
Abstract
Congenital uterine anomalies are not uncommon. Many are asymptomatic and have been associated with normal and adverse reproductive outcomes. The interference of these anomalies with a patient's fertility is an interesting but still debatable issue, and the proper management of infertile women with many forms of these anomalies remains controversial. The current literature regarding the frequency and probable causes of infertility among women with congenital uterine anomalies is insufficient to allow any robust conclusions to be drawn. Diagnostic and selection bias, a lack of objective diagnostic criteria for the different anomaly types and heterogeneity of study designs have contributed to the conflicting results from different studies of the prevalence of these anomalies among the infertile and fertile populations. However, emerging evidence from recent literature suggests causal associations between these anomalies (particularly the septate uterus) and infertility, and demonstrates significant improvements in the fecundity of women with septate uteri and otherwise unexplained infertility after hysteroscopic metroplasty. This review provides a critical update of the state of knowledge regarding congenital uterine anomalies, our current understanding of their effect on fertility and discusses how they can be managed from the reproductive perspective.
Keywords
The uterus is responsible for many of the most crucial steps in the process of reproduction. Sperm migration, embryo implantation, fetal nourishment, development and growth, and finally, the process of labor and birth are all reliant on the existence of a structurally normal and functionally competent uterus. Congenital uterine anomalies may affect some or all of these uterine functions, precluding a successful pregnancy. These anomalies are not uncommon but many are asymptomatic and have been associated with both normal and adverse reproductive outcomes [1–6]. However, at the individual level, their effect on fertility and pregnancy outcomes can be devastating. Furthermore, the proper management of infertile women with these anomalies remains controversial. In addition, these anomalies may be isolated or may be part of a complex syndrome affecting other organs and can therefore have other implications; for example, Müllerian agenesis, renal anomalies and cervicothoracicsomite dysplasia (MURCS association) and vertebra/anus/cardiac/trachea/esophagus/radius/renal/limb (VATER/VACTERL) anomalies syndrome are associated with unicornuate uterus with noncommunicating horn [7,8]. In particular, the association of congenital uterine anomalies with those of the urinary tract is well recognized; up to 40% of patients with a unicornuate uterus and 80% of those with uterus didelphys were found to also have renal anomalies [9–13]. Furthermore, auditory defects were reported in over 22% of patients with Müllerian anomalies [14].
The interference of uterine anomalies with a patient's fertility is an interesting but still debatable issue. This review aims to provide an update of the state of knowledge regarding congenital uterine anomalies, our current understanding of their effect on fertility and we discuss how they can be managed from the reproductive perspective.
Normal & abnormal uterine development
Normal development
During week 6 of fetal life, the primitive gonads appear on the urogenital ridge, medial to the mesonephros [15,16], and the mesonephric (Wolffian) and paramesonephric (Müllerian) ducts develop. It has been suggested that Wolffian ducts act as a precursor/inducer for Müllerian formation [17] or as a guide in the downward growth of the Müllerian ducts [18]. By the seventh week, the
By the sixth week of fetal development, Müllerian ducts arise from longitudinal invaginations of the coelomic epithelium on the anterolateral surface of the urogenital ridges. The ducts develop bidirectionally – the proximal segments remain unfused to form the fallopian tubes while the distal segments progress caudomedially and join in the midline to form the uterovaginal primordium. By week 10, the latter contacts the dorsal wall of the urogenital sinus forming the Müllerian tubercle. Internal canalization of the Müllerian ducts then takes place. The fused caudal portions become divided by a septum, which then regresses in a caudocephalic direction (or bidirectionally [20–23]) and is eventually resorbed to form the uterus with its normally developed configuration and triangular-shaped endometrial cavity, and also form the cervix and upper vagina. In addition to inducing Müllerian development, the Wolffian ducts form the sinovaginal bulbs, which, together with the Müllerian tubercle, form the vaginal plate [24,25]. By the 18th week, the core of the vaginal plate degenerates, forming the lumen of the lower vagina, and this process is complete by week 20 [26,27].
Abnormal development
Congenital uterine anomalies may result from: failure of one or both Müllerian ducts to develop (e.g., agenesis, hypoplasia or unicornuate uterus without rudimentary horn); failure of one or both ducts to canalize (e.g., rudimentary uterus or a unicornuate uterus with rudimentary horn); failure of migration, or abnormal fusion, of the ducts (e.g., uterus didelphys or bicornuate uterus); and failure of resorption of the intervening septum (e.g., a septate uterus or arcuate uterus) [28–31]. The latter two groups constitute lateral fusion defects, which is the most common category of Müllerian defects [32]. In addition, vertical fusion defects may result from the abnormal fusion of Müllerian ducts with the urogenital sinus or from problems with vaginal canalization [33].
However, the most complex malformations are the mesonephric anomalies [17,34]. Wolffian ducts are a precursor/inducer of Müllerian development and are necessary for lower vaginal formation, and by providing the ureteral buds from their distal ends, they play a crucial role in renal development; hence, mesonephric anomalies are mostly associated with uterine malformations and also with the ipsilateral blind hemivagina and renal anomalies (mostly renal agenesis, but also cystic renal dysplasia, ectopic ureters and duplicate collecting systems [35–40]). The ipsilateral blind hemivagina may or may not communicate with the bicornuate/septate uterus (with or without communicating uteri) depending on the coexistence of cervical/cervicovaginal atresia [12,33] or may be associated with uterus unicornis with a rudimentary horn in cases of additional atresia or hypoplasia of the corresponding hemiuterus [41,42].
Classification of congenital uterine anomalies
The first classification was introduced by Strassmann in 1907 [43]. Since then, there have been several classifications based on:
The degree of failure of Müllerian development and fusion [44–47];
The flaws in vertical and lateral fusion leading to the occurrence of obstructive/nonobstructive and symmetrical/asymmetrical anomalies [48–50];
Using precise aspects such as the presence of communicating/noncommunicating bicornuate or septate uteri [51];
The embryologic origin of different elements of the genitourinary tract [34,52–54];
The anatomical structures of the female genital organs (e.g., vagina, cervix, uterus, adnexa-associated malformation [VCUAM] classification [55]).
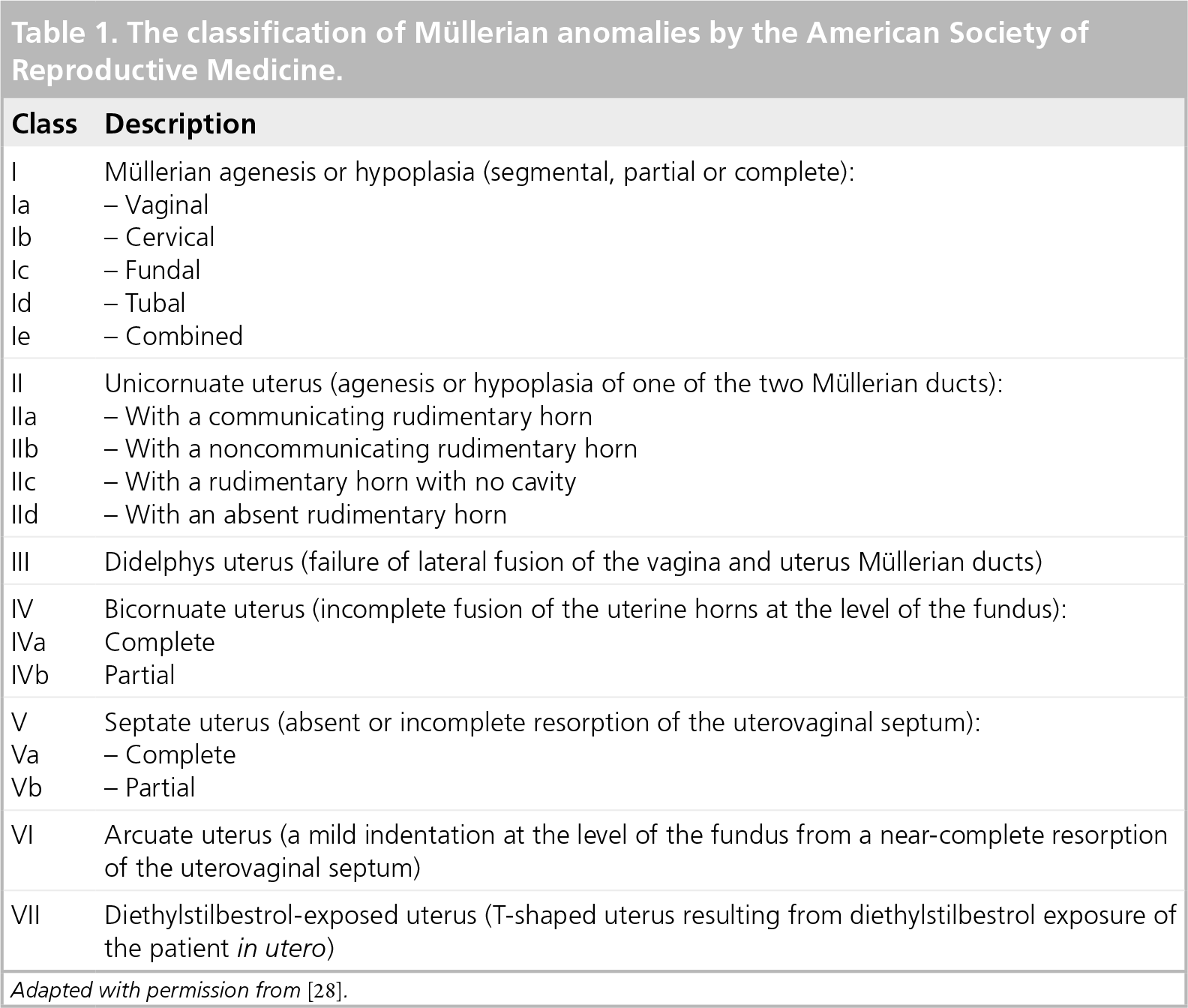
There is no universally accepted standard classification for congenital uterine anomalies [33]; however, the classification described by the American Society of Reproductive Medicine (ASRM; formerly known as the American Fertility Society [AFS]) [47] remains the most widely used. This classification is based on the extent of failure of Müllerian development and divides anomalies into groups with similar clinical manifestations, management requirements and prognosis (Table 1) [28]. However, this classification is not without shortcomings; for example, it does not include combined/complex anomalies (i.e., rudimentary uterus [52,56], cervical atresia [57], unilateral cervicovaginal atresia in a didelphys uterus [54] and utero-, cervico-and/or vaginal septation [58–60]), which are often incorrectly identified, inappropriately treated and sometimes inaccurately reported. Nor does this classification consider the accuracy of the methods used for detecting the anomaly [61–72]. Furthermore, it does not specify criteria for making the diagnosis of each anomaly or group of anomalies [73,74].
The classification of Müllerian anomalies by the American Society of Reproductive Medicine.
Troiano and McCarthy suggested that the AFS classification should function as a framework for describing anomalies, and that clinicians who are faced with complex/combined anomalies should describe them according to their component parts rather than categorizing them into the class that most approximates the dominant feature [75]. This approach was adopted by Acien
Clinical and embryological classification of the malformations of the female genital tract.
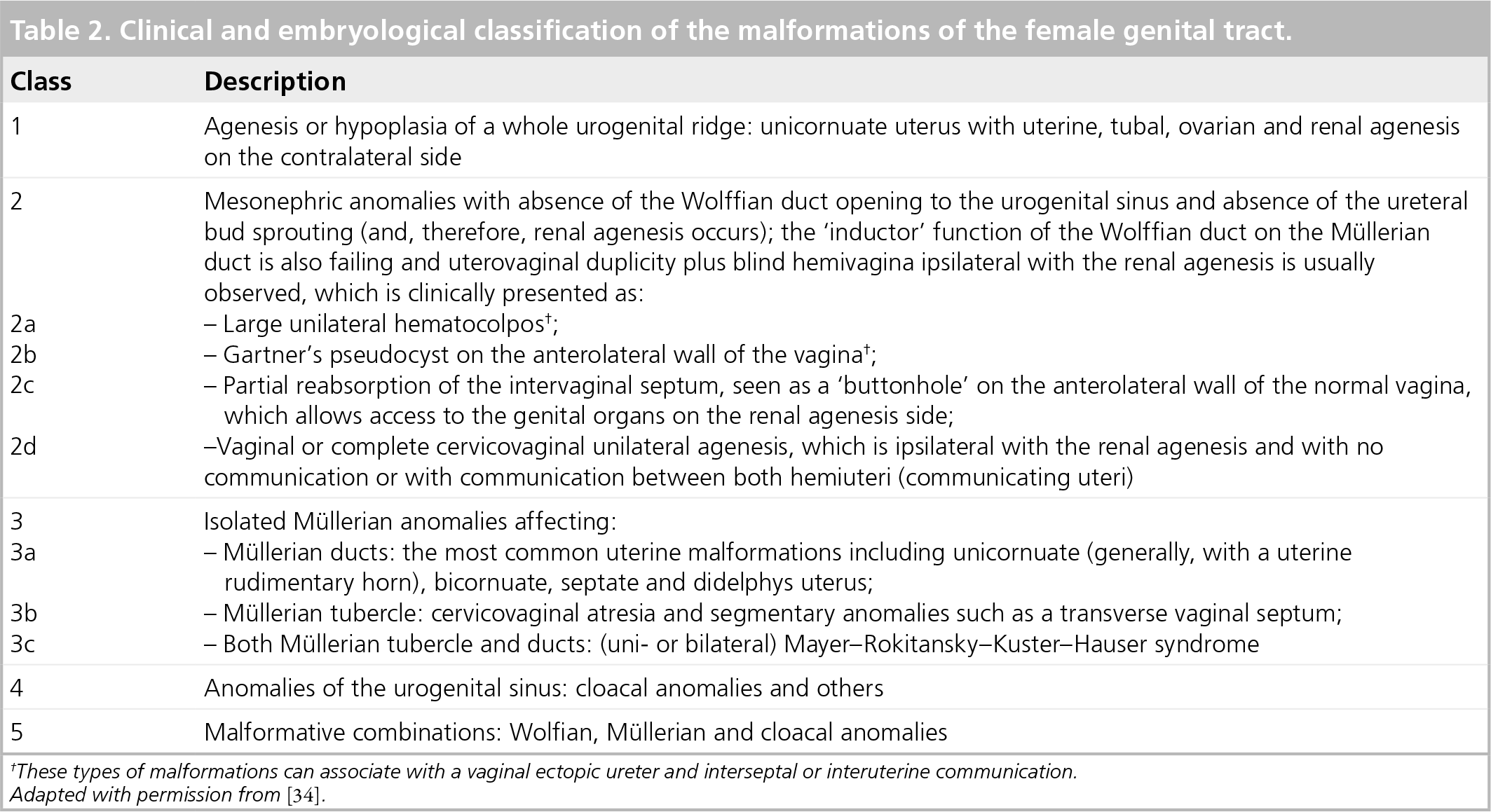
These types of malformations can associate with a vaginal ectopic ureter and interseptal or interuterine communication.
The VCUAM classification: descriptions of the individual malformations relative to the organ.

Etiological factors
The etiology of congenital uterine anomalies is poorly understood, and there are many theories involving genetic, environmental and pharmacologic factors. The role of genetic factors remains unclear. Normal karyotyping was found in 92% of women with Müllerian anomalies while 7.7% of these women had abnormal karyotypes [77]. Several genes have been implicated in the development of Wolffian and Müllerian ducts (e.g.,
Genetic patterns of inheritance have been described in the expression of Müllerian anomalies [81]. Hammoud
Effect of congenital uterine anomalies on fertility
The association between uterine anomalies and adverse pregnancy outcomes, particularly recurrent miscarriage, is well recognized [4,5,86–90]; however, the role of these anomalies in infertility, remains unclear [4,89–92]. To establish whether congenital uterine anomalies have an effect on fertility, the following need to be assessed:
Potential mechanisms whereby uterine anomalies may exert an effect on fertility – this is important for establishing the plausibility of such an effect;
Possible associations between uterine anomalies and infertility – such associations would be existent if the prevalence of these anomalies was found to be higher among the infertile than the fertile population, or if infertility was more likely among those who have these anomalies;
Probable underlying causation (cause–effect relationship) where the presence of uterine anomalies would lead to infertility; consequently, treating these anomalies would improve fertility prospects.
Potential mechanisms for an effect on fertility
Several theories have been postulated to explain the potential adverse effects of congenital uterine anomalies on fertility and reproductive outcome. The evidence to support these theories, particularly with the milder anomalies (e.g., arcuate and subseptate uteri) is deficient and lacking. This is compounded by the fact that Müllerian defects can permit an absolutely normal obstetric outcome [5]. The role of the mechanical factors in cases of severe congenital uterine anomalies (e.g., Müllerian agenesis and cervical atresia) is evident [88]; these factors may also play an important role in cases of less severe anomalies (e.g., bicornuate and septate uteri) that are likely to impact on uterine capacity and the arrangement of uterine musculature (and may consequently cause cervical incompetence). However, such effects are likely to cause adverse pregnancy outcomes rather than impairment of fertility [31,93].
Embryo implantation is affected by the morphology, thickness and vascularity of the endometrium, and by the shape and integrity of the uterine cavity; these factors are likely to be altered with congenital uterine anomalies [94]. Therefore, these anomalies can affect endometrial receptivity, resulting in implantation failure that manifests as early pregnancy loss or infertility [90]. Furthermore, congenital absence of the endometrium has been reported [95]. Uterine septa were found in 9.7% of women who had experienced preclinical miscarriage after IVF [96], and improved results with IVF after hysteroscopic metroplasty were reported [97]. This suggests that a uterine septum may be an important factor predisposing to implantation failure and early pregnancy wastage.
The uterine septum is thought to consist of fibroelastic tissue with inadequate vascularization and an altered relationship between the myometrial and endometrial vasculatures; hence the poor response of the endometrial mucosa covering the septum to estrogen, causing poor proliferation and estrogenic maturation [98,99]. As a result, implantation may be compromised or the decidual growth may be inadequate, causing infertility or early pregnancy loss. It has been suggested that removing the septum may eliminate an unsuitable site for implantation, improve endometrial function, expand uterine capacity and dramatically enhance the reproductive outcome in selected patients [89]. Conversely, Dabirashrafi
Several studies have suggested that the effects on fertility caused by congenital uterine anomalies could be mediated through other infertility factors. Sorensen found that infertility patients with mild Müllerian anomalies were three-times more likely than those with normal uterine cavities to also have oligo/amenorrhea (58.6 vs 19.6%, respectively; p < 0.01), which, in these cases, was almost three-times more likely to be idiopathic (82.4 vs 30%; p < 0.01) [101]. It has been suggested that a defect in steroid receptor proteins in the congenitally deformed uterus may be responsible for these patients' eugonadotropic oligo/amenorrhea. Ugur
Possible associations with infertility
The exact prevalence of congenital uterine anomalies is uncertain [88–90]. Accurate assessment and comparison of the prevalence of these anomalies among the infertile and fertile populations in order to detect associations between these anomalies and infertility (if any) is compounded by several sources of bias. The use of different techniques with variable diagnostic accuracies, the lack of universally accepted objective diagnostic criteria for each anomaly, the inconsistency in interpreting the classification of uterine anomalies and the heterogeneity of the populations examined by various studies have all contributed to the difficulty in determining the true prevalence of congenital uterine anomalies [2–4,69,74,75,89,105,106].
Diagnostic accuracy
Saravelos
Classification of the investigative procedures used for assessing congenital uterine anomalies according to diagnostic accuracy.
Investigations capable of accurately identifying congenital uterine anomalies and classifying them into appropriate subtypes (accuracy >90%):
– Hysteroscopy and laparoscopy
– Hysterosonography (sensitivity: 93%; specificity: 99%; accuracy: 97%)
– 3D-USS (sensitivity: 100%; specificity: 100%; accuracy: 100%)
Investigations capable of accurately identifying congenital uterine anomalies (accuracy >90%) without being able to classify them into appropriate subtypes:
– Hysteroscopy alone
Investigations capable of identifying congenital uterine anomalies with an accuracy of <90%:
– Hysterosalpingography (sensitivity: 78%; specificity: 90%; accuracy: 86%)
– 2D-USS (sensitivity: 56%; specificity: 99%; accuracy: 84%)
Investigations of which the accuracy in diagnosing congenital uterine anomalies is uncertain:
– MRI
– Physical examination during pregnancy or delivery
Hysterosalpingography is a useful screening tool for providing information regarding the uterine cavity [28] and for diagnosing malformations with more aggressive morphological expressions [67]. However, since it does not evaluate the external uterine contour, HSG cannot reliably differentiate between septate and bicornuate uteri [70,75,89]. 2D-USS allows quantification of the observations but has low sensitivity (only identifies approximately half of the uterine anomalies), although it also has a low false-positive rate and its diagnosis is likely to be correct [75,118]. However, there are no universally accepted USS diagnostic criteria for congenital uterine anomalies. Hysterosonography has the advantage of improving the delineation of the internal uterine contour [119] and appears to be accurate, not only in diagnosing, but also in categorizing uterine anomalies into appropriate groups [112,120,121]. 3D-USS has a very high accuracy rate in diagnosing and classifying uterine anomalies [114], with high reproducibility (interobserver variability of only 1% [68]); therefore, introducing appropriate universally accepted diagnostic criteria and a classification of uterine anomalies using 3D-USS could improve the homogeneity of diagnoses. MRI offers a sensitive noninvasive approach of assessing the internal and external uterine contours [62,122,123] and could therefore replace invasive procedures such as laparoscopy for the diagnosis of a ‘double uterus’ [124]. However, owing to the lack of evidence, more studies are required to confirm its diagnostic accuracy.
Hysteroscopy is accurate in identifying congenital uterine anomalies and is often used to establish a definitive diagnosis following an abnormal HSG finding [28,67,88]. However, it does not allow for evaluation of the external uterine contour and is often inadequate in differentiating between different anomaly types; diagnostic laparoscopy is required for the correct differentiation between bicornuate and septate uteri, and this combination (hysteroscopy/laparoscopy) is considered as the gold-standard diagnostic investigative method for evaluating congenital uterine anomalies [4,28,88,90,119]. Hysteroscopy combined with laparoscopy also offers the advantage of concurrent treatment (e.g., resection of uterine septum). However, since there are no strict diagnostic criteria, this exclusively relies on the subjective impression of the clinician [74].
Diagnostic criteria
There are no universally accepted diagnostic criteria for the different types of congenital uterine anomalies. This and the low accuracy of the techniques used for making diagnoses in many of the studies has resulted in wide discrepancies in the reported prevalence of these anomalies; for example, using HSG angles of less than 75° and more than 105° between the uterine horns has been suggested to diagnose the septate and bicornuate uteri, respectively [28,75]. However, the majority of angles of divergence between the horns fall within this range and considerable overlap between these anomalies are noted [61].
Similarly, some authors [75,88,122] consider the uterus to be septate rather than bicornuate if the fundal indentation of the external contour (identified by USS) is greater than 5 mm above the interostial line, while others [28,74,114] have used a cut-off of 10 mm to differentiate between the two anomalies. A threshold of 10 mm of fundal indentation has also been used in laparoscopy [75]. Furthermore, an angle of less than 60° between the two indenting medial margins of the fundus has been used to distinguish between septate and bicornuate uteri. Using these criteria, 92% sensitivity and 100% specificity for diagnosing bicornuate uteri have been reported [113], yet the value of these criteria remains unclear. In addition, measurement of the serosal–endometrial thickness along the uterine fundal border in longitudinal sections has been used as a criterion to aid diagnosis [28]. However, there is no evidence in the literature of such criteria that describe the subseptate uterus and differentiate it from the arcuate deformity. Using MRI, the criteria used to distinguish bicornuate from septate uteri are often similar to those used for USS: a 10 mm threshold of fundal indentation, an intracornual distance of greater than 4 cm or an angle greater than 60° between the two indenting medial margins of the fundus [28].
Using office hysteroscopy, without the use of anesthesia, Bettocchi
Prevalence among the general (fertile) populations
In addition to diagnostic bias, the difficulty in determining the true prevalence of these anomalies among the fertile population may relate to selection bias. Various studies have used different population samples to assess the prevalence of uterine anomalies (e.g., women undergoing sterilization [5,6,125] or being investigated for nonobstetric reasons [118], such as pelvic pain, abnormal uterine bleeding [126] or suspected fibroids [74]). These samples may not be representative of the fertile population, and such bias may result in overestimation of the prevalence of these anomalies among the fertile population.
The effect of these biases is likely to have been reflected in the wide discrepancy between the reported figures for the prevalence of congenital uterine anomalies from different studies (from < 0.5% [105,118] to almost, or over, 10% [3,74,126,127], with a number of studies reporting figures of approximately 2–4% [5,6,30,128] and others of approximately 5–6% [125,129–131]); the lower figures were reported by studies that relied on 2D-USS or HSG [5,6,30,118,128], while the higher figures were reported by those that used 3D-USS, hysterosonography or hysteroscopy [74,125,126,130,131], reflecting the biasing effect of using different diagnostic methodologies among studies. Similarly, Nahum estimated the prevalence of congenital uterine anomalies to be 0.5% among the general and 0.17% among the fertile populations (an extremely low prevalence, which could be related to the inclusion of studies that have relied on physical examination after delivery for assessing the morphology of the uterine cavity) [105], while Grimbizis
Similarly, diagnostic bias is likely to have impacted on the reported prevalence of the different uterine anomalies. This could explain the wide variation in the reported prevalence between studies, particularly of the milder forms of anomaly, such as arcuate uterus, for which estimates range from single figures [6,30,118,128] to over two-thirds of the reported anomalies [74,126,131]. This also explains the difficulty in differentiating between the septate and bicornuate uteri in cases of a ‘double uterus’ appearance observed in earlier studies, which was then overcome by adding laparoscopy to assess the outer uterine contour or by using 3D-USS [74,126,131]. Nahum reported the following distribution of prevalence: 7% for arcuate, 34% for septate, 39% for bicornuate, 11% for didelphic, 5% for unicornuate, and 4% for hypoplastic/aplastic uteri [105]. By contrast, Grimbizis
Prevalence among the infertile population
Similarly, the exact prevalence of congenital uterine anomalies among the infertile population is unknown. Diagnostic bias is likely to have occurred owing to the use of different investigative methods. In addition, selection bias may have impacted on the quoted prevalence reported by different studies owing to the use of different infertility definitions and/or different inclusion criteria (e.g., duration of infertility [5]; primary/secondary infertility [108,110,132]; any cause/tubal/unexplained infertility [133,134]; women undergoing infertility investigation/IVF [64,115,126]; and/or women with oligomenorrohea/polycystic ovaries [101,102]). However, selection and diagnostic biases
Nahum estimated the prevalence of congenital uterine anomalies among the infertile population to be 3.5% (which is over 20-fold higher than the author's estimated prevalence among the fertile population [0.17%]) [105]. Grimbizis
Nahum found significant differences in the distributions of different anomaly types between the fertile and infertile populations [105]. Compared with the fertile group, there were higher proportions of aplastic/hypoplastic (15 vs 3%) and unicornuate (11 vs 4%) uteri among the infertile group, while the bicornuate (25 vs 41%) and didelphic (8 vs 12%) uteri were proportionately under-represented and the septate and arcuate uteri had similar distributions among the two groups. These distributions are likely to have been influenced by selection and/or diagnostic biases. Grimbizis
Comparison of the prevalence among the fertile & infertile populations
To uphold such a comparison and to consequently establish whether congenital uterine anomalies have an effect on fertility, a number of principals need to be set:
To demonstrate the effect (if existent) of uterine anomalies on fertility; their prevalence among the fertile, rather than general, population is more relevant;
The common causes of infertility should be ruled out in the infertile population, or otherwise clearly stated, since these coincidental factors may confound the observed prevalence of uterine anomalies among the infertile population;
The arcuate uterus is considered by many as a ‘normal variant’, while others consider this to have an adverse effect on reproductive outcome; therefore, for the purpose of assessing an association with infertility, the prevalence of uterine anomalies among the different populations should be estimated including and excluding the arcuate uterus;
Different types of uterine anomalies may have different associations with infertility and studying the prevalence of specific anomaly types is more important and more clinically relevant than studying the overall prevalence;
The effect of diagnostic bias on the results of the reporting studies on the prevalence of uterine anomalies among different populations should be considered.
First, to assess the possible association of a variable with infertility, it is best to carry out a comparison between the prevalence of that variable among fertile women who have had a pregnancy and the prevalence among infertile women, regardless of whether they have or have not sought medical advice. For this reason, using a group of women with nonobstetric causes for investigation (e.g., abnormal uterine bleeding) as the comparison group for the purpose of assessing the association of uterine anomalies with infertility would appear to be inappropriate (also in view of potential associations of such causes with uterine anomalies and/or infertility). Furthermore, studies of the prevalence of uterine anomalies among the fertile population that include women following giving birth or those attending hospitals for sterilization, exclude those whose pregnancies have all ended in miscarriages. Yet from the purpose of assessing the exclusive association between uterine anomalies and infertility, this exclusion seems to be appropriate given the well-recognized association between these anomalies and recurrent miscarriage.
Second, the infertility of a proportion of women in the group used for estimating the prevalence of uterine anomalies among the infertile population may be related to one or more of the common infertility causes. The occurrence of these causes in those cases may be totally incidental or there may be an association between these causes and uterine anomalies (further discussed in the section titled ‘Potential mechanisms for an effect on fertility’). Therefore, for the purpose of assessing an exclusive effect (if any) of uterine anomalies on fertility, common infertility causes need to be ruled out in the group used to estimate their prevalence among the infertile population, otherwise these causes should be sought and clearly stated, which may help to establish associations between these infertility causes and uterine anomalies.
Third, the arcuate uterus has the same embryological origin and requires the same therapy as the subseptate uterus but, since it appears extremely unified and seems to behave benignly, it was considered in the AFS classification as a separate entity. For those reasons, the arcuate uterus is considered, by many, as a normal variant [105,135]. Raga
Fourth, in addition to the variation in the overall prevalence of uterine anomalies between different populations, as mentioned previously, several studies found that the distribution of different anomaly types (and, consequently, their relative frequencies) also varies between populations. Furthermore, other studies suggested that different uterine anomaly types may be associated with different patterns of adverse reproductive outcome. (Woelfer
Fifth, the effect of diagnostic bias on the reporting studies regarding the prevalence of congenital uterine anomalies among the different populations has been discussed previously in this article.
None of the earlier published reviews regarding the prevalence of congenital uterine anomalies among fertile and infertile populations have considered all of these principals. This may explain the conflicting results and the continuing controversy as to the effect of these anomalies on fertility. Acien recorded hardly any difference between the prevalence of uterine anomalies among the general population and infertile women [3]. Nevertheless, this review has limitations and is likely to have been influenced by diagnostic bias in view of the investigative methods used. Furthermore, in almost half of the reported cases that were included in the review, the diagnostic methods used were not clearly stated [136,137]. In addition, the lack of a standard classification system and the fact that the populations studied may not be representative of the fertile population are further biasing factors in that review. Nahum found a significant difference between the prevalence of uterine anomalies among fertile and infertile populations, suggesting an association with infertility [105]. Studies in this review included subjects that seem to be representative of these populations, but the major shortcoming is related to diagnostic bias resulting from the inclusion of studies that relied on less accurate methods for detecting/classifying uterine anomalies (explaining the very low prevalence of uterine anomalies among the fertile population reported in that review). Grimbizis
Saravelos
Infertility among women with congenitally malformed uteri
The frequency and likely causes of infertility, particularly the incidence of unexplained infertility, among women with congenital uterine anomalies relative to women with normal uteri could provide information relating to the impact of these anomalies on fertility. However, there is an evident lack of data regarding the fertility of women with congenital uterine anomalies. Acien found that 19.3% of women with uterine anomalies were infertile – an incidence comparable to that of a control group and is close to the reported approximate 15% incidence among the general population [86]. The author found that the incidence of unexplained infertility among infertile women with uterine anomalies (29.4%) was comparable to that among the infertile population as a whole [138–141]. These data do not support the concept of uterine anomalies as an infertility factor. Conversely, Grimbizis
Several studies of assisted conception among infertile women with and without uterine anomalies demonstrated similar implantation and pregnancy rates in the two populations. Marcus
Probable underlying causation of infertility
If there were to be a cause–effect relationship between congenital uterine anomalies and infertility, then correction of these anomalies would be associated with significant improvements in subsequent fertility prospects. There is strong evidence to support the effectiveness of hysteroscopic metroplasty in cases of uterine anomalies with earlier poor reproductive outcome, with decreases in miscarriage ranging from 88 to 14%, and 80% of these will have a term livebirth after metroplasty compared with 3% before metroplasty [4,88–90]. However, for cases of primary infertility, metroplasty is a controversial and much debated issue [4,147]. Owing to the lack of robust evidence based on randomized trials among infertile women with uterine anomalies to compare those who have had metroplasty versus those with no treatment, the proper management of these women remains contentious [90]. Since removal of the septum may potentially prevent miscarriage and preterm birth, if these women are to conceive, it has been argued that metroplasty should be considered in these cases [88,137,148,149]. However, since many women with septate uteri can still have reasonable pregnancy outcomes and since there is no established causal relationship between the septate uterus and infertility, the controversy remains as to whether infertile women who have a septate uterus should undergo metroplasty [150,151].
Several relatively small studies suggest that women with septate uteri and primary infertility may benefit from metroplasty [31,103,104,152–158], although the improvement observed in pregnancy and term live-birth rates is relatively modest (29.5%) [142]. These rates are significantly higher in women after metroplasty who previously suffered recurrent pregnancy loss, which highlights the difference in fertility between the two populations [88,103,142]. Daly
However, heterogeneity, small sample sizes, retrospective design, self-control design and the absence of control groups makes the interpretation of results from these studies difficult. In addition, results of assisted conception studies were inconsistent. Marcus
Furthermore, emerging evidence from recent studies demonstrates significant improvements in the fecundity of women with a septate uterus and otherwise unexplained infertility after hysteroscopic metroplasty. In a prospective self-control study of women with septate uteri and unexplained infertility, Pabuccu and Gomel reported a pregnancy rate of 41% after metroplasty [142]. The authors suggested that such a percentage supports the idea of the existence of a ‘subtle factor’ that is able to impair implantation in these patients. In addition, in a prospective controlled study of women with a septate uterus and otherwise unexplained infertility who underwent hysteroscopic metroplasty, Mollo
Conclusion
The effect of congenital uterine anomalies on fertility has been a much debated subject. Diagnostic and selection bias, a lack of objective diagnostic criteria and an appropriate classification system of different anomaly types, and heterogeneity of study design have contributed to the conflicting results from different studies regarding the prevalence of these anomalies among the infertile and fertile populations. When the accuracy of the diagnostic procedures used was taken into account, it appeared that the prevalence of the septate uterus was over three-times higher (and those of unicornuate and hypoplastic uteri were also higher) among infertile women than in the general population, suggesting associations with infertility. Furthermore, recent evidence reveals significant improvements in pregnancy and livebirth rates and a significantly higher probability of conception and cycle fecundity among women with septate uteri and otherwise unexplained infertility, who underwent hysteroscopic metroplasty relative to women with unexplained infertility and also relative to those with an untreated septate uterus. Despite the fact that this is not based on randomized trials comparing treated and untreated women with septate uteri, this evidence is the best evidence to date for a causal association between the septate uterus and infertility. It may be that uterine anomalies are more closely related to recurrent miscarriage then infertility. However, based on current evidence, infertile women who have no apparent cause for infertility should be offered an investigative procedure (e.g., 3D-USS, hysterosonography or hysteroscopy) and those who are found to have a congenitally malformed uterus (particularly septate uterus) should be counseled regarding the potential association with infertility and should be offered hysteroscopic metroplasty (particularly in women with prolonged infertility, women older than 35 years of age and those who are planning to pursue assisted conception).
Future perspective
We believe that a diagnostic method for detecting congenital uterine anomalies (e.g., 3D-USS or hysterosonography) will be a standard part of the infertility work-up. Infertile women who are found to have a uterine septum will be routinely offered hysteroscopic metroplasty, which will be most often carried out as an office procedure.
Executive summary
The interference of congenital uterine anomalies with fertility is still a debatable issue and the proper management of infertile women with these anomalies remains controversial.
The Wolffian ducts may act as a precursor/inducer for Müllerian duct formation or as a guide in the downward growth of the Müllerian ducts.
In female embryos, absence of the
Müllerian anomalies may result from the failure or malformation of some or all of a series of events including: Müllerian duct formation, elongation, fusion, canalization and septal resorption.
Lateral fusion defects are the most common category of Müllerian anomalies, but the most complex malformations tend to be the mesonephric anomalies.
There is no universally accepted standard classification for anomalies of the female reproductive tract, but the American Fertility Society (AFS) classification remains the most widely used.
The AFS classification system should function as a framework for the description of anomalies, rather than as an exhaustive list of all possible anomaly types.
The etiology of congenital uterine anomalies is poorly understood and there are many theories involving genetic, environmental and pharmacologic factors. The pattern of familial clustering of uterine anomalies suggests a polygenetic or multifactorial mechanism.
Several theories have been postulated, but the evidence in many cases, particularly for the milder forms of uterine anomalies, is deficient and lacking.
Mechanical factors are likely to have an important role in the effect of uterine anomalies on fertility, particularly in cases of severe congenital uterine anomalies.
The endometrial morphology, thickness and vascularity are likely to be altered in cases of congenital uterine anomalies.
Congenital uterine anomalies can affect endometrial receptivity, resulting in implantation failure that manifests as recurrent early pregnancy loss or infertility.
The effect of congenital uterine anomalies on fertility may be mediated through other infertility factors.
The true and exact prevalence of congenital uterine anomalies is uncertain, and there are wide discrepancies between the reported figures from different studies.
Difficulties in determining the true prevalence of congenital uterine anomalies relate to the variation in diagnostic accuracy of the techniques used, the lack of objective diagnostic criteria, the inconsistency in interpreting the classification system, the asymptomatic nature of many anomalies, the selective sampling in many studies and the heterogeneity of the populations studied.
Hysteroscopy combined with laparoscopy, 3D-ultrasound and hysterosonography are highly accurate in diagnosing and classifying uterine anomalies; if 2D-ultrasound is used in conjunction with hysterosalpingography, it can serve as a valuable screening tool. The potential role of MRI requires further evaluation.
The current literature on the frequency and probable causes of infertility among women with congenital uterine anomalies is too limited to draw any robust conclusions.
The existent prevalence literature provides conflicting results and conclusions. For accurate assessment and comparison of the prevalence of uterine anomalies among the infertile and fertile populations, a number of principals relating to the sampling of populations, study design and methodology need to be considered.
Evidence form the recent literature indicates that the prevalence of the septate uterus is markedly higher among the infertile population relative to the general population, suggesting an association with infertility.
There is an apparent lack of robust evidence, based on trials among infertile women with uterine anomalies, to compare fertility prospects in women after undergoing metroplasty versus those with no treatment, and the proper management of these women remains contentious.
Emerging evidence from more recent prospective controlled studies demonstrates significant improvements in the fecundity of women with a septate uterus and otherwise unexplained infertility after hysteroscopic metroplasty relative to women with unexplained infertility and a normal uterus, suggesting a causal association between the septate uterus and infertility.
Footnotes