
Abstract
National data from the Asia–Pacific region suggest that stroke accounts for over 10% of female deaths. With general aging in the region, and longer life expectancies for women than men, action is required to maintain recent improvements in female death rates from stroke. However, local data on incidence and risk factors for stroke amongst women are scarce. Data from 214,032 women in the Asia Pacific Cohort Studies Collaboration were thus used to investigate the risk factors for stroke in the region. Raised systolic blood pressure and diabetes were found to be key risk factors for both ischemic (IS) and hemorrhagic (HS) stroke. After adjustment for other risk factors, every extra 10 mmHg systolic blood pressure increased risk of IS by 36% and HS by 69%, whilst diabetes increased risk of IS by 170% and HS by 147%. Smoking was also an important risk factor for IS and HS; risk was reduced by quitting.
Although epidemiological data on stroke are voluminous, the majority of published information comes from western countries, with relatively few data, especially age-standardized incidence data, from the Asia–Pacific region [1], where the largest proportion of the world's population resides. Stroke is the second biggest killer worldwide, accounting for approximately 10% of all deaths in 2004, and is the sixth most important contributor to healthy life years lost [101]. In China, it has been estimated that stroke reduces years of future life by 20–40% whilst, following a stroke, active life may be reduced by as much as 90% [2]. Stroke is predominantly a disease of old age, the total population of the Asia–Pacific region is aging, women generally live longer than men and (perhaps consequent to suffering stroke at an older age) short-term survival after stroke is generally worse for women than men [1,3,4]. Hence the issue of stroke amongst women in the Asia–Pacific region is clearly of huge importance in global public health.
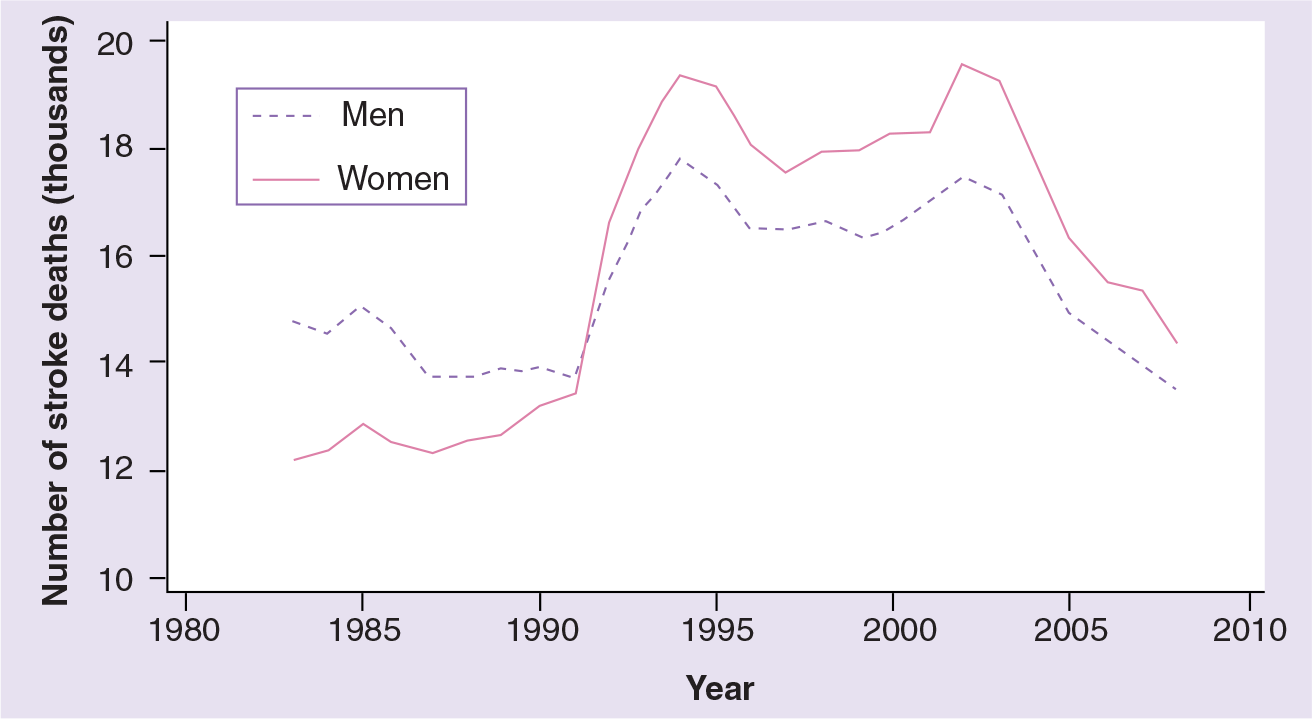
Three examples of the impact of stroke for women in the region will serve as an illustration, bearing in mind that age-standardized incidence and mortality rates are essential to reliably compare time trends within and among nations. In Australia, the number of stroke deaths amongst women has been higher than amongst men for at least 30 years

Fatal strokes amongst women and men in Australia, 1984–2008.

Fatal strokes amongst women and men in Japan, 1951–2009.
Fatal strokes amongst women and men in South Korea, 1983–2008.

Fatal strokes by type as a percentage of all deaths amongst women in Australia, 1998–2008.

Fatal strokes by type as a percentage of all deaths amongst women in Japan, 1951–2009.

Fatal strokes by type as a percentage of all deaths amongst women in South Korea, 1983–2008.
Two issues arise when interpreting findings on the epidemiology of stroke from western countries within the context of the Asia–Pacific region. First, in some countries in the Asia–Pacific region coronary heart disease (CHD) is less common than stroke, unlike Western countries [5]. Second, amongst all strokes, hemorrhagic stroke (HS) is more often observed in Asia than in the western world, where ischemic stroke (IS), with a lower case fatality rate, is far more common. Even so, the relative amount of HS is changing with time, probably due to the epidemiological transition to a western lifestyle [5–7]. Thus, in China, relatively old studies of stroke incidence reported IS percentages of approximately 50%, and HS of 45%, amongst all reported strokes, whereas new studies have found between 44 and 79% for IS and 19–48 for HS [3]. This compares with typical percentages in western countries of 67–81% for IS and 6–20% for HS [8]. HS may well show different associations with risk factors, or even have different risk factors, to IS [9].
Therefore, it is important that stroke subtype is accounted for when assessing risk factors for stroke in the Asia–Pacific region. Unfortunately, this requires expensive investigation, such as CT scans, which may not be available. For example,
This article uses the largest known collaborative study of cardiovascular disease (CVD) and its risk factors, in the Asia–Pacific region, the Asia Pacific Cohort Studies Collaboration (APCSC), to investigate the relationship between putative risk factors and fatal and nonfatal HS and IS.
Methods
Details of the APCSC have been published previously [10]. In brief, studies included had to have a cohort design with selection that was not based upon any disease or risk factor, have baseline information on age, sex and blood pressure, and have cause of death reported during follow-up of at least 5000 person-years. Some cohorts additionally reported nonfatal CVD events. Cohorts suitable for inclusion were classified as from Asia if their participants were recruited from mainland China, Hong Kong, Japan, Singapore, South Korea, Taiwan or Thailand; or ANZ if their participants were recruited from Australia or New Zealand.
The current investigation is restricted to women, but earlier papers from APCSC have reported associations with stroke for men and women combined, often using an earlier (less complete) version of the study database than is employed in this article [11–20]. A further restriction here is that analyses are only given for those major CVD risk factors for which at least 100 IS and HS events were recorded amongst women: diabetes, smoking, blood pressure (only systolic is included here, for brevity), total cholesterol, triglycerides and BMI.
At baseline, the presence of diabetes was determined on the basis of a reported history of diabetes, or by applying the 1999 WHO diagnostic criteria to blood glucose levels at baseline [21]. In one included study (Singapore National Health Survey), diabetes status was also determined by an oral glucose tolerance test. Cigarette smoking status (i.e., current/former/never smoked) was self-reported. Height and weight were measured, rather than self-reported, and BMI was calculated as weight over the square of height (kg/m2). A minority of studies reported repeat measures of some of the risk factors during follow-up.
Most studies used database linkage to identify deaths, while others also included scheduled follow-up visits or examined hospital records, particularly to identify nonfatal events. Outcomes were classified according to the Ninth Revision of the International Classification of Diseases (ICD-9). The outcomes considered in this analysis were: total stroke (430–438); HS (431.0–432.9); and IS (433.0–434.9).
All data provided to the Secretariat were checked for completeness and consistency and recoded, when necessary, to maximize comparability across cohorts. Summary reports were referred back to principal investigators of each collaborating study for review and confirmation.
Statistical analyses
Analyses were based on individual participant data. Cox proportional hazard models, adjusted for age and stratified by study, were used to derive the hazard ratios (HRs), and corresponding 95% confidence intervals (CIs), for each of the six risk factors, both for HS and IS. CIs were computed using the method of floating absolute risks [22]. Fatal and nonfatal events were pooled in the analyses. Continuous risk factors were clustered into four ordinal groups, such that an equal number of events occurred in each group. After these initial analyses, continuous risk factors were represented as continuous variables where the association appeared to be approximately log-linear for both IS and HS; otherwise relatively high and low values were compared. The associations for continuous variables were adjusted for regression dilution bias using the repeat measures data [22]. To compare effects in Asia and ANZ, and to simultaneously see the effects of risk factors after adjusting for others, multivariable Cox models were fitted to data stratified by subregion (Asia/ANZ) and interaction by subregion was tested by adding a subregion by risk factor interaction term to a Cox model, taking the subregions together, for each risk factor in turn.
Results
Of the 44 studies in the APCSC, all but two included women. The other 42 studies involved 214,032 women, of whom 79% were from Asia
Summary of studies in the Asia–Pacific Cohort Studies Collaboration that included women.
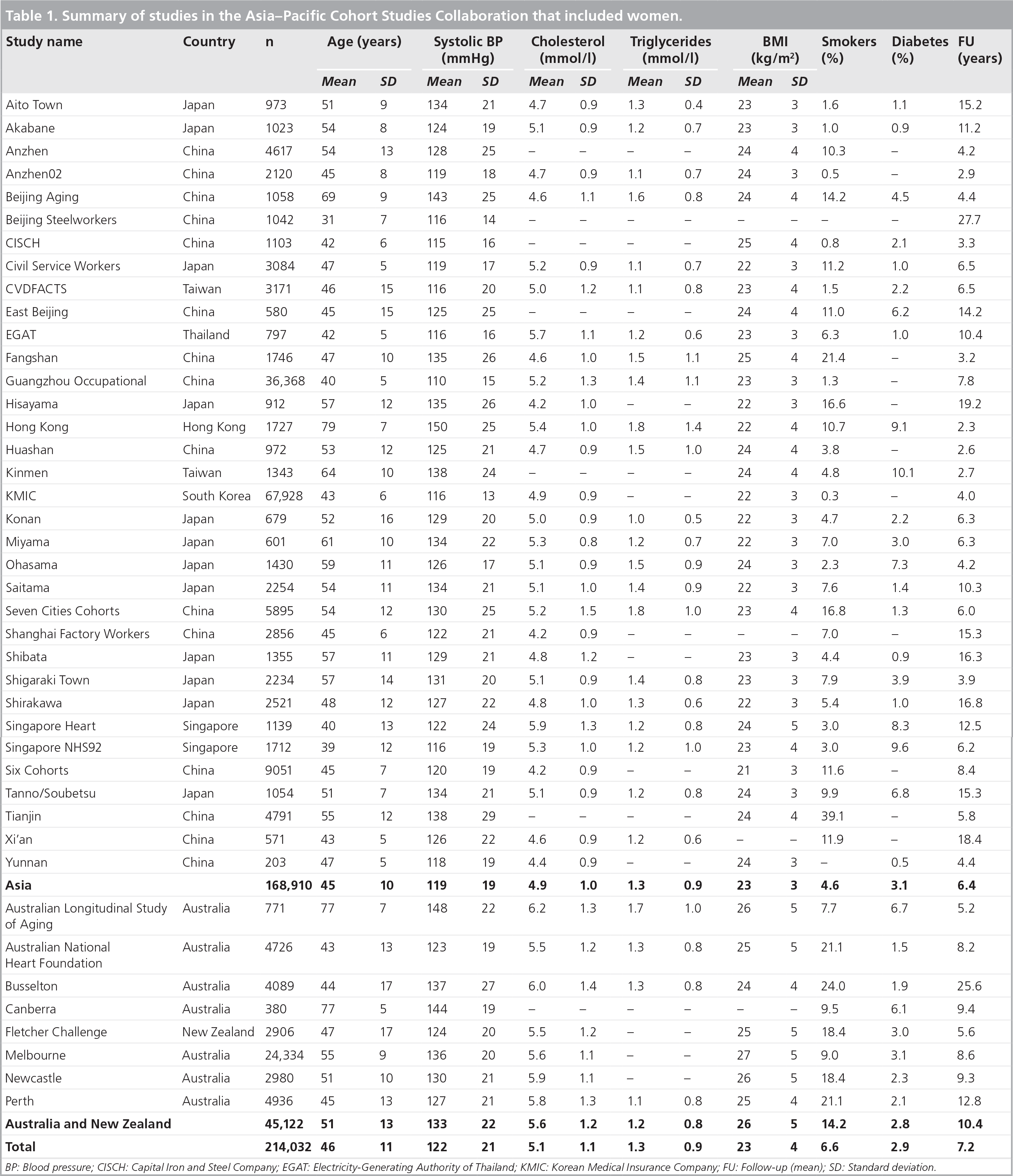
BP: Blood pressure; CISCH: Capital Iron and Steel Company; EGAT: Electricity-Generating Authority of Thailand; KMIC: Korean Medical Insurance Company; FU: Follow-up (mean); SD: Standard deviation.
After adjustment for age, diabetes was significantly (p < 0.05) associated with IS: the HR (95% CI) was 2.40 (1.54–3.74). The corresponding HR for HS was lower and not significantly different from unity at 1.50 (0.73–3.10). The HRs for current smoking versus never smoked, by contrast, were virtually identical for IS, which was 1.35 (1.15–1.58) and HS, which was 1.36 (1.17–1.59), with ex-smokers having a risk, for each subtype, in-between current and never smokers

Age-adjusted hazard ratios for ischemic and hemorrhagic stroke by smoking status for women.

Age-adjusted hazard ratios for ischemic and hemorrhagic stroke by systolic blood pressure group for women.

Age-adjusted hazard ratios for ischemic and hemorrhagic stroke by total cholesterol group for women.

Age-adjusted hazard ratios for ischemic and hemorrhagic stroke by triglycerides group for women.
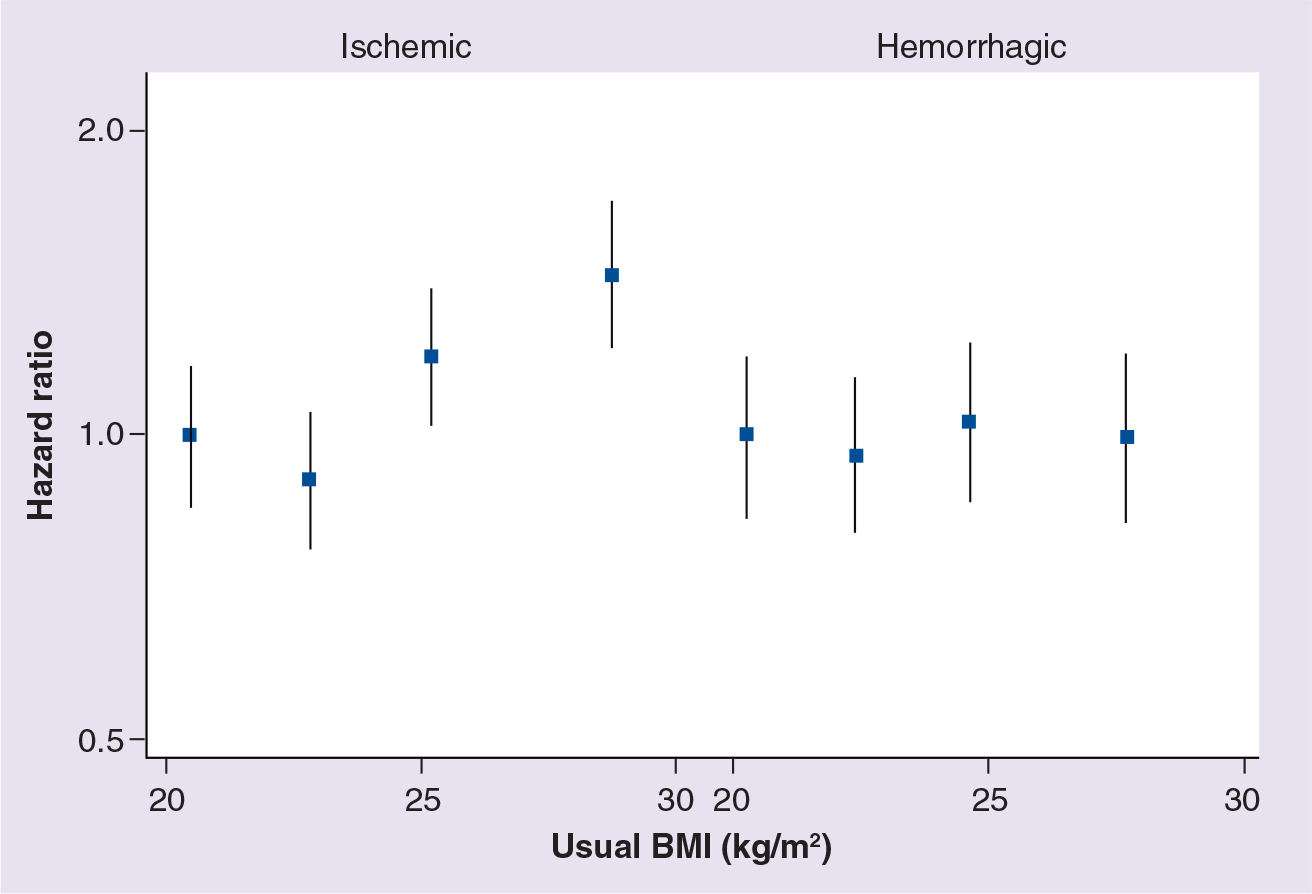
Age-adjusted hazard ratios for ischemic and hemorrhagic stroke by BMI group for women.

Multiple-adjusted hazard ratios for ischemic stroke by subregion and overall.
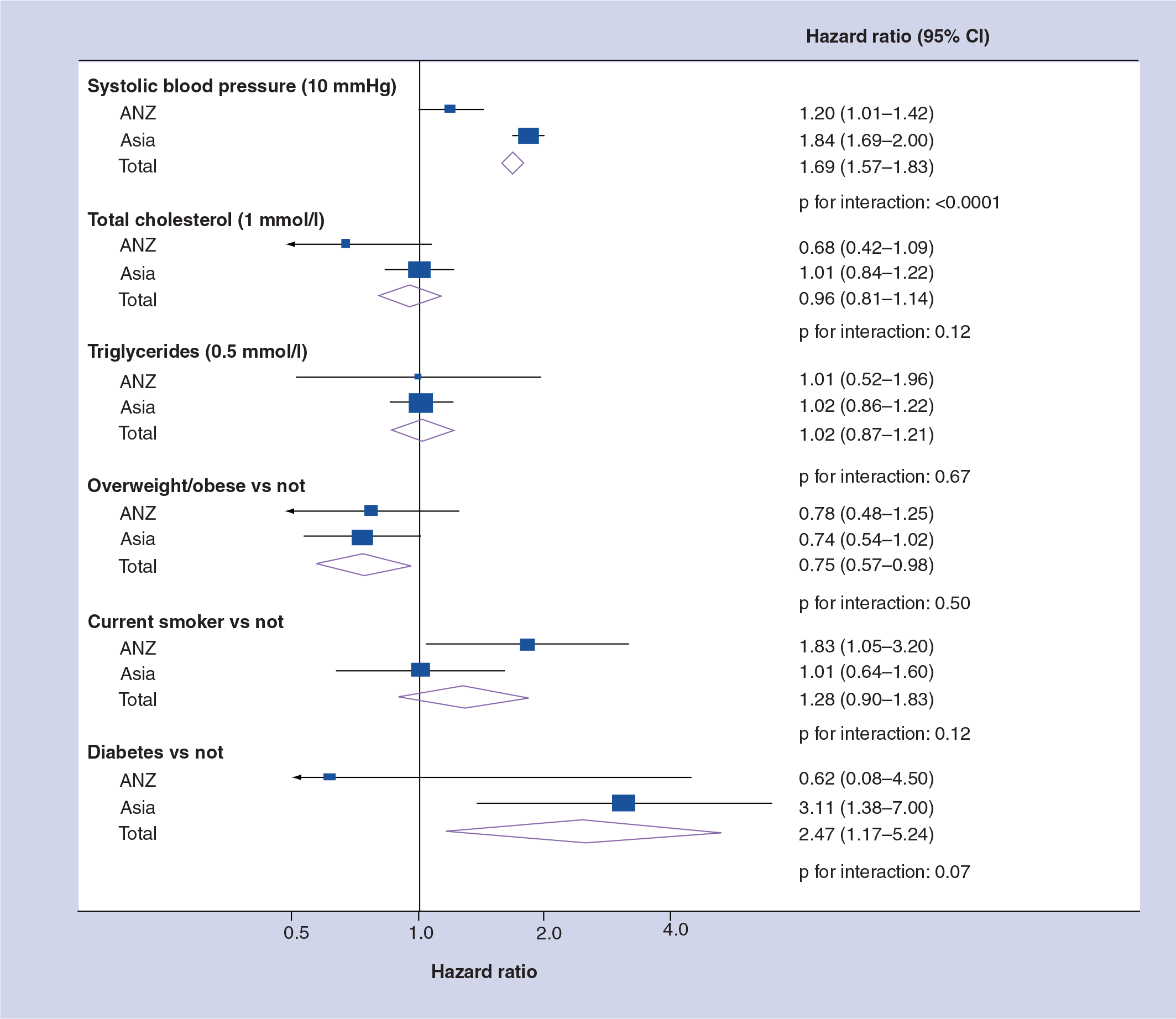
Multiple-adjusted hazard ratios for hemorrhagic stroke by subregion and overall.
The only instance where there was convincing evidence of a real difference between the subregions was for SBP, where the HRs for Asia were significantly higher than for ANZ for both IS and HS. The increase in risk for every additional 10 mmHg was also higher for HS than for IS, most noticeably in Asia (84 vs 44%). For other risk factors, any differences between subregions were explainable by chance except for the triglycerides–IS association, where the point estimate for ANZ was unreliable. There was also a large differential between the sub-regional HRs for HS associated with diabetes, again explained by inaccurate estimation in ANZ, but here the interaction was not quite significant at the 5% level.
Discussion
This study, of more than 200,000 women, has demonstrated that SBP and diabetes are strongly and independently positively associated with both the major subtypes of stroke for women in the Asia–Pacific region. Smoking is the third risk factor of key importance, and, importantly, these analyses provide evidence of a benefit of quitting for women. Overweight/obesity may also be an important predictor of IS, but may have a negative effect on HS. The evidence for any independent positive effect of cholesterol on IS amongst women was weak, whilst there was no evidence of any effect on HS. No evidence was found for any effect of triglycerides on stroke after accounting for other risk factors, in contrast to a recent study of IS in Denmark [23]. Furthermore, there was no firm evidence of differences in effects of risk factors in Asia or ANZ, with the exception of SBP where effects were qualitatively similar, but differed in magnitude such that the associations were sharper in Asia.
Awareness and control of salt in the diet and use of medication to reduce blood pressure has undoubtedly improved in Asia in recent years; for example, Japan has seen reductions in average salt intake in most recent years [24]. This is likely to explain a great deal of the overall reduction in stroke fatalities in several Asian countries [5,6]. The stronger association of SBP with HS than with IS, seen in
Transitions in dietary habits may have had the biggest impact on the IS/HS ratio [5], since increased cholesterol and adiposity may have opposing effects, according to
Diabetes, which is strongly associated with increased body fat, is on the rise throughout the Asia–Pacific region [28]. In this study, diabetes was found to be positively associated with IS after age and multiple adjustment, both in Asia and ANZ. For HS, the evidence was more mixed, but the most compelling analysis, multivariable adjustment using all the data
This study has the advantage of a large sample size, but the disadvantages of lacking both a common protocol across the studies and an objective measure of tobacco inhalation within studies. Whilst stroke was analyzed according to its two major subtypes, HS and IS, etiological differences may occur between subtypes of finer division. For example, a Japanese study has reported low-density lipoprotein cholesterol to be a risk factor for atherothrombotic infarction, but not other types of IS [29]. Furthermore, many cases of stroke in this study were not even able to be classified to one of the two major subtypes.
Future perspective
The implications of the findings presented here are mixed. First, there is clearly a continuing decline in stroke deaths amongst women in the Asia–Pacific region, which suggests that public health and clinical initiatives are already leading to long-term improvements. As well as wholesale changes in stroke deaths for the better, decreases in the relative proportion of deaths due to the hemorrhagic subtype, with its worse prognosis, also point to improvements, although the consequences of a nonfatal stroke are often far from trivial. Data on stroke incidence are rare in the region, and there is a clear need for national registries of stroke, as well as CHD.
The risk factors for stroke of both main subtypes are frequently associated with lifestyle choices, most obviously for smoking. Thankfully, smoking in women is still unusual in most Asian countries, although the prevalence of smoking is on a par with men in Australia and New Zealand [30]. The problem here is that smoking may be portrayed as sexy and empowering to young women, thus requiring sustained vigilance through tobacco control programs. Women are, in many cases in the Asia–Pacific region, primarily responsible for family food choices, storage and preparation. The education of women regarding the risks of excess salt may be the public health strategy with the biggest bang for the buck. Finally, the inexorable rise in diabetes within the Asia–Pacific region is of great concern, with reported national adult rates already as high as 15% [31]. Diabetes is a stronger risk factor for IS amongst women than men [32], and results here suggest it is also an important risk factor for HS amongst women. Hence, actions to control the diabetes epidemic, and to prevent its sequelae, should be expected to have a huge impact on death and disability amongst women from the Asia–Pacific region.
Executive summary
Stroke accounts for more than 10% of fatalities amongst women in the Asia–Pacific region.
In recent years, stroke deaths in the region have been decreasing and the relative number of deaths from hemorrhagic stroke has decreased, relative to ischemic stroke.
Data from women in the Asia–Pacific Cohort Studies Collaboration show that systolic blood pressure and diabetes are the most important risk factors for stroke of both subtypes. Smoking is also a key risk factor, with reduced risk for those who have quit.
Raised BMI is associated with a higher risk of ischemic stroke, but not hemorrhagic stroke.
National stroke registries are needed to monitor incidence and mortality.
Education regarding the dangers from salt used in food preparation and storage can be expected to have a huge impact on reducing stroke rates, especially if backed by government policies.
Tobacco control initiatives, targeted to women's issues, should also help to reduce the risk of stroke amongst women.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.