
Abstract
Objective:
Pelvic floor dysfunction has a high prevalence among women worldwide. However, in the Kingdom of Saudi Arabia, it is underreported. Thus, we aimed to estimate the prevalence and risk factors of pelvic floor dysfunction in women in the Kingdom of Saudi Arabia.
Methods:
We conducted a cross-sectional study on literate non-pregnant women aged ⩾18 years who agreed to participate in our survey. We used the validated and translated Australian pelvic floor questionnaire and conducted a multivariate logistic regression analysis to assess the risk factors of pelvic floor dysfunction.
Results:
A total of 824 participants completed the questionnaire. While 60.2% of the participants had pelvic floor dysfunction, 67.7% reported signs of bowel dysfunction. Urinary dysfunction, prolapse, and sexual dysfunction were present in 44.1%, 67.7%, and 55.4% of the participants, respectively. Age, high body mass index, chronic medical illness, heavy weight lifting, and multiparity were found as the risk factors of bladder function problems. Meanwhile, chronic medical illness, heavy weight lifting, and multiparity were found as the risk factors of bowel dysfunction and prolapse. Age group and marital status were the independent factors associated with sexual dysfunction.
Conclusion:
We noted a high rate of pelvic floor dysfunction in the Kingdom of Saudi Arabia, which calls for the need to provide holistic approaches for the prevention and management of pelvic floor dysfunction among women.
Keywords
Introduction
Pelvic floor dysfunction (PFD) can cause a variety of conditions, including urinary incontinence (UI), fecal incontinence (FI), pelvic organ prolapse (POP), sensory or emptying abnormalities of the lower urinary tract, defecation dysfunction, sexual dysfunction, and chronic pain syndromes. These conditions can present separately or can coexist. 1
Twenty-five percent of women in the United States have at least one of the aforementioned conditions. 2 Among them, stress urinary incontinence (SUI) is the most common, with a prevalence of 17% in the general population. 2
Overactive bladder is one of the forms of PFD, with an estimated prevalence of 7.6% to 13%.3,4 SUI, POP, and FI have an estimated prevalence of 1.7% to 35.5%,5,6 2.9% to 20%,2,5 and 0.2% to 13%,7,8 respectively. Nonetheless, data on the prevalence of other forms of PFD are limited.
Age, ethnicity, multiparity, mode of delivery, history of pelvic surgery, pregnancy, chronic cough, obesity, spinal cord disorders, family history, and genetics are the most common identifiable risk factors of the development of PFD. 9 They are usually associated with high numbers of pregnancies and deliveries10,11 and heavy lifting.7,12
It is believed that the tendency to develop PFD increases with age. It occurs mostly after women reach the age of 55 years.13,14 However, there are recent data showing that PFD can develop in women at a different age group. Almousa and Bandin van Loon 15 reported that the prevalence of UI among nulliparous adolescent and middle-aged women ranged from 1% to 42.2%. Meanwhile, Batmani et al. 16 reported that the prevalence of UI among older women was approximately 37.1%.
Women with PFD report serious social, economic, physical, and psychological problems that considerably reduce their quality of life (QoL) and productivity.17,18
The total population of the Kingdom of Saudi Arabia (KSA) is 35,498,167. The largest population lives in Riyadh regions (4,205,961). 19 In 2020, women constitute 42.17% of the total population in the KSA. 20
In 2012, Altaweel and Alharbi 21 reported that 29% of women in Riyadh developed UI, and >10% of them reported a marked effect of UI on their QoL.
Despite the widespread recognition of the above-mentioned problem by health experts, no studies have yet assessed the magnitude of PFD in our country. Thus, this study aimed to assess the prevalence and risk factors of PFD in women in Riyadh, the capital of the KSA.
Methods
Study design and participants
We conducted a cross-sectional survey among non-pregnant women aged ⩾18 years. All participants were literate and agreed to participate in the survey conducted in Riyadh, KSA. We excluded women who were aged below 18 years, pregnant, or illiterate. The study was conducted following the recommendation of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement 22 and approved by the institutional review board of Princess Nourah Bint Abdulrahman University (number: 190198). Written informed consent was obtained from the study participants.
Survey tool
We used the electronic Australian pelvic floor questionnaire and conducted the survey between 9 November 2019 and 14 March 2020. The questionnaire assesses four components of PFD; 23 in this study, it was initially translated to Arabic and has been validated in previous studies. 23 The questionnaire consists of six sections comprising 63 questions. There are 18 questions on demographic data and potential risk factors, which include area of residency, nationality, age, marital status, educational level, occupation, smoking status, monthly income, weight, height, history of medication with laxatives and nonsteroidal anti-inflammatory drugs, number of spontaneous vaginal delivery (SVD), number of cesarean section, history of instrumental delivery, age at first pregnancy, number of episiotomies, history of heavy weight lifting, health issues (hypertension, diabetes, arthritis, bronchial asthma, stroke, multiple sclerosis, depression, and allergy), and history of abdominal surgery or perineal surgery (Supplemental Material). In addition, there are 43 questions on bladder, bowel, and sexual functions and prolapse symptoms.
The calculated sample size for the descriptive analysis was 350 participants based on the assumption that the prevalence of PFD is 20%, with 5% level of precision for the 95% confidence interval. The formula used for the sample size was as follows: n = (PQ/L)2 × (Zα)2, where P is the prevalence of PFD; Q, 1 – P; L, width of the confidence interval; and Zα, standard normal deviation at α = .05. The sample size was enhanced by 10% by taking into account the non-response. Our assumption was based on the international evidence of the prevalence of PFD (i.e. 20%–23%). 24 The target sample size was 1050, which was chosen as the highest sample size, among different sample sizes which were calculated in relation to bivariate analysis. A total of 886 (84.4%) participants answered the survey. We included 824 participants after excluding those with missing data.
Data collection
Data collected from the participants were kept confidential and anonymous.
We invited the participants to take part in the survey by sending links through email and social media platforms, such as WhatsApp, Twitter, and LinkedIn.
Statistical analysis
Data were entered into Microsoft Excel and analyzed using the SPSS statistical software, Version 24.0 (IBM, Inc., Chicago, IL, USA). Descriptive statistics (means, standard deviations, frequencies, and percentages) were used to describe the categorical and quantitative variables. Pearson’s chi-square test was used to assess the association between the categorical study and categorical outcome variables. We used odds ratios to measure the association between the categorical variables. Moreover, we conducted a multivariate binary stepwise logistic regression analysis to identify the independent factors associated with the prevalence and four components of PFD, namely, bladder dysfunction, bowel dysfunction, prolapse symptoms, and sexual dysfunction. The p values of ⩽.05 and 95% confidence intervals were used to report the statistical significance and precision of the results.
Results
A total of 886 participants completed the survey; among them, we excluded 62 owing to incomplete data. Thus, 824 participants were finally included and analyzed in this study. Approximately 64.1% of the participants were aged <40 years, 79.2% were Saudi nationals, 62.6% were married, and 69.6% were sexually active. Most of the participants had attained post-secondary education. Only 25.2% of the women were employed. In addition, more than 50% of the participants reported a monthly income above 10,000 SR. We recorded a normal body mass index (BMI) in 40.2% of the participants and a BMI indicating overweight and obesity in 32.4% and 25.2%, respectively. Furthermore, the prevalence of smoking was found to be 11%. While 49.2% had health issues, such as hypertension, diabetes, arthritis, bronchial asthma, stroke, multiple sclerosis, and depression, 39.3% had a history of medication with laxatives and nonsteroidal anti-inflammatory drugs. Approximately 51.5% experienced SVDs (1:4) compared with 24.8% who underwent a cesarean section (1:2). Approximately 46.2% of the participants were aged 20 to 29 years during their first pregnancy. We noted one to three episiotomies in 41.3%. Moreover, 57.8% had a history of lifting heavy weights (Table 1).
Sociodemographic and clinical characteristics of the participants.

The prevalence of PFD was 60.2%. In addition, the prevalence of the four components of PFD (bladder function, bowel function, prolapse symptoms, and sexual function) ranged from 20.9% to 67.7%. Bowel dysfunction and prolapse symptoms had the highest and lowest prevalence, respectively (Table 2).
Prevalence of PFD and its components among the women in Riyadh using the Australian pelvic floor questionnaire (n = 824).

PFD: pelvic floor dysfunction; BFPs: bladder function problems.
Prevalence of PFD and its associated factors
Table 1 summarizes the sociodemographic and clinical characteristics of the participants. Based on the bivariate analysis results and unadjusted odds ratios, age group, marital status, occupation, smoking status, presence of health issues, BMI, history of medication, number of SVDs, number of cesarean sections, age at first pregnancy, number of episiotomies, and history of heavy weight lifting were significantly associated with the prevalence of PFD. The odds ratio of having PFD among the women in the age groups of 30 to 39, 40 to 49, 50 to 59, and ⩾60 years was 2.65, 3.93, 3.94, and 2.77 times significantly higher than that among the women in the age group of 18 to 29 years. The odds ratio of having PFD among the married and divorced or widowed women was 6.40 and 2.66 times higher than that of the single women. Similarly, the odds ratio of having PFD was significantly higher in the women who were non-workers and workers, smokers, overweight, and obese and had health issues, a history of medication, a higher number of SVDs, a higher number of cesarean sections, a higher age at first pregnancy, a higher number of episiotomies, and a history of lifting heavy weights than in their counterparts.
Meanwhile, the multivariate analysis with the adjusted odds ratios and 95% confidence intervals demonstrated significant independent associations of marital status, history of medication with laxatives and nonsteroidal anti-inflammatory drugs, and history of lifting heavy weights with the prevalence of PFD. The adjusted odds ratios of having PFD among the married and divorced or widowed women were higher than those among the single women. The odds ratios of having PFD among the women who had a history of medication with laxatives and nonsteroidal anti-inflammatory drugs were 1.75 times higher than that among the women who had no history of medication with these drugs. Furthermore, the odds ratio of having PFD among the women who had a history of lifting heavy weights was 1.72 times higher than that among the women who had no history of lifting heavy weights (Table 3).
Factors associated with the prevalence of PFD among the women.

PFD: pelvic floor dysfunction; OR: odds ratio; CI: confidence interval.
Prevalence of bladder function problem and its associated factors
In the bivariate analysis, there was a significant association of nationality, age group, marital status, presence of health issues, BMI, history of medication with laxatives and nonsteroidal anti-inflammatory drugs, number of SVDs, age at first pregnancy, number of episiotomies, and history of lifting heavy weights with the prevalence of bladder dysfunction. The multivariate binary logistic regression analysis revealed a substantial association of nationality, age group, BMI, history of medication with laxatives and nonsteroidal anti-inflammatory drugs, number of SVDs, and history of lifting heavy weights with the prevalence of bladder function problems (BFPs), including nocturia, urgency, UI, SUI, urgency UI, and/or mixed UI. Therefore, the odds ratio of having BFPs among the Saudi women was 1.54 times higher than that among their non-Saudi counterparts. The odds ratio of having BFPs among the women aged 50 to 59 and >60 years was 2.42 and 1.51 times greater than that among those aged 18 to 29 years, respectively. The odds ratio of having BFPs among the women who were overweight and obese was 1.55 and 1.70 times greater than that among those with a normal body weight, respectively. Furthermore, the odds ratio was 1.79 times higher in the women with a history of medication with laxatives and nonsteroidal anti-inflammatory drugs than in those without. Moreover, the odds ratios were 1.77, 1.86, 2.66, and 2.14 times higher in those with two, three, four, and higher numbers of SVDs than in those without any experience in SVD, respectively. A history of lifting heavy weights was also significantly associated with the prevalence of BFP, with an odds ratio of 1.73 (Table 4).
Factors associated with the prevalence of BFPs among the women.

BFPs: bladder function problems; OR: odds ratio; CI: confidence interval.
Prevalence of bowel dysfunction and its associated factors
The bivariate analysis revealed a substantial association between the above-mentioned variables of bladder function and the prevalence of bowel dysfunction. However, the multivariate binary logistic regression analysis showed an independent and significant association of nationality, presence of health issues, history of medication with laxatives and nonsteroidal anti-inflammatory drugs, number of SVDs, and history of lifting heavy weights with the prevalence of bowel dysfunction. Hence, the odds ratio of having bowel dysfunction among the Saudi women was 1.53 times higher than that among their non-Saudi counterparts. In addition, the odds ratio of having bowel dysfunction was 2.05 and 1.88 times higher in the women with health issues and a history of medication with laxatives and nonsteroidal anti-inflammatory drugs than in their healthy counterparts, respectively. Moreover, the odds ratio of having bowel dysfunction was significantly higher in the women with higher numbers of SVDs (2.04, 2.50, and 3.75 times higher in the women with two, three, and four SVDs, respectively) than in those with no experience in SVD. Furthermore, the odds ratio of having bowel dysfunction was 2.05 times higher in the women with a history of lifting heavy weights than in those without (Table 5). Approximately 51.5% of the women cannot control their flatus, and 54.2% had an overwhelming feeling to empty their bowel.
Factors associated with the prevalence of bowel dysfunction among the women.

OR: odds ratio; CI: confidence interval.
Prevalence of prolapse symptoms and their associated factors
The bivariate and multivariate analyses revealed significant associations of the presence of health issues, number of SVDs, and history of lifting heavy weights with the prevalence of prolapse symptoms. The odds ratio of having these symptoms in the women with health issues was 1.65 times significantly higher than that in the healthy women. Furthermore, the odds ratio was 2.05, 2.91, 3.10, 2.99, and 3.93 times higher in the women with one, two, three, four, and higher numbers of SVDs than in those without any experience in SVD, respectively. The odds ratio was 1.66 times higher in the women with a history of lifting heavy weights than in those without (Table 6).
Factors associated with the prevalence of prolapse symptoms among the women.

OR: odds ratio; CI: confidence interval.
Prevalence of sexual dysfunction and its associated factors
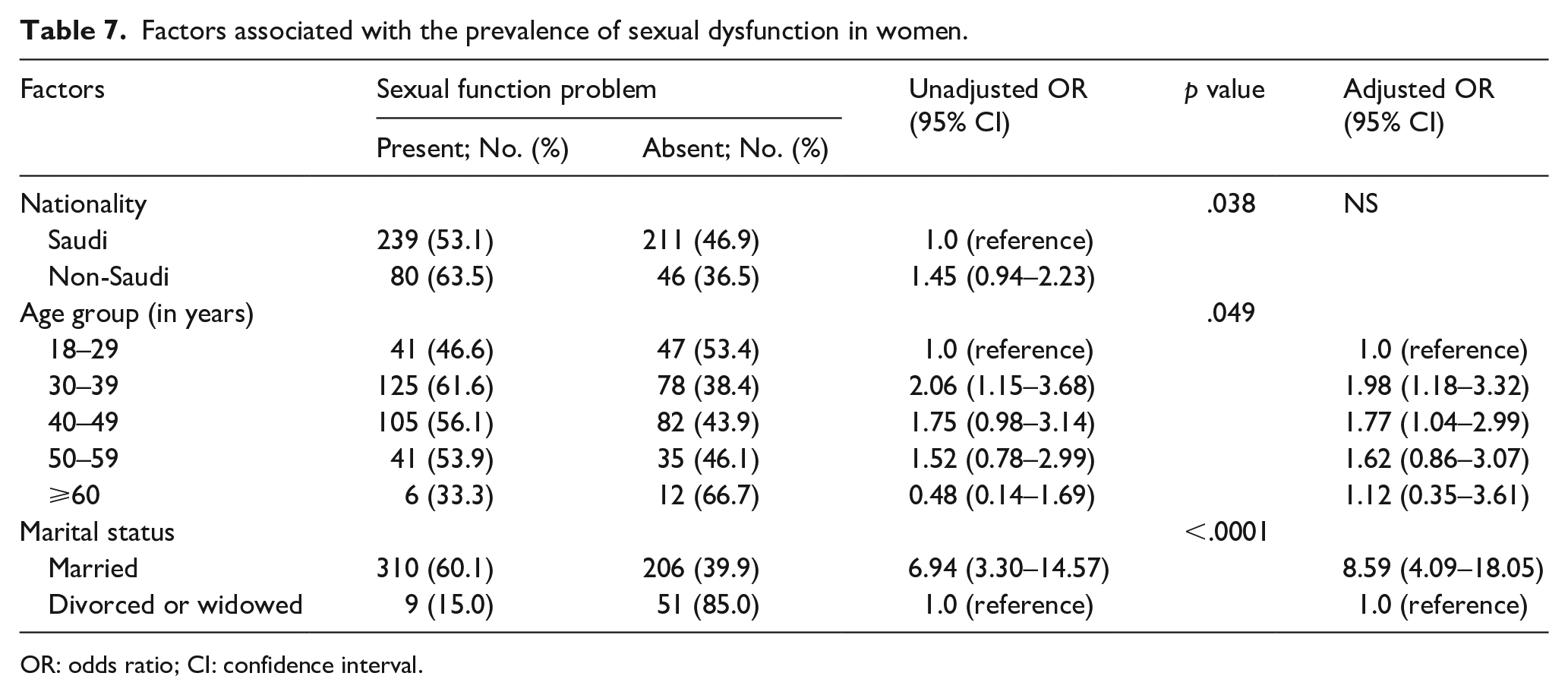
The bivariate analysis revealed a significant association of nationality, age group, and marital status with the prevalence of sexual dysfunction. Age group and marital status were the independent factors associated with sexual dysfunction. The odds ratios of having sexual dysfunction were significant in the 30- to 39- and 40- to 49-year age groups. Meanwhile, the odds ratios were 1.98 and 1.77 times higher in the women aged 30 to 39 and 40 to 49 years than in those aged 18 to 29 years, respectively (Table 7).
Factors associated with the prevalence of sexual dysfunction in women.
OR: odds ratio; CI: confidence interval.
Discussion
PFD is not only a major health problem but also a factor significantly affecting the QoL of a woman during her entire life. 25 This study is the first comprehensive population survey-based cross-sectional study to estimate the prevalence of PFD among women in the KSA. Herein, we also investigated the risk factors associated with the occurrence of PFD in the study population. We found that the prevalence of PFD among the participants was 60.2%. In contrast, the prevalence of the four components of PFD, namely, bladder function, bowel function, prolapse symptoms, and sexual function, ranged between 20.9% and 67.7%. Bowel dysfunction was found to have a high prevalence, while prolapse symptoms were found to have a low prevalence in the studied population.
BFPs were prevalent in 44.1% of the participants. Our results are consistent with those of a US-based study that reported a prevalence of BFPs of 45%. 21 The published estimates of the prevalence of BFPs in the KSA range widely from 29% to 44.25%.25–27 In contrast, the reported prevalence in the Middle East is 30% to 54.8%.28–30
The prevalence in our study was higher than that reported in Qatar, 31 the UAE, 32 and Oman. 33 Nonetheless, it was lower than the prevalence reported in a British study. 34 The lowest prevalence of BFPs has been reported in Singapore. 4 The differences in the prevalence between studies can be attributed to the variation in the study design and population. 33 In addition, the variety and presence of several risk factors among the participants also contribute to this difference.
Bowel dysfunction was prevalent in 67.7% of our female participants. We used a broader definition of anal incontinence, which includes the leakage of gas as well as solid and liquid stool. 35 Our analysis showed the highest prevalence when compared with the results of studies conducted in the UAE, 36 Qatar, 37 Lebanon, 5 Japan, 38 Korea, 39 Malaysia, 40 and Norway. 41 No previous studies have reported the prevalence of female anal incontinence in the KSA. The variations in our results can be associated with the differences in the study samples, definitions of bowel dysfunction, periods over which the prevalence was assessed (4 weeks versus 1 year),5,36–46 and questionnaires used. Furthermore, constipation is one of the risk factors significantly associated with anal incontinence. According to a study among Norwegian women, the prevalence of FI increased in those with chronic constipation than in those without. 41 Moreover, the prevalence of irritable bowel syndrome in the KSA was relatively higher than the results of studies conducted in several other countries.45,46 Furthermore, women experiencing three or more births had a higher prevalence of bowel dysfunction than their counterparts. 47 Childbirth leads to weakness or injury of pelvic floor muscles. As the number of vaginal deliveries increases, the chance of this damage will increase too.
POP is a common condition, with a worldwide prevalence of 30% to 50% in women aged over 50 years. 48 The prevalence of symptomatic POP was 20.9%, which is similar to the results of 30 studies conducted across 15 developing countries. Furthermore, the mean prevalence of POP was reported to be 19.7%. 49 The prevalence of POP was higher in our study population than in Swedish (7.3%–9.1%), 50 Australian (8%), 51 and Pakistani (10.3%) women. 52 Nonetheless, it was lower than that reported in studies conducted in the UAE (29.6%), 53 India (41%), 54 and Tanzania (64.6%). 55
The variation in the above-mentioned prevalence ranges from 7.3% to 64.6%. This can be associated with the differences in the definitions of POP, methods of diagnosis, and methods of classification and inclusion of different age groups. Moreover, the studies were conducted in rural and urban areas comprising different cultures. Furthermore, the condition was diagnosed via an interview, a questionnaire survey, or a clinical examination.
Female sexual dysfunction (FSD) has a major impact on the QoL and interpersonal relationships of patients. It is physically disconcerting, emotionally distressing, and socially disruptive for several women. 56 In our study, we noted FSD in 55.4% of the participants (18–60 years). This prevalence was higher than 43% in the United States as reported by Laumann et al. 57 Meanwhile, Cayan et al. 58 reported an overall prevalence of 46.9% in Turkish women. In contrast, Jaafarpour et al. 59 reported a prevalence of 46.2% in Iranian women. The prevalence of FSD in our study was lower than 64.7% and 67.8% obtained in Jordanian 60 and Egyptian women, respectively. 61 The reported prevalence of sexual dysfunction is higher among married women than divorced and widowed women. This could be explained by conservative and Islamic Saudi culture. It is prohibited for women to have a sexual relationship out of the marriage umbrella.
The differences in the prevalence of FSD between countries may be a consequence of several medical and psychological factors, particularly in the settings of possible socioeconomic, cultural, and racial differences. In addition, the clinical definition used for each dysfunction, type of assessment methods performed (self-reported questionnaire, mailed questionnaire, interview by phone, and personal interview), relationship with the participants’ partners, educational qualification, and characteristics of the samples (general population versus those visiting sexuality clinics) may have contributed to the variation.
The prevalence of PFD increases with age as the body becomes weaker along with the development of other medical problems. Researchers have identified several risk factors for the development of PFD. 62 Age was significantly associated with the prevalence of PFD. This was consistent with the results of studies that reported the presence of at least one symptomatic PFD among women aged more than 40 years.63,64
A higher BMI was associated with a higher prevalence of PFD. Obesity has been previously linked to UI, FI, and POP. Furthermore, weight loss and bariatric surgery reportedly improve UI, while reducing the prevalence of FI. 65 However, weight loss may not improve the bothersome prolapse symptoms. 65 Approximately 33.5% of Saudi women in the KSA are obese compared with 28.0% who are overweight. 66 In our study, 25.2% and 32.4% of the participants were obese and overweight, respectively. Our study emphasized the significance of obesity as a modifiable risk factor. The association of obesity with PFD highlights the importance of addressing weight loss in women who are obese. It also elucidates the significance of screening for these disorders in women who are overweight and obese.
A history of medication with laxatives and nonsteroidal anti-inflammatory drugs and multiparity were found to be significantly associated with PFD symptoms. A prior study has reported an association between a history of medication and an increased risk of POP and UI. 10 Furthermore, our findings regarding the association between multiparity and POP and UI are consistent with those published in prior studies.10,65 A third- or fourth-degree anal sphincter tear and an instrumented delivery consistently increase the odds of having postpartum FI. 2 Moreover, a history of lifting heavy weights was found to be significantly associated with the prevalence of PFD. Weight lifting can lead to overload, weakness, and overstretching of pelvic floor muscles, which can increase the risk of PFD. However, the impact of exercises on PFD had been investigated thoroughly in the literature.67–69 De Mattos Lourenco et al. 70 found that high-impact activities increased the prevalence of UI by 1.9-fold over medium-impact activities. Meanwhile, Bø and Nygaard 71 stated that the impact of physical activities on the pelvic floor differs on an individual basis. We believe that this area should be evaluated thoroughly to reach an appropriate recommendation to the society.
Our study had several strengths, including the prospective study design, use of a validated and translated questionnaire, and representative study population recruited from a tertiary center within a university hospital setting. Furthermore, this is the first study to investigate the epidemiology of pelvic floor–related symptoms and their risk factors in the KSA. However, there are also some limitations that need to be addressed in future studies. Herein, we collected information from participants residing only in Riyadh, most of whom were highly educated and employed. Since an online survey was utilized, women who are illiterate and who do not have an access to the Internet were excluded. This made generalization of our results difficult. Risk factors, such as detailed physical exercises and muscular and neurological illnesses, were not assessed in this study. Moreover, there is a potential of recall bias by responders to some risk factors such as number of episiotomies or detailed history of lifting heavy weight. Large high-quality research that would cover urban and rural areas in the KSA is needed. In addition, the effect of variable risk factors on PFD needs to be thoroughly investigated. The study highlighted the high prevalence of obesity among a population in the KSA and its association with PFD symptoms as well as other diseases. This finding will help in implementing prophylactic strategies to decrease the prevalence of PFD.
Conclusion
Our study noted a high prevalence of PFD in Riyadh, the capital of the KSA. No previous study has assessed all aspects of PFD. Further studies comprising a larger cohort of women should be conducted in other parts of the KSA to obtain more information on this condition and its preventable risk factors.
Supplemental Material
sj-docx-1-whe-10.1177_17455065211072252 – Supplemental material for Prevalence of pelvic floor dysfunction in women in Riyadh, Kingdom of Saudi Arabia: A cross-sectional study
Supplemental material, sj-docx-1-whe-10.1177_17455065211072252 for Prevalence of pelvic floor dysfunction in women in Riyadh, Kingdom of Saudi Arabia: A cross-sectional study by Haifaa Malaekah, Haifaa Saud Al Medbel, Sameerah Al Mowallad, Zahra Al Asiri, Alhanouf Albadrani and Hussam Abdullah in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455065211072252 – Supplemental material for Prevalence of pelvic floor dysfunction in women in Riyadh, Kingdom of Saudi Arabia: A cross-sectional study
Supplemental material, sj-docx-2-whe-10.1177_17455065211072252 for Prevalence of pelvic floor dysfunction in women in Riyadh, Kingdom of Saudi Arabia: A cross-sectional study by Haifaa Malaekah, Haifaa Saud Al Medbel, Sameerah Al Mowallad, Zahra Al Asiri, Alhanouf Albadrani and Hussam Abdullah in Women’s Health
Footnotes
Acknowledgements
We would like to thank Etedal Algenaimi, Fatemah Alhedaithy, Kholoud Alotaibi, Raghad Aldhuwayhi, Areej Alghamdi, Maha Abowadaan, Rawan Alqahtani, and Hadeel Bin Zaid for their help during data collection.
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.