stress urinary incontinence, fecal incontinence and prolapse are the more common PFDs, this review focuses on the association between these disorders and various obstetrical variables.
It is important to note that, although vaginal delivery appears to be the most important predisposing factor for PFDs, the evidence to support this finding is derived from observational studies because randomized controlled trials comparing different modes of delivery and the number of deliveries are not feasible for various reasons (e.g., patient's preference and the unpredictability of the labor course, among others).
Parity & PFDs
Several studies have shown that PFDs are more common in parous women compared with nulliparous women of the same age, irrespective of the mode of delivery. Hansen
Among parous women, an increasing number of childbirths further increases the risk of PFDs. Kepenekci
Mode of delivery & PFDs
Several studies support that the incidence of PFDs varies with the mode of delivery. MacLennan
In a recent study of parous women, history of a vaginal childbirth was associated with twice the risk of developing bothersome symptoms of stress incontinence compared with women delivered exclusively via cesarean section [13]. In contrast to this finding, the follow-up study of the randomized, multicentered Term Breech trial, which compared maternal outcomes 2-years after planned cesarean section with planned vaginal birth for breech presentation at term, showed no differences in the incidence of urinary incontinence between the two delivery groups (17.8% in the planned cesarean section group and 21.8% in the planned vaginal birth group). In addition, there was no difference in the degree of bother caused by urinary incontinence between the two groups [29].
Vaginal childbirth that is complicated by anal sphincter trauma has been linked to postpartum fecal incontinence. A history of third- and fourth-degree obstetric lacerations was identified as the only obstetrical risk factor for postpartum fecal incontinence in a recent systemic review [30]. However, in the absence of anal sphincter trauma, vaginal delivery does not appear to increase the risk of anal incontinence [31].
Several studies have linked vaginal childbirth to pelvic organ prolapse [13]. In one study, history of a single vaginal delivery was associated with a tenfold increased likelihood of developing prolapse [32].
Compared with other PFDs, the association between mode of delivery and overactive bladder syndrome is not well established. For example, the likelihood of overactive bladder syndrome does not differ significantly in women who underwent vaginal or cesarean birth 5–10 years ago [13].
Other obstetrical events & interventions
Among vaginally parous women, observational studies have identified certain obstetrical factors that may increase the risk of PFDs. These factors include operative vaginal delivery, prolonged second stage of labor, fetal macrosomia and perineal lacerations. These risk factors often occur in clusters (
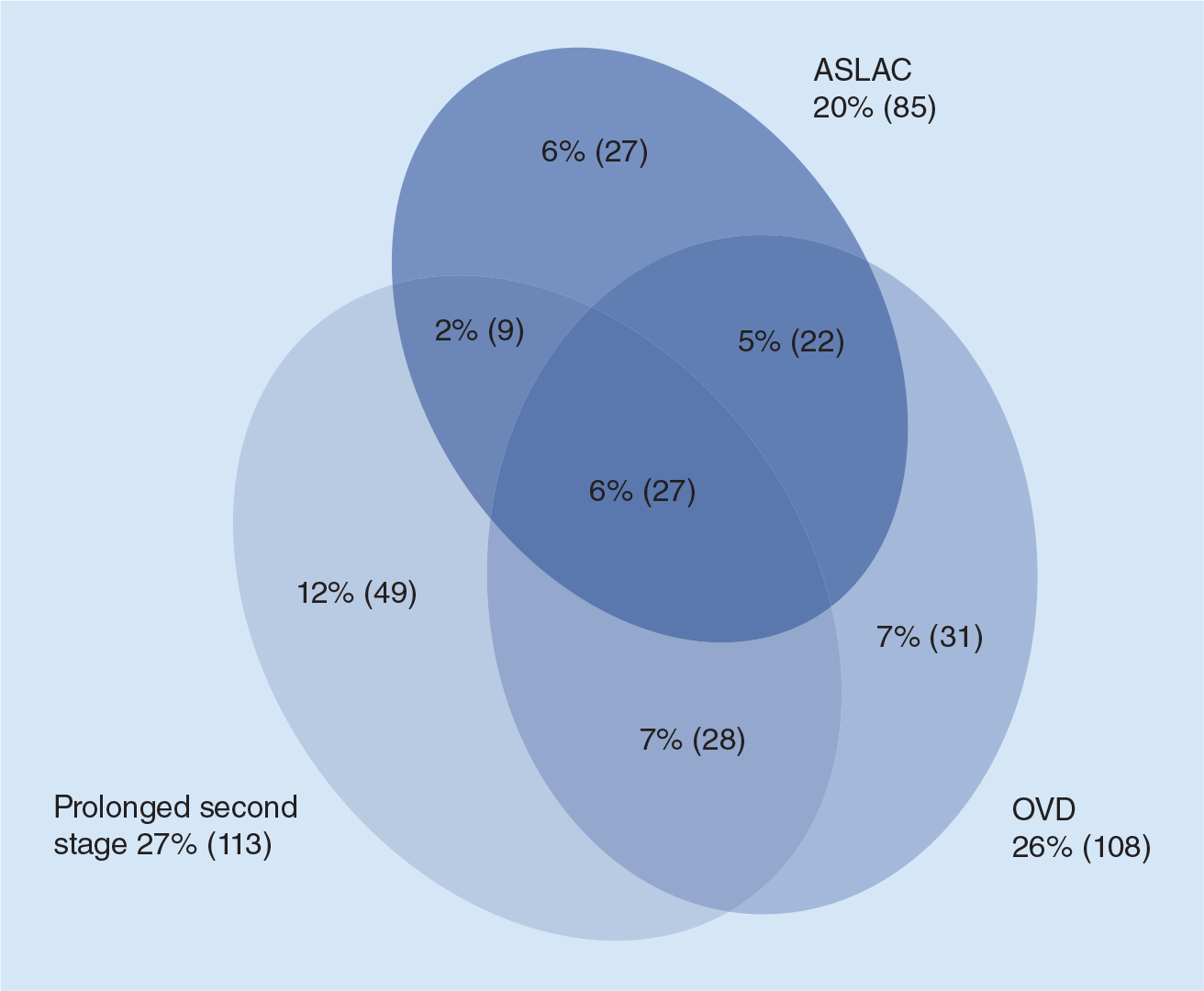
In summary, due to the clustering of some putative risk factors for PFDs, it is impossible to attribute the risk to a single variable. Acknowledging this limitation, the sections that follow review the available evidence for the impact that obstetrical factors have on the development of PFDs among parous women.
Operative vaginal delivery
‘Operative vaginal delivery’ or the ‘instrumental vaginal delivery’ refers to the use of traction devices to assist uterine contractions and maternal expulsive efforts during the second stage of labor to achieve delivery of the fetus. Forceps and vacuums are the most commonly used instruments for this purpose. Indications for operative delivery include a prolonged second stage of labor or the need to shorten the second stage of labor due to nonreassuring fetal status or maternal comorbidity [35], hence operative vaginal delivery can be a surrogate marker for difficult labor.
Operative vaginal delivery significantly increases the risk of PFDs. In a cohort of parous women 5–10 years after delivery, history of operative vaginal delivery was associated with a fourfold increase in the adjusted odds for stress urinary incontinence and overactive bladder syndrome, while adjusted odds for prolapse increased eightfold [36]. Risk of surgical intervention for stress urinary incontinence and prolapse is also higher after operative vaginal delivery. For example, the odds of surgical intervention for stress urinary incontinence is 20-times higher for those who have experienced forceps-assisted delivery compared with women who gave birth exclusively via cesarean [25,37]. Operative vaginal delivery is also a risk factor for anal sphincter injury, which is an independent risk factor for the development of anal incontinence.
In a randomized controlled trial comparing maternal outcomes after forceps versus vacuum delivery, no difference was noted between forceps and vacuum delivery groups in terms of various urinary and bowel symptoms at 5 years postpartum [38]. However, more recent studies have shown that forceps-assisted vaginal delivery is more likely to be associated with overactive bladder syndrome, prolapse [39], subclinical sphincter defects and altered continence [40,41] compared with vacuum-assisted delivery.
Episiotomy & perineal laceration
Episiotomy is an incision on the female perineum that is performed just prior to crowning of the fetal head to increase the diameter of pelvic outlet, thus expediting delivery of the fetus. It is one of the most common surgical procedures experienced by women [42]. A total of 30–35% of vaginal births include episiotomy in the USA [43], while 46% of low-risk nulliparous women in the UK experience episiotomy [44].
Historically, episiotomy was introduced as a strategy to prevent fetal trauma and maternal perineal injury and its routine use gained popularity as it was endorsed by prominent obstetricians in the early 1900s [45,46]. However, research on the relative benefits and harms of routine episiotomy has led to conflicting results. Early advocates of routine episiotomy argued that it protects the mother's perineum, resulting in better postpartum pelvic organ support [47,48]. However, high-quality evidence to support the practice of routine episiotomy is lacking. In a systemic review of 28 prospective studies looking at pelvic floor outcomes after episiotomy, no difference was found in symptoms of urinary incontinence between spontaneous laceration and episiotomy groups. In addition, episiotomy was not found to be protective against fecal incontinence, prolapse or decreased pelvic floor muscle strength [49].
The use of routine episiotomy also started to gain criticism with the appearance of literature suggesting a possible association between episiotomy and third- and fourth-degree lacerations [50]. Helwig
Anal sphincter laceration is an independent risk factor for fecal incontinence. The prospective multicenter CAPS study showed that compared with women who underwent vaginal childbirth without observed injury to anal sphincter, women who had anal sphincter lacerations during vaginal childbirth were twice as likely to develop postpartum fecal incontinence [13]. In addition, women with a sphincter laceration had greater severity of fecal incontinence. More recently, in a prospective cohort study of women who underwent vaginal childbirth without injury to the anal spincter, women who sustained an observed injury to the anal spincter during childbirth are twice as likely to develop postpartum fecal incontinence [13]. More than 90% of the episiotomies in this population were midline.
Mediolateral episiotomy has not been found to increase the incidence of prolapse and urinary and fecal incontinence compared with first- and second-degree spontaneous perineal lacerations and intact perineum [53]. There is also evidence suggesting a protective role of mediolateral episiotomy against the development of central-support defects of the anterior vaginal wall [54]. Hence the role of episiotomy as a risk factor versus a protective factor for the development of PFDs remains unknown, as was concluded by a 2005 systematic review [49].
Another interesting and relevant subject is the role of spontaneous lacerations in the development of PFDs and whether lacerations compared with episiotomy are less traumatic to the perinium. A retrospective cross-sectional survey of women 12 months after vaginal childbirth found no statistically significant differences in the reported levels of urinary incontinence and other pelvic floor symptoms between women with an episiotomy and women with first- or second-degree perineal trauma. This study concluded that women with an episiotomy have similar perineal morbidity to those with a spontaneously occurring laceration [55]. Milsom
In summary, episiotomy and severe perineal lacerations are both markers of a difficult childbirth, and they are often associated with clinical scenarios confounded with operative vaginal birth, fetal macrosomia and a prolonged second stage of labor. Most of the evidence is derived from observational studies. It has been difficult to conduct a randomized controlled trial comparing liberal use of episiotomy with restrictive use of episiotomy and perineal lacerations because of high rates of crossover in interventions between the groups [57]. Hence the role of episiotomy and spontaneous perineal laceration with respect to PFDs remains debatable and requires further investigation.
Prolonged second stage of labor
The second stage of labor is characterized by progressive descent of the fetal head through the completely dilated cervix. This is achieved by the expulsive forces generated by uterine contractions. During these contractions, intrauterine pressure can be as high as 8 kPa. Maternal pushing can further increase intrauterine pressure to as high as 19 kPa [58]. Ischemic necrosis of the pelvic tissues (including nerves and muscles) and stretch injuries, leading to permanent denervation of the tissues, can occur if this pressure continues for an extended duration [59]. Thus, a prolonged second stage may increase soft tissue injury and neuromuscular damage to the pelvic floor. Both of these mechanisms may be central to the pathophysiology of PFDs. This finding is further supported by the suggestion that prolonged pushing for more than 1 h during the second stage of labor is associated with denervation injuries to the pelvis in primiparous women, whereas a passive second stage of labor does not increase the risk for denervation injury [60]. Kearney
Prolonged second stage of labor has been identified as a risk factor for postpartum urinary incontinence in primiparous women [62]. A small Japanese study identified duration of the second stage of labor of more than 30 min as a risk factor for pelvic organ descent in primiparous women [63].
Prolonged second stage of labor has not been directly associated with fecal incontinence, but some studies have shown an increase in incidence of third- and fourth-degree lacerations with prolonged duration of second stage of labor [64]. As discussed above, these severe perineal lacerations are risk factors for anal incontinence. This increase in severe perineal lacerations is most likely a result of obstetric interventions, such as operative vaginal delivery, to manage the prolonged second stage of labor. Adjustment for these factors has been shown to eliminate the association between prolonged second stage and anal sphincter injuries [65].
It is critical to understand that a prolonged second stage of labor is often associated with fetal macrosomia, occiput posterior position, operative vaginal delivery and the use of episiotomy. Hence the observed association between PFDs and prolonged second stage of labor may represent a combined effect of the above factors.
Fetus-related factors
Several studies have reported an association between higher birth weights and postpartum urinary incontinence [66,67]. Viktrup
Maternal age
Delayed childbearing has been identified as a risk factor for PFDs in several studies. Kuh
In summary, several obstetrical and non-obstetrical factors contribute to the association between vaginal childbirth and PFDs. These factors often coexist and the individual contribution of these variables may be difficult to assess. Our knowledge on this subject is based on observational studies because randomized trials cannot control for some of the risk factors discussed above.
Mechanism of obstetrical injury
Preservation of the function of pelvic viscera depends upon the interaction between the anatomical as well as neurological integrity of the organs and their support systems. For example, the maintenance of urinary continence depends on the anatomical and functional competence of the urethral sphincter and integrity of the urethral coaptation mechanism, as well as structurally and neurologically intact urethral support system (levator muscles and endopelvic fascia, among others). Loss of any of these components can lead to incontinence. The trauma to the pelvic floor during childbirth that predisposes women to develop PFDs appears to be multifactorial, as shown in

Multifactorial nature of obstetrical trauma leading to pelvic floor disorders.
Mechanical injury to the pelvic floor
Mechanical support to the pelvis is provided by the muscles of the pelvic diaphragm, endopelvic fascia and its lateral condensations (arcus tendentious fascia pelvis and pelvic ligaments), and their bony attachments. The levator ani muscle complex, which consists of the pubococcygeus, puborectalis and iliococcygeus muscles, is the largest muscle of the pelvic floor and a critical component of the pelvic floor support system. This muscle complex forms a U-shaped sling around the urethra, distal vagina and rectum, thus providing support to these structures. The normal baseline activity of the levator ani muscle keeps the urogenital hiatus closed against the opening action of intra-abdominal pressure. A maximum voluntary contraction of the levator ani muscles further increases the vaginal closure force by 46%, leading to further compression of the rectum, distal vagina and urethra behind the pubic bone [76]. Damage to levator ani muscles may lead to the widening of the urogenital hiatus and downward descent of the pelvic organs. Several MRI [77] and ultrasound studies have shown increased odds of levator ani muscle injury in women with pelvic organ prolapse [78]. Increased prevalence of levator ani muscle injury has also been shown in women with stress urinary incontinence [79].
Vaginal childbirth has been identified as a risk factor for levator injury. Overstretching and damage to the levator muscle, particularly to the pubococcygeal muscle, which is the shortest and most medial component of levator ani complex, has been linked to vaginal delivery [68]. Operative vaginal delivery further increases the risk of levator ani injury [80]. Increase in the incidence of levator ani muscle injury has been listed as one of the potential explanations for the observed association between older age at first birth and higher incidence of PFDs. Dietz and Simpson performed 3D ultrasounds on vaginally parous women who presented with symptoms of PFDs. Women with evidence of levator muscle trauma on 3D ultrasounds were older than women without evidence of levator trauma (mean age: 25.5 vs 23.5 years) [81].
Denervation injury
The pudendal nerve innervates the external urethral and external anal sphincter, and hence plays an important role in maintaining continence. Due to its relative superficial anatomical location in the female pelvis, the pudendal nerve is at risk of injury during vaginal injury. Stretching and compression injury to the pudendal nerve has been reported with 38–42% of vaginal deliveries [82]. Concentric needle electromyography in women with a history of vaginal delivery has shown evidence of transient denervation of the pelvic floor [60]. The majority of pelvic floor injuries are reversible and reinnervation, as indicated by increased density of neurofilaments, leads to the return of continence in the postpartum period [83]. However, if there is a complete transaction or a severe crush injury to the pudendal nerve, return of function may be delayed [84]. Several studies (animal and human) have implicated childbirth injury to the pudendal nerve as an etiology for postpartum urinary and fecal incontinence. Kerns
Connective tissue remodeling
Defects in the endopelvic fascia have been reported in patients with anterior vaginal wall prolapse and stress urinary incontinence. Richardson
The endopelvic fascia and other connective tissue elements of the pelvic floor are at risk of stretch and detachment from their bony attachments during childbirth. During pregnancy, the pelvic floor undergoes hormone-mediated physiological changes in its biomechanical properties, resulting in increased distensiblity of the vagina. Animal models have shown that the vaginal wall and its supportive tissue complex is more distensible and less stiff during pregnancy [91]. This process is mediated by increased synthesis of collagen and elastin by fibroblasts. Collagen and elastin are two main components of the extracellular matrix of the connective tissue. Collagen determines the tensile strength while elastin contributes to tissues' ability to stretch. Fibroblasts are sensitive to mechanical stretch and connective tissue synthesis is proportional to the degree of stretch. Excessive stretching of the vaginal wall initiates a degradative response mediated by release of collagenases from activated fibroblasts. This results in increased degradation of collagen, as well as other constituents of the vaginal wall. Thus, difficult or prolonged labor may exceed the stretch limits of the soft tissue, causing imbalance in the reparative and degradative processes and increasing susceptibility of pelvic floor supportive structures to birth trauma [92].
After delivery, there is substantial remodeling of the connective tissue components. This is accomplished by an increase in collagen and elastin synthesis; however, the new tissue that results from healing after childbirth is not as strong as the original tissue that it replaces. Defects in the process of remodeling of the vaginal wall after childbirth have been investigated as a possible mechanism for the development of PFDs. In animal models, impaired elastin synthesis has been shown to be associated with development of prolapse [93]. Differential expression of genes involved in elastin metabolism was noted in vaginal tissue of women with stress urinary incontinence [94]. Similarly, changes in the composition of collagen have been reported in women with prolapse [95]. It is unclear whether these observed differences in the connective tissue of women with PFDs are the cause or the result of these disorders. Thus the clinical relevance of ‘knockout’ mice models (e.g., those with impaired elastin metabolism) is uncertain.
Conclusion & future perspective
PFDs are common conditions and are responsible for significant financial and emotional burden to patients and the healthcare system. Current literature suggests a strong association between vaginal delivery and both stress urinary incontinence and prolapse. Observational studies have identified certain obstetrical exposures, which appear to be more traumatic to the pelvic floor, particularly forceps delivery, prolonged second stage of labor and sphincter lacerations. Randomized controlled trials to study the effect of individual variables are not practical. Some potential risk factors such as maternal age, occiput posterior position and fetal weight, are nonmodifiable. However, in the light of currently available data, efforts should be directed toward avoiding exposure to modifiable risk factors, such as minimizing the use of forceps, shortening duration of active pushing in the second stage of labor and increased vigilance for anal sphincter injuries. Whether these efforts will result in a reduction in the incidence of PFDs is an interesting area for future research.
Executive summary
Vaginal childbirth and parity appear to be important risk factors for the development of pelvic floor disorders (PFDs), such as stress urinary incontinence and pelvic organ prolapse.
Obstetrical exposures, such as operative vaginal delivery, prolonged second stage of labor, fetal macrosomia and perineal lacerations, often coexist. Hence, the isolated effect of these variables on the pelvic floor is difficult to study.
Trauma to the pelvic support system, denervation injury, ischemia, combined neurovascular injury and defective soft-tissue remodeling are some of the mechanisms that may explain the association between vaginal delivery and PFDs.
Studies are needed to understand the relative contribution of episiotomy and perineal lacerations with respect to prolapse.
Pathophysiologic mechanisms underlying the association between PFDs and childbirth need further investigation. For example, whether the observed differences in connective tissue components of women with and without PFDs are a consequence or the cause of these disorders is an interesting area of research.
Footnotes
Vaginal childbirth and pelvic floor disorders
To obtain credit, you should first read the journal article. After reading the article, you should be able to answer the following, related, multiple-choice questions. To complete the questions (with a minimum 70% passing score) and earn continuing medical education (CME) credit, please go to www.medscape.org/journal/wh. Credit cannot be obtained for tests completed on paper, although you may use the worksheet below to keep a record of your answers. You must be a registered user on Medscape.org. If you are not registered on Medscape.org, please click on the New Users: Free Registration link on the left hand side of the website to register. Only one answer is correct for each question. Once you successfully answer all post-test questions you will be able to view and/or print your certificate. For questions regarding the content of this activity, contact the accredited provider,