
Abstract
Several variations in fallopian tube anatomy may be noted during the evaluation of infertility. Some anatomical variants such as accessory tubal ostia are rare. A 31-year-old woman presented to our center with a 2-year history of primary infertility. Given her history of dysmenorrhea, a diagnostic laparoscopy was performed. Laparoscopy revealed a left utero-sacral endometriosis implant, which was resected. Although the left fallopian tube was normal, the right fallopian tube was noted to have two prongs with individual ostia. Tubal cannulation confirmed two separate ostia, with chromotubation showing free flow of dye through separate fimbrial ostia of the right fallopian tube. The current case highlights that accessory tubal ostia are rare müllerian duct anomalies seen during laparoscopy and can be associated with endometriois or primary infertility.
Keywords
Introduction
Disease of the fallopian tube accounts for about 25%–35% of all female infertility cases.1,2 Several variations in fallopian tube anatomy may be noted during the evaluation of infertility either via pelvic ultrasonography (US), hysterosalpingography (HSG), or laparoscopy. 3 Some anatomical variants such as phimoses, accessory tubes, sacculations, and fimbrial agglutinations are noted frequently, 3 while others such as accessory tubal ostia are encountered rarely. 4 Accessory tubal ostia are considered natural but rare fallopian tube variants that occur when ectopic tubal fimbria are noted at a distance from the normal fimbriated end.5,6 Previous studies have reported accessory tubal ostia, at least co-incidentally, in patients undergoing treatment for infertility.6–8 However, the association between accessory tubal ostia and infertility remains contentious as the aforementioned studies are from over 25 years ago. Thus, given the rarity of accessory tubal ostia, particularly in association with infertility, we report the case of a 31-year-old nulligravid woman found to have an accessory tubal ostium, during the laparoscopic evaluation of severe dysmenorrhea and primary infertility.
Presentation of the case
Patient details
A 31-year-old woman presented to our center with a 2-year history of primary infertility. Although her menstrual cycles were regular, she experienced moderate-to-severe dysmenorrhea. She did not experience dysmenorrhea. Her medical and surgical history was unremarkable. She had no history of sexually transmitted infections. Her partner was 35-year-old gentleman with no proven fertility.
Initial assessment
The patient’s initial work-up revealed normal levels of follicle-stimulating hormone, luteinizing hormone, anti-mullerian hormone, thyroid-stimulating hormone, and prolactin. Her HSG showed normal fill and spill of radiographic dye through both fallopian tubes. A transvaginal pelvic US revealed normal uterine contour and normal ovaries with an antral follicle count of approximately 24. Her partner’s semen analysis was also within normal limits.
Treatment
Given her history of dysmenorrhea, a diagnostic laparoscopy was performed. Although the pelvis was devoid of any adhesions, an endometriosis implant was noted on the left utero-sacral ligament, which was resected using monopolar scissors (Figure 1). The left fallopian tube appeared normal; however, the right fallopian tube (Figure 2) was noted to have two prongs (one main/primary fallopian tube ostium and a second accessory fallopian tube ostium). Laparoscopic cannulation confirmed two separate ostia, with chromotubation showing free flow of dye through separate fimbrial ostia of the right fallopian tube (Figure 3). Histopathology of the left utero-sacral implant was consistent with endometriosis.

Circle highlights the resection site of the left utero-sacral endometriosis implant.

Laparoscopic view of the right fallopian tube with two separate fimbrial openings, that is, a primary and accessory ostium.
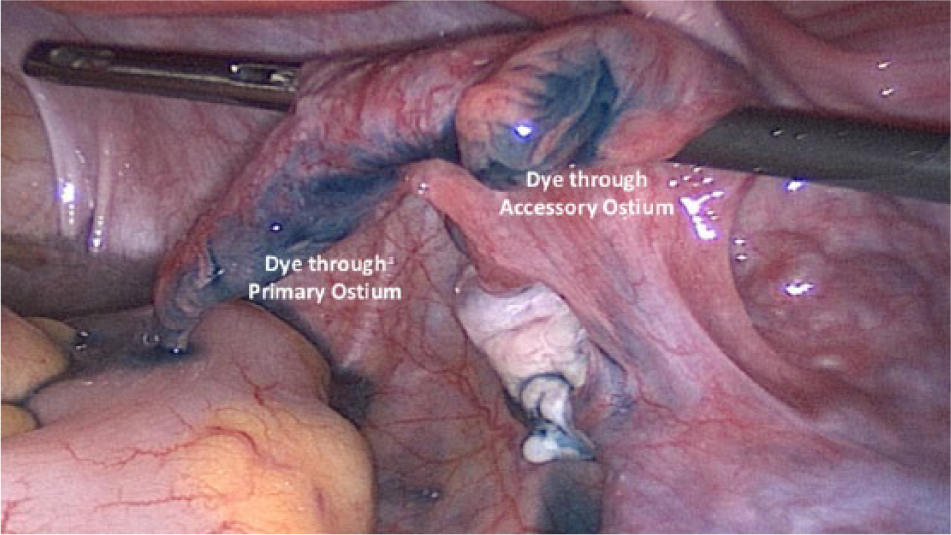
Chromotubation revealing normal flow of dye through the primary and accessory ostium of the right fallopian tube.
Outcome and implications
Following laparoscopy, the patient underwent four intrauterine insemination (IUI) cycles: two with clomiphene citrate and two during natural cycles. However, all IUI cycles were unsuccessful. The patient is currently undergoing treatment with in vitro fertilization.
Discussion
Accessory tubal ostia are rare müllerian duct anomalies, with an estimated incidence of 1.9%. 5 They are characterized by two separate fimbrial openings, that is, a greater (primary) and lesser (accessory) ostium,1,5 and are thought to result from the bifurcation of the distal ends of the müllerian ducts.2,6 HSG may not provide informative clues about accessory ostia, thus necessitating laparoscopy, particularly in the presence of dysmenorrhea or primary infertility. Accessory tubal ostia are divided into two subtypes depending on the distance between the primary and accessory ostia seen during laparoscopy. Those occurring <1 and ⩾1 cm from the primary ostia are called terminal and ampullary accessory ostia, respectively. 5 Accessory tubal ostia are frequently associated with endometriosis. 5 In one study, 90.5% (19/21) patients with accessory ostia were noted to have stage I–II endometriosis. 5 In another retrospective study, the incidence of accessory tubal ostia was found to be higher among infertile women (10%) than fertile controls (0%). 3
Possible complications associated with this anomaly include ectopic pregnancy, pyosalpinx, as well as infertility.3–6 Its involvement in the pathogenesis of infertility remains unclear although one possible mechanism involves the escape of the ovulated oocyte from the fallopian tube through the accessory ostium.3,5 The additional ostium may also perturb normal ciliary function and transport of fluid through the fallopian tube, thereby impacting the early steps of fertilization. Given its association with endometriosis, it also likely that endometriosis-related pro-inflammatory mediators also impede fertility by causing distal tubal agglutination or phimosis.3,5 Such derangement in fallopian tube function may occur even in early stage endometriosis. 5
Surgical treatment of accessory tubal ostia can be achieved through the laparoscopic or abdominal approach. Ampullary accessory ostia can be treated with a monofilament purse-string suture at the base of the accessory ostium followed by resection or electrocoagulation of ostial stump. 5 In contrast, terminal accessory ostia can be treated with an incision made from the fimbria to the accessory ostium, with a mattress suture of the fimbria. 5 Good fertility outcomes have been reported after surgical treatment of accessory tubal ostia. In a study of 21 infertile women with accessory ostia, Cohen 7 reported a live birth rate of 47% with natural conception after tubal microsurgery. Using a laparoscopic approach in 18 patients with accessory ostium, Zheng et al. reported a clinical pregnancy rate of 66.7% with natural conception and IUI. While did offer our patient the options of laparoscopic tubal surgery following her unsuccessful cycles, she opted for in vitro fertilization.
Conclusion
Previous reports in the medical literature have described accessory tubal ostia as incidental anatomical variants during the work-up for infertility or in conjunction with endometriosis. Although its association with primary infertility remains contentious, we posit that the anatomic and functional aberrations of the fallopian tube as the accessory ostium may contribute to the pathogenesis of primary infertility. Patients with accessory tubal ostia may have normal HSG findings, thereby necessitating laparoscopy in those with dysmenorrhea or primary infertility. Surgical treatment of accessory tubal ostia can be achieved through the laparoscopic or abdominal approach although many patients may opt for assisted reproductive techniques to achieve a pregnancy.
Executive summary
Introduction
Several variations in fallopian tube anatomy may be noted during the evaluation of infertility.
Some anatomical variants such as accessory tubal ostia are rare.
Presentation of the case
Accessory tubal ostia may frequently present in conjunction with endometriosis.
Discussion
Hysterosalpingography may not provide informative clues about accessory ostia, thus necessitating laparoscopy, particularly in the presence of dysmenorrhea or primary infertility.
Surgical treatment of accessory tubal ostia can be achieved through the laparoscopic or abdominal approach although many patients may opt for assisted reproductive techniques to achieve a pregnancy.
Conclusion
Accessory tubal ostia are rare müllerian duct anomalies seen during laparoscopy, which can be associated with endometriosis and primary infertility.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional review board
Institutional review board approval was not required for this report. Verbal patient consent was obtained for the publication of this case.