
Abstract
Sexual function in female diabetic patients is much less investigated than in males. Empirical studies do not show uniform results, but it appears that diabetic women experience more frequent sexual dysfunction in general than age-matched healthy controls, independent of the sociocultural environment. The most frequently cited dysfunctions are desire and arousal disorders, such as lubrication difficulties, while orgasmic capacity appears to be less affected. Direct pathophysiological effects on lubrication are proven, but the impact on mental arousal is unclear. The role of diabetic complications is controversial. The comorbidity with depression plays a major role. Individual coping with the disease and the quality of the relationship are also contributing factors. Patients should be encouraged to talk about their sexual problems, as both biomedical and psychosocial factors have to be explored. Therapeutic interventions include basic counseling, biomedical treatment of atrophy and lubrication difficulties, as well as treatment of comorbidities and/or sex therapy.
Keywords
In Western societies, diabetes mellitus has a high prevalence. Worldwide it is estimated that 171 million people suffer from diabetes and it is projected that by 2013 there will be 366 million people affected [1]. For the moment there is no cure, thus the goals in general are twofold, namely minimizing long-term complications and maximizing or optimizing the wellbeing and quality of life of the affected individuals. Sexual function or dysfunction and sexual satisfaction are part of the psychosocial wellbeing. For a long time is has been recognized that men are at risk for developing impaired sexual function and research has mainly focused on sexual problems in diabetic men. The impact of diabetes on female sexual function has been investigated much less. In recent years, a few epidemiological studies have, however, demonstrated that there is an increase of female sexual dysfunction (FSD) in diabetic women compared with controls, although the type of dysfunction and the possible causes are controversial.
This review attempts to answer the following questions: do diabetic women suffer more frequently from FSD and/or do diabetic women suffer from specific patterns of sexual dysfunction? What causes FSD in diabetic patients? And finally, how should we diagnose and treat FSD in patients with diabetes mellitus?
Methodology
Literature in Pubmed from the last 10 years was searched for using the search terms ‘diabetes’, ‘female sexual dysfunction’, ‘FSD’ and ‘risk factors of FSD’. Cases treated at the Division of Psychosomatic of Obstetrics and Gynaecology and Sexuality at the University Hospital, Basel, Switzerland, were reviewed.
Results
Two major methodological problems had to be taken into account. First, prevalence studies looking for frequencies of sexual dysfunction and comparing it to controls have several drawbacks, which make evaluation difficult. Diabetes mellitus is not a single disease; it includes both Type 1 and Type 2 diabetes. Age, length of the disease, complications, treatment modalities, as well as the life phase, such as premenopause and perimenopause, may have an important impact. Some of the studies control for these variables, others do not. Owing to the complexity of human sexuality, it is methodologically very difficult to control for all intervening variables.
Second, explorative correlational studies trying to determine the causes of sexual dysfunction encounter other difficulties, for example differentiating the impact of physiological changes versus psychological changes, looking for the impact of diabetes-specific health problems versus the general problems of chronic disease, and finally, looking for or differentiating between diabetes-related factors and comorbidities.
Do diabetic women suffer more frequently from female sexual dysfunction?
In some large epidemiological studies, diabetes mellitus is cited as a risk factor for sexual dysfunction in male and female patients [2–4].
An international expert committee concluded in their publication that common risk factor categories associated with sexual dysfunction exist for men and women, including: individual general health status, diabetes mellitus, cardiovascular disease, other genitourinary disease, psychiatric/psychological disorders, other chronic diseases and sociodemographic conditions [5].
Searching for risk factors for FSD in a Brazilian community sample, the authors found that women with diabetes mellitus had a higher probability of developing low sexual desire and orgasmic difficulties [6].
In a review published in 1998 summarizing 15 studies, the reviewers concluded after critical analysis of the data that diabetes in women might have some negative influence on sexual desire, that problems with vaginal lubrication seemed to be increased two-times and that there was no major influence on orgasm. They pointed out that the results were inconsistent and partially contradictory [7].
It is notable that some authors, such as Schiel, found a significant difference between women with Type 1 diabetes and those with Type 2 diabetes [8]. In Type 1 diabetes the prevalence of sexual disorders was 18%, while in Type 2 patients it was 42%.
In a more recent study looking at 50 women with Type 1 diabetes and 47 healthy controls, the authors found that Type 1 diabetic women had decreased sexual function and increased sexual distress compared with control subjects during the luteal but not the follicular phase of the menstrual cycle [9].
Women with Type 2 diabetes were assessed by Erol and coworkers [10]. A total of 72 young diabetic women with a minimum age of 37.8 years and no other systemic diseases were age-matched to 60 healthy controls. Female sexual functioning index (FSFI) was used in this study. Lack of libido was the most common symptom in diabetics and was observed in 70% of the women. Diminished clitoral sensation was observed in 62.5% of the women, 37.5% complained of vaginal dryness and 41.6% had vaginal discomfort. Orgasmic dysfunction was found in 49% of the women. All these symptoms were significantly higher when compared with controls.
Enzlin and co-workers reported on a study comparing 120 patients with Type 1 diabetes mellitus [11] and 180 controls, which found that 27% of women with Type 1 diabetes reported sexual dysfunctions compared with 15% of female controls; 15% of women with Type 1 diabetes reported two or three problems versus 7% among the control group. Lubrication difficulty was the only problem that was significantly more prevalent in women with Type 1 diabetes (14%) compared with controls (6%).
There have been some important and interesting studies performed in different sociocultural environments (Table 1).
Female sexual dysfunction in diabetic patients with different sociocultural backgrounds.
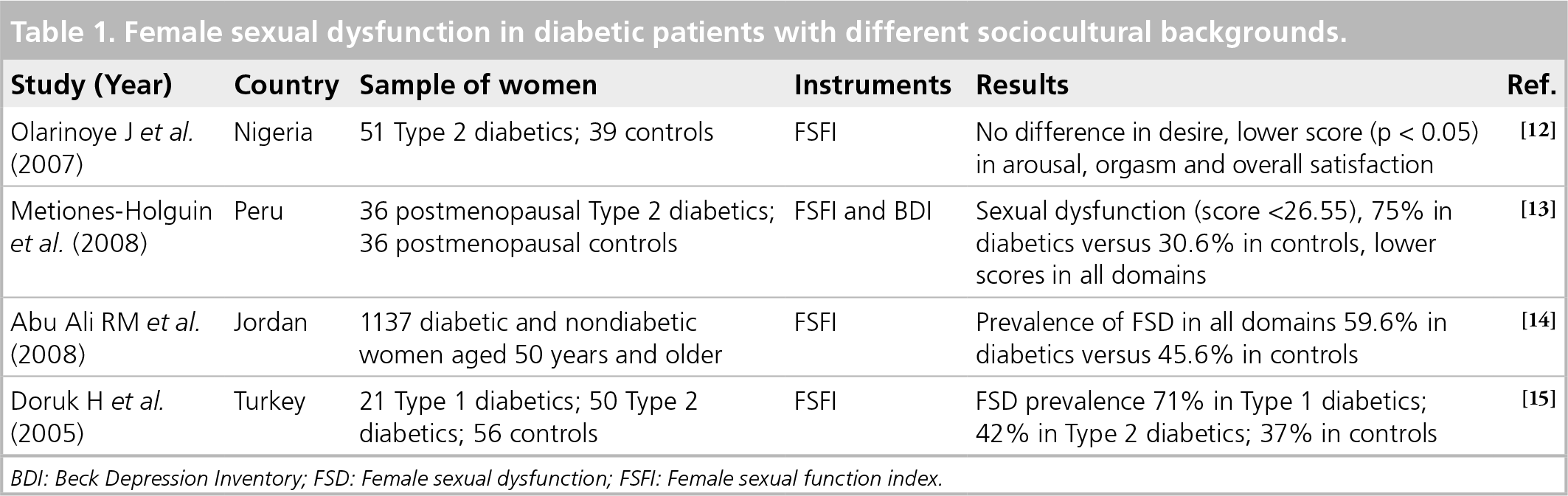
BDI: Beck Depression Inventory; FSD: Female sexual dysfunction; FSFI: Female sexual function index.
In a study among women with Type 2 diabetes in Nigeria, women were assessed using the FSFI questionnaire, which was applied to 51 women with Type 2 diabetes and 39 nondiabetic controls [12]. The FSFI scores in the arousal, pain, orgasm and overall satisfaction domains were all lower in the diabetic women (p < 0.05). There was no significant difference in the scores for the desire domain in the two groups (p > 0.05). Further determinance of FSFI included age, the duration of diabetes illness and a presence of menopause.
In a Peruvian study, 72 postmenopausal women with a stable partner, 36 of whom were diabetic, were studied [13]. Sexual functioning was assessed using the FSFI and depression using the Beck Depression Inventory (BDI) scale. They found no difference between diabetic and control women regarding age, years of schooling, number of children, age at menarche, age at first sexual experience, years postmenopausal or body mass index.
Assuming sexual dysfunction to be a score higher than 26.55, the prevalence of sexual dysfunction among diabetics was 75.0 versus 30.6% in the control group (p < 0.001). Diabetics demonstrated worse scores globally and in all domains of the FSFI: desire, arousal, satisfaction and pain.
In a study in Jordan, data were collected from 1137 married women using the Arabic translation of the FSFI questionnaire [14]. Prevalence of sexual dysfunction in diabetic women 50 years of age or older was 59.6 versus 45.6% in nondiabetic women (p = 0.003). Diabetic women had more dysfunction of desire, arousal, lubrication and orgasm than nondiabetic women.
In a study in Turkey, 127 married women were examined: 21 women with Type 1 diabetes, 50 women with Type 2 diabetes and 56 healthy women as a control [15]. Female sexual functions were evaluated with a questionnaire to assess sexual desire, arousal, lubrication, orgasm, satisfaction and pain. The prevalence of sexual dysfunction was 71% in the Type 1 diabetic group, 42% in the Type 2 diabetic group and 37% in the control subjects. The scores for sexual desire, arousal and lubrication were significantly lower in the Type 1 diabetes group than in the control subjects (p < 0.05). The scores of orgasm, satisfaction, dyspareunia and total sexual function were slightly lower in the Type 1 diabetic group than in the other groups.
In this study, contrary to other previously mentioned studies, the prevalence of sexual dysfunction was significantly higher in the Type 1 diabetic women than in the Type 2 diabetics and control subjects.
Summarizing the above-mentioned studies, it can be stated that for diabetic women:
They appear to experience sexual dysfunctions more frequently in general than age-matched healthy controls;
These findings are independent of the sociocultural environment;
In many studies the degree of the individual distress and suffering is not well documented;
It seems that the most frequently cited dysfunctions are desire and arousal disorder, mainly lubrication difficulties, while orgasmic capacity appears to be less affected;
This pattern is, however, still under debate.
What contributes to FSD in diabetes mellitus patients?
Female sexual dysfunction is a complex clinical phenomenon and is conditioned by various factors (Figure 1). We have proposed the use of a multidimensional model differentiating between pre-existing factors (age, pre-existing sexual difficulties and resources, body image and gender) disease-specific factors (threat, direct pathophysiological effects, comorbidities and drugs) and disease response factors (affective response, individual coping, impact on body image and change in partner dynamics).

Conditioning factors contributing to female sexual dysfunction in diabetic patients.
Applying this model to FSD in diabetic patients is illustrated in Figure 1. Disease-specific biomedical factors can be subdivided into either immediate direct pathophysiological effects on the vascular and neurological components of the female sexual response or indirect effects via typical complications found concomitant with diabetes and comorbidities frequently associated with diabetes.
Among psychosocial factors, pre-existing sexual problems, before the onset of disease, possibly predispose to FSD. Other important psychosocial factors are the affective response to the diabetic disorder, especially depression, coping style with the chronic disease, and the impact of diabetes on body image and on the quality of the relationship.
With this complex and manifold pathogenesis of FSD it is rather difficult to study isolated factors.
In the Turkish study, no factor predicted sexual dysfunction in the diabetic women while further age, poor education, absence of occupation and menopause predicted sexual dysfunction in the control subjects [14].
In the study in Nigeria, age, duration of diabetes and the presence of menopause were risk factors for sexual dysfunction [12].
Regarding direct pathophysiological effects, Erol demonstrated in a study in 2003 that for each genital as well as extragenital site, the mean biotensiometric values were significantly higher in diabetics [16]. Sensation of introitus, vagina, labia minora and clitoris were found to be the most deteriorated genital sites in diabetic women. However, the difference between diabetic women with or without female sexual dysfunction was not significant for these values. The authors conclude that the somatic sensory system is affected by diabetes, however, sexual dysfunction does not always manifest or is directly related to this pathophysiological effect.
To question whether direct diabetic complications have an impact on sexual function is controversial. Enzlin et al. found that women with diabetic women complications did not report significantly more sexual problems compared with diabetics without complications, and that neuropathy, nephropathy and retinopathy were not significantly associated with sexual dysfunction [17]. In the same study, the authors found that there was an association between the number of complications and the number of sexual problems when women with FSD were compared with diabetic women who did not suffer from FSD [17].
Psychosocial factors have not been so extensively studied. There is some indirect evidence concerning the importance of three psychosocial parameters: affective disorders (mainly depression), individual coping with the disease and quality of the relationship. The comorbidity of diabetes with depression has been described in several studies. Salonia used the BDI in his study to assess depression and found that more than half of the patients examined had scores indicating depression [9]. Furthermore, the scores of the BDI showed a strong positive correlation to low sexual desire and arousal problems, and less correlation to orgasmic difficulties.
Enzlin noted some important gender differences regarding the factors associated with sexual dysfunction [17]. In men, but not in women, sexual dysfunction was related to age, BMI, duration of diabetes and diabetic complications. In women, but not in men, sexual dysfunction was related to depression and the quality of the partner relationship.
In the Peruvain study, diabetics had a worse score for depression (11.5 ± 5.6 vs 8.9 ± 4.7; p < 0.03), and a more deteriorated marital relationship (scale of 0–20: 13.4 ± 2.9 vs 15.1 ± 1.9; p < 0.009) [12]. In the same study, however, after adjusting for depression, years of schooling, hysterectomy, marital relationship and age, diabetes mellitus remained an important risk factor for sexual dysfunction (OR: 6.2; 95% CI: 2.0–19.6; p < 0.02). These authors conclude that diabetes mellitus affects all areas of female sexuality and that this condition is independent of depression.
Indirect evidence concerning the impact of individual coping with the disease on sexual dysfunction was found in Enzlin's study [17]. Diabetic women with FSD had more negative appraisal of their diabetes mellitus, had more problems with their emotional adjustment to diabetes, were less satisfied with their treatment, and experienced more impact of treatment on daily life. Diabetic women with sexual dysfunction reported a significantly lower overall quality of marital relationship than women without sexual dysfunction – a difference not found in men.
In a qualitative study in which the inverviewers asked a group of diabetic women about their sexual life, the participants revealed self-blame and embarrassment regarding their diabetes and sexual functioning [18].
Summarizing the studies regarding the conditioning factors contributing to FSD in diabetic patients, the following multidimensional structure arises:
Direct pathophysiological effects on the vascular and neurologic elements of the sexual response are proven, but their importance for the subjectively experienced arousal seems unclear;
The role of diabetic complications in FSD is controversial;
The comorbidity of diabetes with depression plays a major role in the pathogenesis of FSD;
Individual coping with the disease and the quality of the relationship are contributing factors that may be of larger importance than organic changes.
Diagnostic approach
Taking into the account the above summarized contributing factors to sexual difficulties in diabetic women, the diagnostic approach has to combine different elements and methods, as is illustrated in Figure 2:

The diagnostic pathway for diabetic patients with female sexual dysfunction.
Give patients permission to address their sexual concerns. Sometimes this can be done by proactively asking about sexual difficulties. A qualitative study has shown that diabetic female patients may feel too ashamed or embarrassed to talk about their sexual problems in the medical consultation. A useful question in the routine control could be: ‘Some of my diabetic patients remark changes in their sexual life and/or sexual dysfunction. Is this a concern for you?'
Exact descriptive diagnosis. This is carried out by focused questions addressing the different elements of the female sexual response: desire, arousal, orgasm and pain. Is it primary or secondary, global or situational, always or intermittently occurring?
Comprehensive biopsychosocial assessment.
Biological contributing factors
Assessment of the diabetes-related metabolic status and degree and intensity of complications are of course part of the diagnostic workup. This basic medical workup includes drug history of the patient, duration of diabetes, medical history of the patient (especially, other chronic metabolic diseases), and the treatment method for the control of the diabetes;
The age of the patient and the reproductive life phase are important factors to assess, for example, postpartum, perimenopause, menopause, hormonal treatment (hormonal contraceptives or hormone-replacement therapy);
With the help of the gynecologic examination local changes in the vulva and the vagina, especially atrophic changes, can be seen and some basic sensory testing can be performed;
In rare cases, hormones should be measured, especially if there is the suspicion of an androgen deficit.
Psychosocial contributing factors
Questions or questionnaire about the affective state, especially depression (additional use of a standardized questionnaire such as the BDI is recommended);
Questions regarding general coping with the disease, the treatment and the possible distress caused by these factors;
Questions about the relationship, including those about the partner's sexual function, possible conflicts regarding the needs and wishes, and other aspects of marital discord.
By putting all these elements together the physician can establish a multidimensional diagnostic working hypothesis concerning the individual sexual dysfunction or disorder.
Therapy
The therapeutic approach is frequently a combination of interventions targeting the different pathogenetic factors (Figure 3):

The therapeutic approach for female sexual dysfunction in diabetic patients.
Optimizing the diabetic therapy: in one case study, dyspareunia that could be demonstrated in a young diabetic woman disappeared after normalizing the metabolism [19];
Stabilizing the hormonal milieu: in some patients with signs of lack of estrogen and androgens contributing to the sexual dysfunction, hormone-replacement therapy either systemic or local is indicated [9];
Drug treatment with phosphodiesterase (PDE)5 inhibitor. It has been demonstrated, that the use of PDE5 inhibitors may increase the vaginal and clitoridal blood flow, thereby facilitating sexual arousal. The improvement in arousal can be associated with an increase in desire [20];
General counseling about optimizing the way the patient copes with the disease. This can improve compliance and minimize the stress and anxiety patients may suffer from;
Treatment of a coexisting depression, preferably by a combination of drug treatment with an antidepressant without negative impact on libido and arousal, and cognitive behavioral therapy;
Couple counseling. How do both partners view the disease, what are their main concerns and stressors? How do they view the impact of the diabetes on the quality of their relationship and their sex life? How can they overcome communication difficulties? [3]
Summarizing the therapeutic approach, it can be said that diabetic females with sexual dysfunction often need a combined approach that integrates the optimal care for their disease combined with drug and psychosocial interventions targeting frequently existing comborbidities and/or psychosocial pathogenic factors.
Future perspective
Increasing numbers of female patients with diabetes mellitus will increase the demand for sexual counseling and care;
Primary care physicians, internists, diabetes specialists and gynecologists will be confronted with these patients and their problems and they will need some basic training in managing FSD;
Biomedical treatment options will increase, including new substances acting on peripheral and central pathways of the female sexual response;
The interaction of diabetic metabolic status and reproductive hormones (natural stages as well as hormonal contraceptives and post-menopausal hormone therapy) will be of increased scientific interest;
Affective, behavioural and psychosomatic aspects of diabetes mellitus will gain importance;
There will be a need for multidisciplinary care teams, including professionals trained in couple therapy and sexual medicine.
Executive summary
In Western societies, diabetes mellitus has a high prevalence. Worldwide it is estimated that 171 million people suffer from diabetes and it is projected that by 2013 there will be 366 million people affected.
For a long time, men have been recognized to be at risk for developing impaired sexual function and research has mainly focused on sexual problems in diabetic men. The impact of diabetes on female sexual function has been investigated much less.
Appear to experience more frequently sexual dysfunctions in general than age-matched healthy controls, independent of the sociocultural environment.
Although in many studies the degree of the individual distress and suffering is not well documented, it seems that the most frequently cited dysfunctions are desire and arousal disorder, mainly lubrication difficulties, while orgasmic capacity is less affected. This pattern is, however, still under debate.
Direct pathophysiological effects on the vascular and neurologic elements of the sexual response are proven, but their importance for the subjectively experienced arousal is unclear.
The role of diabetic complications is controversial.
The comorbidity of diabetes with depression plays a major role in the pathogenesis of female sexual dysfunction.
Individual coping with the disease and the quality of the relationship are contributing factors that may be of larger importance than organic changes.
Give patients permission to address their sexual concerns.
Perform an exact descriptive diagnosis.
Diabetes-related metabolic status and degree and intensity of complications; duration of diabetes, treatment method for the control of diabetes; drug history; and medical history of the patient (especially other chronic metabolic diseases).
Age and the reproductive life phase.
Gynecologic examination (local changes in the vulva and the vagina, especially atrophic changes).
In rare cases hormones should be measured, especially if there is the suspicion of an androgen deficit.
Questions or questionnaire about the affective state, especially depression (additional use of a standardized questionnaire such as the Beck Depression Inventory is recommended).
Questions about the general coping with the disease.
Questions about the relationship, including those about the partner's sexual function, possible conflicts regarding the needs and wishes, and other aspects of marital discord.
The therapeutic plan includes:
– Optimizing the diabetic therapy;
– Stabilizing the hormonal milieu;
– Drug treatment with a phosphodiesterase 5 inhibitor;
– General counseling about optimizing the way the patient copes with the disease;
– Treatment of a coexisting depression, preferably by a combination of drug treatment with an antidepressant without negative impact on libido, and arousal and cognitive behavioral therapy;
– Couple counseling.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.