
Abstract
Pregnancy-induced hypertensive syndromes are an important cause of cerebrovascular diseases during pregnancy. Women with pregnancy-induced hypertensive syndromes are at an increased risk of ischemic and hemorrhagic strokes. Posterior reversible encephalopathy and reversible vasoconstriction syndromes are common. Cerebral venous sinus thrombosis may also occur. Preeclampsia and eclampsia reflect generalized endothelial dysfunction. Prompt diagnosis and identification of patients at risk allows for early therapeutic interventions and improved clinical outcomes.
Keywords
Preeclampsia, eclampsia and the syndrome of hemolysis, elevated liver enzymes and low platelet count (HELLP) may manifest with cerebral ischemic or hemorrhagic events in the pre-, peri- and post-partum periods for stroke during pregnancy [1]. These syndromes are part of a continuum of pregnancy-induced hypertension syndromes. Neurologic events associated with these syndromes are presumed to occur because of impaired cerebral autoregulation that is one of the putative mechanisms for cerebrovascular dysfunction in these pregnancy-related syndromes. The main neurologic manifestations of preeclampsia/eclampsia are headache, visual disturbances (including blurred vision, visual field scotomata and cortical blindness) and seizures. These preeclampsia/eclampsia-related events are a major cause of maternal disability and maternal and fetal death in the USA, and without prompt and aggressive treatment these patients may rapidly decline.
Index case
A 39-year-old gesta one, para one (G1, P1) woman with no prior history of hypertension or renal disease had a seizure 1 week following normal vaginal delivery. She complained of headaches and not feeling well prior to the episode. She was diagnosed with preeclampsia at 37 weeks' gestation. She was also noted to have a platelet count of 80,000 per μl of blood prior to delivery. Liver function tests were normal. She was initially treated with magnesium sulfate, and labetalol was added for blood pressure control. She did not have recurrent seizures and had resolution of blood pressure elevation on follow-up visits. Initial brain MRI and follow-up brain MRI carried out 1 month later are shown in
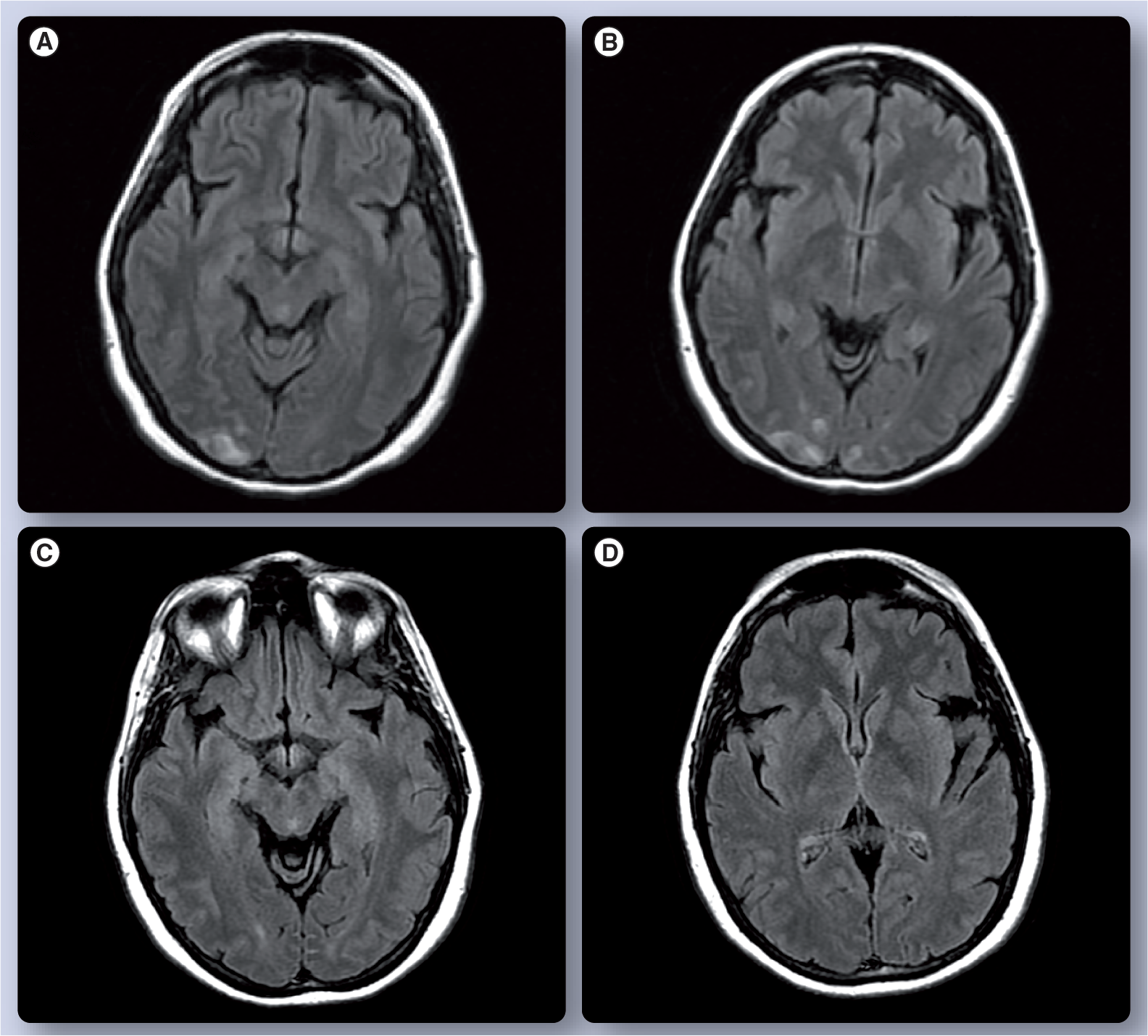
Brain MRI of a 39-year-old woman with postpartum eclampsia.
Epidemiology & definitions
In the USA, preeclampsia/eclampsia affects 5–8% of all pregnant women and is the third leading cause of maternal mortality [2]. Preeclampsia/eclampsia is more common in African–American and Hispanic women than Caucasian women. Advance age is a risk factor for preeclampsia eclapmpsia.
Stroke may complicate hypertensive disorders of pregnancy. Pregnancy is a risk factor for stroke. Compared with nonpregnant women, pregnant women (including the initial 6 weeks postpartum) have a 2.4 times higher stroke risk [3]. The event rate for stroke (excluding subarachnoid hemorrhage) among pregnant women is 34.2/100,000 people in the USA [4].
In a study of 240 Hispanic women with cerebrovascular complications during pregnancy and postpartum, preeclampsia/eclampsia was more commonly associated with intracerebral hemorrhage (57.5%) and ischemic strokes (36%) than with cerebral venous thrombosis (9.6%) [5]. Moreover, there is a higher stroke risk during the first postpartum year following preeclampsia/eclampsia [3].
Pregnancy, by itself, is an independent stroke risk factor [6,7]. In two retrospective series, severe preeclampsia and eclampsia are among the most common causes of pregnancy-related strokes [8]. Pregnancy-induced hypertensive syndromes with abnormally elevated blood pressure may occur throughout pregnancy or the postpartum period. Pregnancy-induced hypertensive syndromes complicate up to 10% of all pregnancies [9,10]. Pregnancy-induced hypertensive syndromes include pre-existing hypertension, gestational hypertension, preeclampsia, preeclampsia superimposed upon pre-existing hypertension and eclampsia. Preeclampsia occurs in up to 8% of all pregnancies in the USA and 14% of all pregnancies worldwide. Pre-existing hypertension exists in an additional 3% of pregnant women and gestational hypertension further complicates 6% of all pregnancies [11].
Pre-existing hypertension, defined as systolic blood pressure (SBP) ≥140 mmHg or a diastolic blood pressure (DBP) ≥90 mmHg, may antedate pregnancy, occur earlier than 20 weeks' gestation or persist for longer than 12 weeks following labor. Pre-existing hypertension may be idiopathic (essential hypertension) or due to an underlying medical condition (secondary hypertension).
Gestational hypertension develops after 20 weeks of pregnancy, and should be resolved by 12 weeks postpartum. By contrast with preeclampisa, gestational hypertension is not associated with proteinuria. Gestational hypertension, however, particularly occurring before 30 weeks' gestation, is a risk factor for preeclampsia in subsequent pregnancies [12].
Preeclampsia is defined as new onset arterial hypertension (SBP ≥140 mmHg or DBP ≥90 mmHg) and proteinuria (≥0.3 g in a 24 h urine specimen) occurring after the 20 weeks' gestation in a previously normotensive woman. Preeclampsia may be mild or severe. Severe preeclampsia is defined by the occurrence of organ damage

Organ dysfunction in severe preeclampsia.
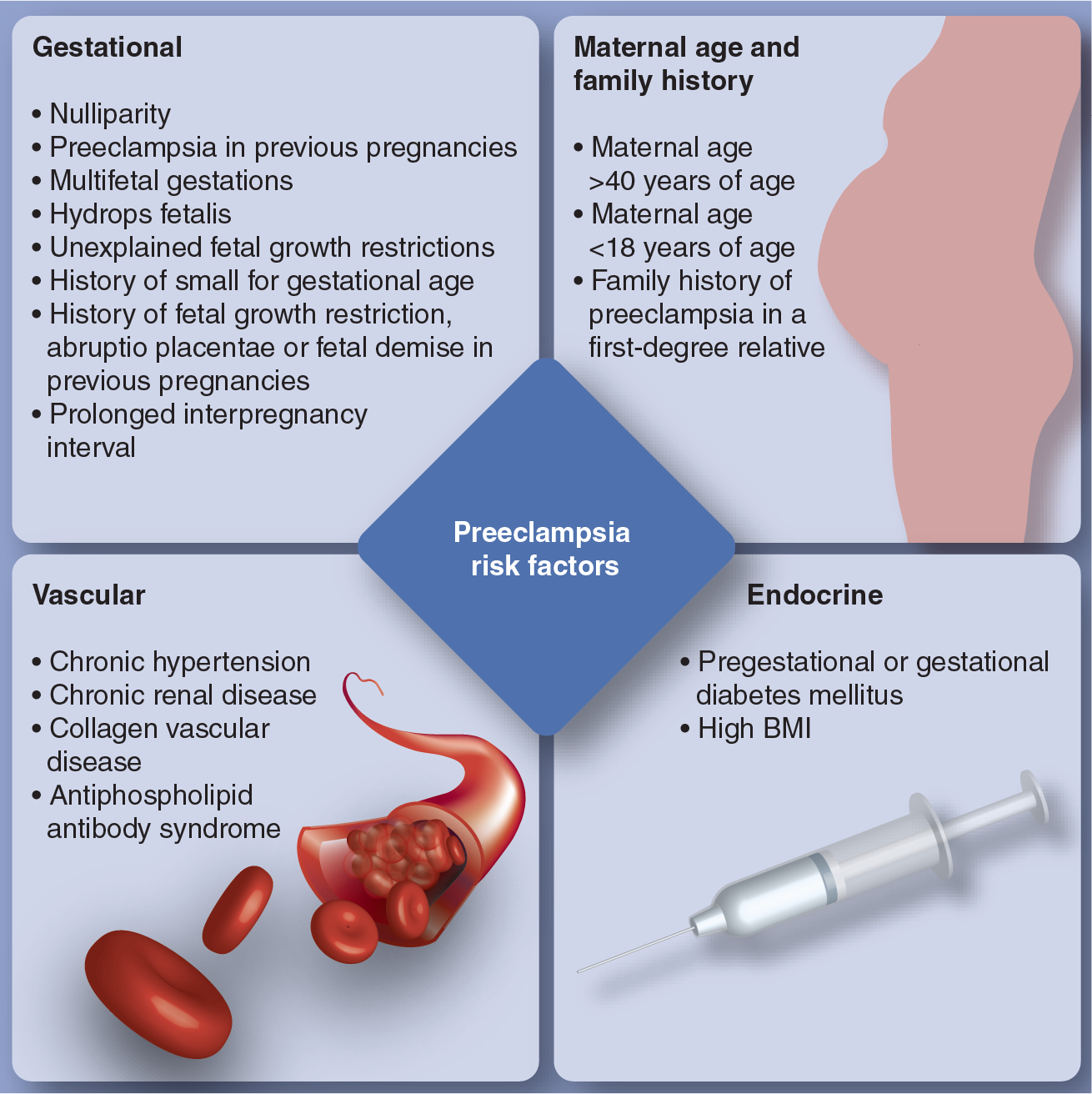
Preeclampsia risk factors.
Hemolysis, elevated liver enzymes and low platelet count syndrome is a severe form of preeclampsia. In addition to cerebral ischemia and hypertensive intracerebral hemorrhage, HELLP syndrome may also lead to intracranial hemorrhage

A 35-year-old woman, gesta one, para one who at 9 h postpartum developed occipital headaches, blurred vision and mental obtundation.
Postpartum cerebral angiopathy is a form of reversible cerebral vasoconstriction syndrome typically occurring within the first week following a normal pregnancy. Headache may be the initial manifestation of this disorder.
Certain medications, including ergots, triptans and bromocriptine, may contribute to postpartum cerebral angiopathy [15].
Pathophysiology of preeclampsia & eclampsia
The exact mechanism for the development of preeclampsia/eclampsia remains unknown. The pathogenesis is probably multifactorial with maternal, fetal and placental factors playing different roles. Many of the clinical manifestations of preeclampsia are explained by maternal generalized endothelial dysfunction. Generalized endothelial dysfunction causes dysregulation of arterial vascular tone (hypertension and vasoconstriction), increased vascular permeability (edema and proteinuria) and abnormal endothelial expression of procoagulant molecules (coagulopathy)

Pathophysiology of preeclampsia.
The specific pathophysiologic mechanisms of preeclampsia/eclampsia-induced cerebrovascular disease are poorly understood. Cerebrovascular disturbances seen in preeclampsia/eclampsia are similar to those seen in hypertensive encephalopathy (HE) and reversible cerebral vasoconstriction syndromes. A predilection to the occipital and parietal lobes describes the variant of posterior reversible encephalopathy syndrome (PRES). A notable difference between HE and PRES is that, in PRES, blood pressure may be normal or marginally elevated. The cerebrovascular disturbances in pregnancy-induced hypertension, HE and PRES include impaired cerebral blood flow autoregulation, hyperperfusion and cerebral edema [16]. Acute elevation of arterial blood pressure impairs arteriolar autoregulatory capacity leading to blood–brain barrier disruption and subsequent edema formation

Brain edema formation in preeclampsia/eclampsia.
Clinical manifestations
Preeclampsia is characterized by the gradual development of hypertension and proteinuria, particularly in primigravid women. It is more common during the third trimester of pregnancy. It may also occur during the partum or postpartum period. Pregnancy-induced hypertension occurring ≤20 weeks' gestation is suggestive of a molar pregnancy rather than preeclampsia.
Arterial hypertension is the earliest manifestation of preeclampsia. Blood pressure elevations usually do not reach hypertensive ranges (≥140/90 mmHg) until 34 weeks' gestation. Whereas the clinical criteria for preeclampsia requires a SBP ≥140 or DBP ≥90, the progression in blood pressure elevation is also important. For instance, a previously normotensive woman with BP readings of 90/60 that has a BP of 135/85 during pregnancy should have close monitoring as she may be at risk for development of proteinuria and further rises in blood pressure. A SBP ≥160 or a DBP ≥110 at two separate intervals at least 6 h apart indicates the development of severe preeclampsia.
The kidneys are the most commonly affected organs by preeclampsia. In normal pregnancy, the glomerular filtration rate (GFR) is increased by almost 50%. Women with preeclampsia have markedly decreased renal blood flow and GFR, although absolute values may remain around the nonpregnant range [19]. However, renal failure is uncommon; increased urinary protein excretion results from dysfunctional selectivity by the glomeruli for protein size and charge [19].
Proteinuria is a required manifestation for the diagnosis of preeclampsia. A minimal amount of proteinuria owing to an increase in the GFR commonly occurs in normal pregnancy. However, levels of >300mg/24 h are pathologic. In mild preeclampsia, proteinuria is ≥0.3 g in a 24 h urine specimen. Proteinuria ≥5 g in a 24 h urine specimen or a urine output ≤500 ml/day indicates severe preeclampsia. Patients with hypertension (≥140/90) without proteinuria should continue to have close monitoring for the development of proteinuria, but 10% of women without proteinuria may have other clinical manifestations of preeclampsia or histological changes of preeclampsia [20]. Eclampsia may also manifest in patients without proteinuria [21]. Other manifestations attributed to renal dysfunction include hyperuricemia, hypocalciuria and podocyturia (urinary excretion of podocytes). Pitting edema may occur with normal pregnancy but facial edema and rapid weight gain (>5 lb per week) warrant clinical evaluation for preeclampsia.
Thrombocytopenia is the most common hematological abnormality observed in preeclampsia. Formation of microthrombi leads to low circulating platelet counts. Severe preeclampsia occurs with platelet count ≥100,000 per μl of blood. Low hematocrit in the presence of schistocytes and helmet cells indicate microangiopathic hemolysis.
Hepatic changes observed in patients with severe preeclampsia include periportal hemorrhages, ischemic lesions and fat deposition. Right upper quadrant or epigastric pain and elevation of liver transaminases are common manifestations of preeclampsia-induced liver injury. In more severe cases, subcapsular hemorrhage or hepatic rupture may occur.
Preeclampsia may also lead to decreased left ventricular performance and coronary ischemia [22,23]. Chest pain or shortness of breath in a preeclamptic patient warrants evaluation for possible myocardial ischemia and cardiomyopathy. Patients are also at risk for pulmonary symptoms related to pulmonary edema; the etiology of pulmonary edema is multifactorial. Mechanisms include elevation of intravascular hydrostatic pressure, decreased intravascular oncotic pressure, capillary leak and left ventricular dysfunction.
Neurologic manifestations
The neurologic manifestations represent a form of hypertensive encephalopathy [24]. The most common clinical manifestations of hypertensive encephalopathy are altered state of alertness and headache. Headache, visual disturbances, focal neurological deficits or seizures may be the initial manifestation to pregnancy-induced hypertensive syndromes [25,26]. Headaches commonly precede seizures in eclamptic women [27]. There is a relationship between history of migraine headache and the development of preeclampsia [28]. Characteristics of headaches are nonspecific, but a persistent headache that does not improve with analgesics should warrant evaluation for severe preeclampsia.
The presence of seizures defines eclampsia. Seizures are usually generalized tonic-clonic, but partial seizures, either simple or complex, may also occur [29]. Postpartum seizures usually occur within 24 h following delivery; however, seizures may manifest up to 8 weeks after delivery [30].
Visual complaints range from blurred vision or visual field cuts to complete vision loss. The predominance of visual disturbances is explained by the predilection of vasogenic edema of the parietal and occipital lobes (cortical blindness) in pregnancy-induced hypertensive syndromes [31–33]. The retina may also be involved. Blindness may precede the onset of seizure activity but may occur in severe preeclampsia not associated with seizure activity. Funduscopic examination may show papilledema or macular edema. Blindness is usually reversible, but permanent vision loss may occur [34]. Balint syndrome is due to bilateral involvement of the parieto-occipital cortex [35].
Coma may occur during eclampsia. Nonconvulsive status epilepticus should be considered in comatose eclampstic patients. Coma may occur in the absence of seizure activity and may be due to intracerebral hemorrhage or cerebral infarction. The Glasgow Coma Score (GCS) and the organ failure score are good outcome predictors in eclampsia [36].
Cerebrovascular complications of pregnancy-induced hypertensive syndromes include ischemic stroke, intracerebral hemorrhage, or subarachnoid hemorrhage and cerebral venous sinus thrombosis (CVST). Preeclampsia is an established risk factor for ischemic stroke and intracerebral hemorrhage, but probably not for CVST [5,37,38]. CVST commonly occurs during the first trimester of pregnancy or 2–3 weeks following delivery. Preeclampsia/eclampsia may be a stroke risk factors years later following pregnancy [7].
Neuroimaging studies in preeclampsia & eclampsia
In general, noncontrast head CT scan and brain MRI are probably safe during pregnancy. The use of intravenous contrast agents are to be avoided unless absolutely necessary. Cranial computed tomography is a useful test in evaluating acute intracranial hemorrhage. Subarachnoid hemorrhage is usually localized to isolated areas in the cerebral convexity [39]. Hypodensities of the subcortical cerebral white matter of the parieto-occipital lobes may be elucidated by cranial computed tomography.
Brain MRI has a higher sensitivity for cerebral abnormalities seen in pregnancy-induced hypertensive syndromes. Hyperintense T2-weighted image/fluid-attenuated inversion recovery signal change without enhancement or restrictive diffusion is commonly seen in the cortex and white matter of the parieto-occipital lobes (case index,
Diagnosis
Blood pressure elevation should be documented on two separate occasions at least 6 h apart. Screening for proteinuria is commonly performed using a urine dipstick sample. A 24-h urine specimen is required for correct quantification and diagnosis of preeclampsia. Protein:creatinine ratios have not been validated to diagnose preeclampsia. Secondary causes of hypertension, proteinuria and organ dysfunction needs to be excluded if clinically suspected. For instance, a pregnant woman with a history of systemic lupus erythematous may have significant blood pressure elevation due to lupus nephropathy or preeclampsia. To date, there are no validated screening laboratory or imaging markers for preeclampsia. Angiogenic factors (e.g., VEGF, sFIt-1 and PIGF, among others) are the most promising laboratory markers for preeclampsia.
Treatment
Aspirin may decrease the risk of developing preeclampsia and perinatal death [41–43]. It is reasonable to start a low dose of aspirin at 12–14 weeks' gestations in patients with preeclampsia risk factors [102]. No other interventions have been proven to prevent the occurrence of preeclampsia.
Pregnancy-induced hypertensive syndromes are a disease spectrum rather than different entities. Patients with ‘mild preeclampsia’ must be treated seriously since lack of prompt treatment may lead to irreversible maternal or fetal organ damage.
Once the patient is diagnosed with preeclampsia/eclampsia, therapies are directed at controlling hypertension, seizure control and management of cerebral edema. Prompt delivery of a viable baby remains the main and only curative therapeutic intervention. General anesthesia for cesarean section in preeclamptic women is best to be avoided unless absolutely necessary. In a population-based study of 8567 preeclamptic women who had undergone cesarean section, general anesthesia was associated with a higher stroke risk as compared with either spinal or epidural anesthesia [44].
Preferred antihypertensive agents are hydralazine and labetalol. Nicardipine or nifedipine may be used as alternatives, but angiotensive converting enzyme inhibitors are to be avoided during pregnancy due to its teratogenic potential. The mean arterial pressure goal is 105–125 mmHg. In most cases of severe preeclampsia, intravenous magnesium sulfate (loading dose of 4–6 g, followed by a maintenance dose of 1–3 g/h) is started prior to labor or cesarean section and continued 24 h postpartum. The Confidential Enquiry into Maternal and Child Health (CEMACH) of 2003–2005 reported 18 maternal deaths related to preeclampsia/eclampsia. Stroke occurred in 12 (ten intracranial hemorrhages and two ischemic strokes) of these cases. The most common cause of intracerebral hemorrhage was uncontrolled hypertension. General anesthesia may be required for emergent caesarean sections during preeclampsia/eclampsia. Additional increase in systemic blood pressure during general anesthesia must be anticipated to avoid intracranial hemorrhage [45].
Magnesium sulfate is the drug of choice for preventing seizures during eclampsia [46]. Eclampsia requires the administration of a 4–6 g loading dose of magnesium sulfate followed by a 2 g/h maintenance dose. The benefit of magnesium sulfate is probably due to antivasospastic effects leading to increase in cerebral blood flow and prevention of ischemic damage. In addition to preventing seizures, magnesium sulfate reduces the risk of maternal death and improves outcomes for the offspring [46]. Only loading dose of magnesium sulfate was also proven to be effective in controlling seizures in a randomized clinical trial [47]. Furthermore, a Cochrane review of 15 randomized clinical trials concluded that the use of magnesium sulfate during preeclampsia reduces the risk of eclampsia by more than 50% [48]. Magnesium sulfate is not recommended for mild preeclampsia. Adverse effects of magnesium sulfate may include hypotension, flaccid areflexic paralysis, hypothermia, respiratory paralysis, hypocalcemia as well as uterine hypotonia. Benzodiazepines should be considered if seizures recur. The routine use of phenytoin/phosphenytoin during eclampsia should be avoided. Even though the mechanism of cerebral vasospasm is theoretically similar to vasospasms due to subarachnoid hemorrhage, magnesium sulfate was not better than placebo in the Intravenous Magnesium Sulfate for aneurysmal subarachnoid Hemorrhage (IMASH) trial [49].
Pregnancy is a relative contraindication for the use of intravenous recombinant tissue plasminogen activator (r-tPA) to treat acute ischemic stroke. Uncontrolled blood pressure of >185/110 mmHg is an absolute contraindication for the use of intravenous r-tPA during acute ischemic stroke. The risks of maternofetal hemorrhagic complications with the use of intravenous r-tPA in preeclamptic/eclamptic women is not known.
Prognosis
The short-term maternal mortality rate in eclamptic patients is increased by several factors. These include HELLP syndrome, acute renal failure, <28 weeks gestational age, African–American race, abruptio placentae, multiparity, comatose state and intracranial hemorrhage [50]. Stroke causes 5% of maternal deaths in the USA [50,51]. Up to 20% of all maternal deaths are attributed to early intracerebral hemorrhage [50]. Short-term fetal mortality rate in eclamptic mothers is increased by the presence of the HELLP syndrome, severity of BP elevation, <28 weeks gestational age, history of preeclampsia, abruptio placentae, intrauterine growth retardation, African–American race and maternal age ≥35 years [52].
Preeclampsia is also predictive of future cerebrovascular and cardiovascular disease. Two systematic reviews quantified the risk of future cardiovascular events in preeclamptic women
Relative risks of developing cerebrovascular disease in women with a history of preeclampsia/eclampsia.

NA: Not applicable.
Long-term neuropsychological sequelae, such as depression and cognitive deficits, may be secondary to cerebrovascular disease induced by hypertensive diseases of pregnancy. In a survey of 128 patients with history of HELLP syndrome, 28% had depression and 26% had anxiety [55].
Conclusion
Preeclampsia and eclampsia are major causes of maternal mortality. Cerebrovascular complications include ischemic stroke, intracranial hemorrhage and reversible cerebral vasoconstriction syndrome. Aspirin may decrease the risk of developing preeclampsia among high-risk patients. Prompt delivery of the offspring, magnesium sulfate and blood pressure control remain the main therapeutic interventions.
Future perspective
Identification of patients at risk of developing pregnancy-induced hypertensive syndromes remain a major research focus. Biomarkers, that increase the risk of stroke during pregnancy-induced hypertensive syndromes may provide clinical guidance regarding early therapeutic interventions. Clinical trials evaluating the safety of intravenous tPA and others in acute ischemic stroke interventions during pregnancy are necessary.
Executive summary
Compared with nonpregnant women, pregnant women (including the initial 6 weeks postpartum) have a 2.4-times higher stroke risk.
The event rate for stroke (excluding subarachnoid hemorrhage) among pregnant women is 34.2/100,000 in the USA.
Preeclampsia/eclampsia is more commonly associated with intracerebral hemorrhage and ischemic strokes, than cerebral venous thrombosis.
There is a higher stroke risk during the first postpartum year following preeclampsia/eclampsia.
The exact mechanism for the development of preeclampsia/eclampsia remains unknown.
A predilection for the occipital and parietal lobes describes the variant of posterior reversible encephalopathy syndrome.
The cerebrovascular disturbances in pregnancy-induced hypertension and posterior reversible encephalopathy syndrome include impaired cerebral blood flow autoregulation, hyperperfusion and cerebral edema.
The neurologic manifestations represent a form of hypertensive encephalopathy.
Headaches commonly precede seizures in eclamptic women.
Postpartum seizures usually occur within 24 h following delivery.
Nonconvulsive status epilepticus should be considered in comatose eclamptic patients.
The predominance of visual disturbances is explained by the predilection of vasogenic edema in pregnancy induced hypertensive syndromes to the parietal and occipital lobes.
Hyperintense T2-weighted image/fluid-attenuated inversion recovery signal changes without enhancement or restrictive diffusion is commonly seen in the parieto-occipital cortical and noncortical regions.
Cerebral angiographic studies may be needed to exclude CNS vascular malformations, including cerebral aneurysms.
Evaluation of the extracranial cerebrovasculature should be considered since cervo-cephalic arterial dissections have been reported in preeclampsia presenting with acute neurological deficits.
To date, there are no validated screening laboratory or imaging biomarkers for preeclampsia.
Aspirin may decrease the risk of developing preeclampsia and perinatal death.
Prompt delivery of a viable baby remains the main and only curative therapeutic intervention.
General anesthesia during preeclampsia has been associated with a higher stroke risk as compared to either spinal or epidural anesthesia.
Magnesium sulfate is the drug of choice for preventing seizures during eclampsia.
Stroke causes 5% of maternal deaths in the USA.
Up to 20% of maternal deaths are attributed to early intracerebral hemorrhage.
Preeclampsia is predictive of future cerebrovascular and cardiovascular disease.
Biomarkers of potential stroke risk during pregnancy induced hypertensive syndromes may provide clinician guidance regarding early therapeutic interventions.
Websites
101. August P, Sibai B: Clincial features, diagnosis, and long-term prognosis of preeclampsia. 2011 Uptodate version 18.3. www.uptodate.com/contents/clinical-features-diagnosis-and-long-term-prognosis-of-preeclampsia
102. Lim K-H, Steinberg G: Preeclampsia. Emedicine article. Updated 31 August 2010 http://emedicine.medscape.com/article/1476919-overview
Footnotes