
Abstract
The progesterone-receptor (PR) ligand family includes pure agonists, such as progesterone itself, or synthetic progestins, and at the opposite side of the biological spectrum, pure progesterone antagonists, such as onapristone. The actions of these compounds are mostly mediated by the nuclear PR, and appear to be tissue specific. Progesterone-receptor modulators (PRMs) are PR ligands with tissue-specific actions. Uterine actions of antiprogestins and PRMs depend on many factors and treatment duration may play a central role. This review will first summarize the current knowledge on the mechanisms of action of PRMs, with a special focus on the nonpregnant uterus, and describe compounds that are currently undergoing clinical development. Then, clinical effects of PRMs and antiprogestins in the nonpregnant uterus will be described. Finally, pending issues on endometrial safety during chronic administration of PRMs will be addressed.
Mechanisms of action progesterone-receptor modulators
The actions of PRMs in target tissues are mediated mainly by nuclear PRs, which belong to the nuclear-receptor family of ligand-activated transcription factors [1]. Three main isoforms of PR (A, B and C), are encoded by a single gene located on chromosome 11. The long form PRB contains an N-terminal fragment of 164 amino acids, which is absent from PRA. As a consequence PRB contains three transcription-activating domains (AF-1, AF-2 and AF-3) while PRA contains only two (AF-1 and AF-2). PRA and PRB isoforms have similar steroid hormone and DNA-binding activities but have distinct functions depending on the cell type and context of the target gene promoter. Animal PR-knockout models have suggested tissue-specific actions of PRA and PRB [2]. In mice, PRA controls estradiol-induced endometrial proliferation while PRB appears to control breast differentiation and proliferation. Hence, one of the mechanisms of this tissue specificity may be related to the ratio of PR isoforms expression. Additionally, the agonist-bound PR is believed to modulate transcription either by direct action on the general transcriptional machinery or by association with coregulators. Coactivators may be regarded as amplifiers of transcriptional regulation, and include among others, steroid receptor coactivator (SRC) family members and receptor interacting protein 140 [3–5]. Data from the literature are increasing very rapidly to describe a highly complex regulators system [6] including over 200 different molecules. A tissue specificity of PR-SRCs interactions have been described in mice suggesting that SRC1 is predominantly associated with PR transcription activation in the uterus while SRC-3 may play a similar role in the breast [7–9]. PR can also interact with transcription corepressors, such as the nuclear receptor corepressor (NCoR), and the silencing mediator of retinoic acid and thyroid hormone receptor (SMRT). This usually occurs in the presence of an antagonist ligand. However, additional mechanisms are probably involved. For example, the mixed agonist–antagonist aso-prinil (J867, formerly Schering, NJ, USA/TAP, IL, USA) allows the recruitment of coactivators by PR in vitro while the antagonist mifepristone (RU 486, Exelgyn, Paris, France) does not. However, none of the compounds has progesterone-like ability to oppose estrogen in the rat endometrium [10].
An additional PRC isoform able to bind to PRA and PRB isoforms and inhibit their biological actions has been described. Thus far, its expression is limited to the amniochorion and placenta [11,12]. Finally, progesterone can have rapid effects resulting from the actions of specific receptors localized to the plasma membrane (mPR) [13], which bear structural, but virtually no sequence homology to the G-protein-coupled receptor family. Interestingly, mPR have been detected in human myometrium, where progesterone regulates multiple kinase-mediated pathways, which could modulate myometrial contractility and be involved in spontaneous labor induction [14].
In the human endometrium, the expression of both PRA and B isoforms, as well as of their coregulators (SRC1, NCoR and SMRT), has been described [15–17]. Both isoforms and coregulators expression is modulated along the menstrual cycle in a compartment-specific manner [15,18]. The subnuclear localization of PR isoforms has also been shown to vary during the menstrual cycle [19], although the physiological significance of this phenomenon in the endometrium remains to be determined [15,16,20].
Interactions of this whole system of PRs and coregulators with the transcriptional machinery are complex. Coregulators are enzymes that modify the local chromatin, and provide protein reactants for controlling the various steps of transcription [6]. Since other steroid hormone receptors share the same coregulators with PR, there is an interaction between the different steroid receptors present at the transcription initiation site. Finally other regulators actions, mediated by various intracellular signaling pathways, such as growth factors, interact with this complex, which introduces an additional ‘cross talk’ between steroid receptors and growth factors for example.
Currently available and/or under clinical development progesterone-receptor modulators
Mifepristone (RU 486) was the first PRM to be evaluated in women in the early 1980s [21]. This compound exerts antiprogestin activity in the presence of progesterone and can have agonist effects in the postmenopausal endometrium [22]. Since then, many PRMs have been developed (Table 1).
Main progesterone-receptor modulator compounds undergoing clinical development.
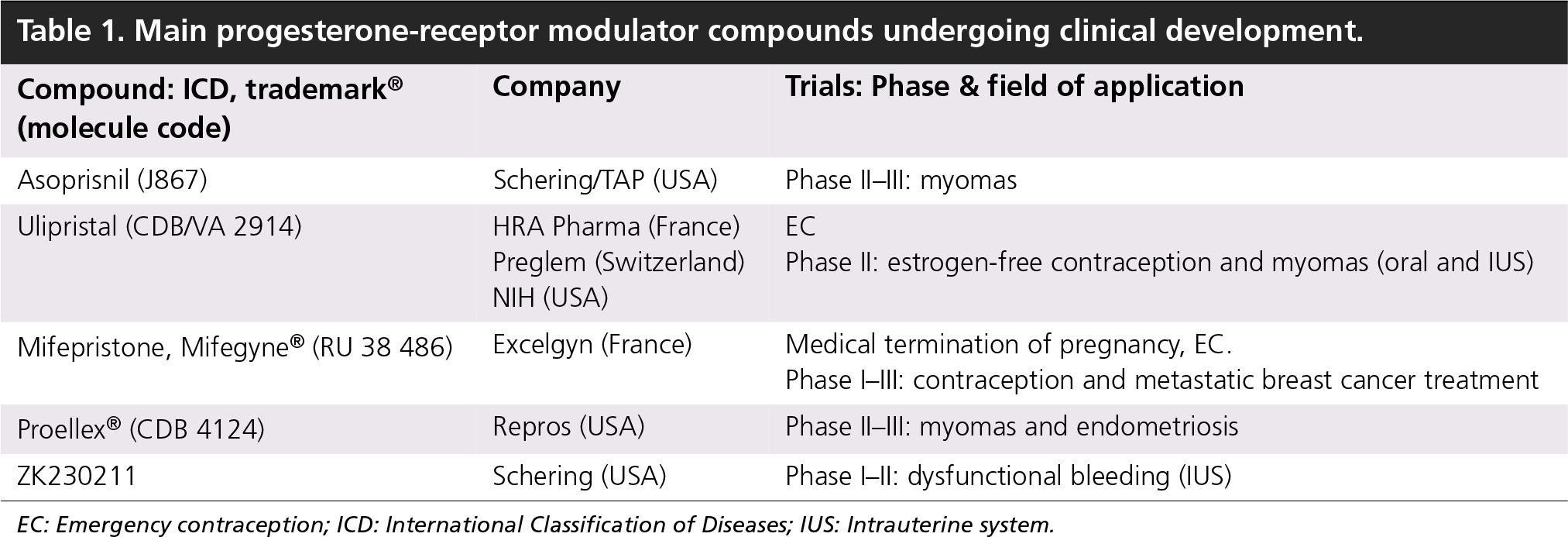
EC: Emergency contraception; ICD: International Classification of Diseases; IUS: Intrauterine system.
All antagonistic or mixed agonist–antagonist compounds that have reached the clinical step are steroid derivates (Figure 1). Some of them are testosterone derived (e.g., Mifepristone and Asoprisnil), while others are progesterone-derived (Ulipristal, HRA Pharma, Paris, France/Preglem, Geneva, Switzerland) (Figure 1). All the compounds are carbon 11-substituted with a bulky residue. The presence of this residue prevents the three-dimensional agonist configuration of the ligand–receptor complex [10]. As a consequence, the interaction with the transcriptional machinery is impaired. The different compounds have in common a potential antiprogestogenic activity, although it might be more or less pronounced. However, the activity of PRMs has been shown to depend on the cellular context, dose and duration of treatment and presence or absence of progesterone [23,24]. The cell-specific expression of PR isoforms and coregulators may also be involved. As previously discussed, additional mechanisms are probably implicated, including cross talk with growth factor, cytokines and peptidic hormones receptors. PRMs have different affinity for steroid hormones receptor, including glucocorticoid receptor (GR). While mifepristone strongly binds to GR and is used to treat Cushing's syndrome, ulipristal has a very low affinity for this receptor and asoprisnil a reduced affinity, suggesting a higher specificity and a potential new subclass of dissociated PRMs that have reduced antiglucorticoid activity [25–27].

Progesterone-receptor modulators.
Endometrial effects of progesterone-receptor modulators
Data from studies evaluating the potential use of PRMs for contraception and treatment of myomas have shown that their effects on the endometrium could be dose and duration dependent.
Very short-term administration/single dose
This very short-term administration has clinical applications for bleeding control in progestin-only pill users, for emergency contraception (EC) and during IVF cycles.
Proof-of-concept animal studies have shown that short-term administration of PRMs could modulate the uterine environment and interfere with implantation and early pregnancy. Banaszak et al. found that the inhibition of progesterone action by the PR antagonists ZK 137.316 in intact and ovariectomized baboons altered the action of chorionic gonadotropin on the endometrium at the time of uterine receptivity [28]. This PRM reduced the epithelial plaque reaction, completely inhibited α-smooth muscle actin (αSMA) expression in stromal fibroblasts, and induced the reappearance of the PR and estrogen receptors (ERα) in epithelial cells. However, this treatment had no effect on the expression of glycodelin in the glandular epithelium as a short-term treatment (10 days). These results indicate that blocking the action of progesterone on the endometrium even for a short period of time has a profound effect on the hCG-induced response in stromal fibroblasts. Using an in vitro model of human blastocyst adhesion to cultured human endometrial cells, Petersen et al. [29] have demonstrated that the antiprogestin Org 31710 has anti-attachment properties. The mechanism of this effect has to be determined since the morphology of endometrial cells was not modified (e.g., pinopodes developed normally) neither was the expression of biochemical markers of implantation such as glycodelin A and leukemia inhibiting factor. Recently, Gemzell-Danielsson et al. have shown that mifepristone, but not levonorgestrel, inhibits human blastocyst attachment to an in vitro endometrial three-dimensional cell culture model [30].
This body of evidence can be integrated in the potential use of mifepristone and other PRMs for EC, although some of these studies were not conducted with this initial purpose [31]. The luteinizing hormone (LH) surge blockade was the primary mechanism on which antiprogestins were used for EC. The prevention of implantation is also a potential mechanism to explain the efficacy of PRMs for EC [32–34]. Different doses of mifepristone for EC have been compared in clinical trials [35,36], all of them resulting in a marked decrease in the number of expected pregnancies. Mifepristone has the distinct advantage to be effective up to 120 h after unprotected intercourse whereas the Yuzpe protocol or levonorgestrel efficacy is limited by license to the initial 72 h [35–38]. Levonorgestrel may be considered between 73 to 120 h but women should be advised of the limited evidence for its use [39]. Ashok et al. compared 100 mg mifepristone versus Yuzpe method for EC [40]. Mifeprisotne seems to be highly effective (0.6% pregnancy vs 3.6% with Yuzpe method) with high patient acceptability and fewer side effects compared with the standard Yuzpe regimen. However, the delay in the onset of menstruation was longer with mifepristone. Currently, mifepristone is used for EC in China [41] and may be authorized in different countries in the future. Ulipristal has also been evaluated for EC in a randomized trial versus levonorgestrel [42]. Based on the estimated cycle day of unprotected intercourse, 85 and 69% of anticipated pregnancies, respectively, were averted in a group of 1500 women.
Additional attempts were made in the past to use PRMs as ‘menses regulators’ [43,44]. Mid-luteal phase administration of mifepristone produces bleeding within 72 h and inconstantly induces luteolysis, with a decrease in serum follicle-stimulating hormone, estradiol and progesterone concentrations. Administration of mifeprisotne in the late luteal phase does not disturb menstrual cycle length, bleeding patterns, ovulation, or hormonal parameters in treatment or post-treatment cycles. However, the drug alone cannot be used as a ‘menses regulator’ or ‘once-monthly pill’ since some pregnancies do continue.
Progesterone-receptor modulators have also been evaluated during IVF cycles where they could block the LH surge and avoid premature luteinization as an alternative to GnRH analogues. One clinical pilot study has demonstrated that mifepristone is effective for the prevention of premature LH surges and/or premature luteinization in women undergoing controlled ovarian hyperstimulation for in vitro fertilization [45]. The endometrial morphology was normal in women treated with mifepristone and hCG, however the expression patterns of glycodelin, IGF-binding protein-7, glutathione peroxidase-3, and solute carrier family 1 member 1 showed a striking absence of upregulation in patients treated with mifepristone compared with controls. The evaluation of endometrial receptivity status during IVF cycles using antiprogestins requires additional evaluation, including the definition of the optimal dose and duration of antiprogestin administration.
Breakthrough bleeding is the most common reason for discontinuing progestin-only contraception. Studies evaluating the endometrial effect of PRMs in association with progestins have suggested that monthly administration of antiprogestins could improve cycle control in women using the progestin-only pill [46,47] or contraceptive implants [48]. Although the limited body of evidence currently available [48] does not demonstrate a decrease in contraceptive efficacy, this point has to be confirmed in large-scale studies. The cellular mechanism of this effect is still under evaluation. During the physiological menstrual cycle [49,50], progesterone withdrawal results in an upregulation of inflammatory mediators, production of matrix metalloproteases (MMPs), a leucocyte influx and expression of stromal VEGF receptor, kinase insert domain-containing receptor in the upper endometrial zones. There is coincident hypoxia and an upregulation of VEGF. VEGF binds to its type 2 receptor, kinase insert domain-containing receptor, and there is a paracrine/autocrine action on the upregulation of MMP production in the same endometrial upper zone stromal cells. The potential mechanism(s) involved in abnormal bleeding during synthetic progestin use include changes in the ratio of pro- versus anti-angiogenic factors; alterations in metalloproteinases and tissue inhibitor of metalloproteinases (TIMP); changes in tissue factor a known hemostasis mediator in the endometrium; and increased endometrial leukocytes with a particular emphasis on uterine natural killer (uNK) cells [51]. The first report of upregulation of estrogen and PR by mifepristone was made in women complaining of vaginal bleedings while using Norplant [52]. Mifepristone administration (200 mg at the beginning of the bleeding) in addition to the progestin delivering implant was associated with a downregulation of PR subtype B and an upregulation of ER, compared with women with the implant alone. Women treated with mifepristone also demonstrated a tendency to increase ovulation rates and reduced vaginal bleeding. The effect of mifepristone on endometrial steroid receptors was consistent with functional inhibition of progesterone's effects. Histological findings in starters of depo-medroxyprogesterone acetate (DMPA) have shown that the synchronous maturation of glands and stroma seen in normal secretory endometrium transforms following DMPA treatment to confluent stromal cell decidualization with small, attenuated glands [53]. Following mifepristone, the endometrium reveals altered maturation. The glands show persistent subnuclear vacuoles, more characteristic of early luteal phase, and stromal edema, more characteristic of mid- to late-luteal phase. Progesterone and estrogen receptors and signaling pathways may be modified as well as cell proliferation as shown in DMPA users treated with mifepristone [54]. Short-term exposure of mifepristone (single dose of 25 mg) increases the expression of endometrial ERα, PRAB, PRB and SRC-1 and promotes cell proliferation. Prolonged exposure to mifepristone (25 mg twice a month for three months) does not alter the suppression of these receptors that are caused by DMPA and continues to result in endometrial atrophy. Endometrial apoptosis is downregulated as well in these patients in the short term while longer-term administration does not result in any significant modification of apoptotic rates [55]. Modulation of endometrial cells environment such as immune cells chemoattraction or MMP expression has also been reported in new DMPA users treated with mifepristone [56], in whom the decreased rates of breakthrough bleeding are associated with decreased MMP-1 and −9 expression and fewer mast and T cells.
Mid- to long-term administration
Initial data obtained in nonhuman primates have suggested that antiprogestins could induce a profound endometrial atrophy and antiestrogenic effects [57–61], but this effect has not been reproduced in clinical studies. The nonhuman primate endometrium is thus not a proper model to investigate the potential effects of antiprogestins in the uterus. Studies evaluating mid- to long-term effects of PRMs on the human uterus have been conducted in normal volunteers for estrogen-free contraception, or in women with dysfunctional bleeding, mostly related to myomas. The common features of these studies were the induction of amenorrhea and blockade of the LH surge without impairment of folliculogenesis. The endometrial effects of selective PRMs (SPRMs) are, at least in part, related to the specific endocrine environment induced by these compounds. The main endocrine effect of PRMs is to inhibit the LH surge induced by estrogens [62,63] without impairing follicular development, although the precise mechanism of these effects still remains to be determined. As a consequence, plasma estradiol levels remain in the normal range of a follicular phase [64–67].
Clinical studies of contraceptive effects of PRMs have shown a dose- and duration-dependent efficacy. Daily low dose (<2 mg/day) mifepristone failed to inhibit ovulation [68], however, a daily dose of 0.5 mg mifepristone slightly delayed endometrial development and glandular diameter was significantly reduced. Daily 2–5 mg of mifepristone inhibits ovulation and secretory transformation of the endometrium [69–71]. VA 2914 5–10 mg daily can inhibit ovulation, without inhibiting endogenous estrogen secretion [65]. The endometrial aspect is predominantly secretory, although this aspect frequently differs slightly from the usual secretory aspect, as a result of stromal compaction and inactive cystic-like glandular appearance. Asoprisnil has also been demonstrated to inhibit the LH surge, with estradiol levels remaining in the follicular phase physiological range [72]. The histological aspect has been described as nonphysiological secretory with compact stroma and dilated glands with few mitotic figures. Interestingly, the contraceptive efficacy of weekly mifepristone (25 or 50 mg) has recently been evidenced by Pei et al., suggesting a persistent effect of mifepristone [73]. The effects on the endometrium reported in this study are limited to bleeding patterns. During the first 3 months no differences were observed between the two groups while during the following 3 months women receiving 50 mg/week had significantly less bleeding days.
The control of uterine bleeding by the administration of PRMs in women with myomas has been documented with mifepristone and asoprisnil, allowing amenorrhea in 80–90% women after the second month of treatment. Intrauterine administration of PRMs has also been evaluated in women scheduled for hysterectomy as a result of heavy or painful menstruations. Heikinheimo et al. compared ZK230211 versus levonorgestrel intrauterine releasing systems [74]. The number of days with bleeding and spotting was significantly higher in the levonorgestrel group. The mechanism of this endometrial action is still unknown. Endometrial morphology in the ZK-IUS group, demonstrated the absence of stromal decidualization and the presence of dilated glands. Epithelial cells showed little proliferative activity and secretory morphology. Proliferation markers such as Ki-67 and phosphorylated histone 3 were not higher in the ZK-IUS group. Finally, PR expression and IGFBP1 protein expression were higher in the ZK-IUS group. Vascular modifications observed in monkeys, including hyaline degeneration in spiral arteries walls [75], have not been observed in the human endometrium. The effects of mifepristone, ulipristal or ZKs on human spiral arteries have not been described in detail. The vascular impact of a daily asoprisnil administration for 3 months has been evaluated by Williams et al. [106]. Unusual thick-walled muscular arterioles and prominent aggregations of thin-walled vessels were present in endometrial stroma. Such aspects have not been observed after continuous administration of VA 2914 for 3 months [Unpublished Data]. Modifications of microvessel maturity may also be involved. In fact, intrauterine administration of levonorgestrel induces immature microvessels [76], and antiprogestins may exert the opposite effect. Modifications of the MMP system [56], as well as regulation of the VEGF system [77–80], may also be involved, although in vivo data are still lacking in this field.
Effects of selective progesterone-receptor modulators on myomas
Progesterone-receptor modulators evaluated for medical treatment of myomas (mifepristone, asoprisnil and ZK compounds) (Table 1), have demonstrated the dual benefit of reducing tumor volume and induce amenorrhea. Mifepristone has been the most widely evaluated compound and the available data have been summarized by Steinauer et al. [81]. Tumor volume is reduced by 40–60%. Interestingly, no dose–effect relationship has been observed [82].
Asoprisnil has also been studied for this indication. Amenorrhea and tumor volume reduction were observed in a similar way, although in that case Chwalisz et al. reported a dose-dependent effect of asoprisnil [83]. Proellex® is another PRM evaluated for myoma treatment, showing the same level of efficacy both on bleeding and tumor volume, although data are only available from the manufacturer's website. Finally, ulipristal is also currently being evaluated for the treatment of myomas.
Different cellular mechanisms of action have been suggested. Studies using asoprisnil or ulipristal have shown antiproliferative and proapoptotic effects in cultured leiomyoma cells [84–86]. Modulation of growth factors (EGF, IGF1 and TGFβ3) and their signaling pathway may be involved in tumor growth control during PRM treatment [87]. However, those mechanisms of action are probably complex since Maruo et al. recently reported dual actions of progesterone on myoma growth; one is to stimulate growth via EGF1 and BcL2, and the other is to inhibit growth downregulating IGF1 expression. This dual action could explain the inconstant action of levonorgestrel-IUS on myoma size [88]. Finally, interaction with angiogenic factors may play a role. VA 2914 can inhibit VEGF and adrenomedullin (ADM) expression in myoma cells [89].
Endometrial effects of progesterone-receptor modulators: the safety issue
The endometrial effects of antiprogestins are a subject of controversy, related to the specific aspect of the endometrium observed during treatment [90]. Since they had not been previously observed, it is currently discussed to define a new histological classification to allow an accurate description of these specific aspects. In fact, the usual classifications using proliferative, secretory, menstrual as well as atrophic or hyperplatic items may not be appropriate, as discussed below.
Studies in both human and animal endometrium have demonstrated that, in addition to their expected progesterone-antagonist properties, these substances may display unanticipated effects. These include ‘proliferative (estrogen-like)’ and ‘antiproliferative (antiestrogen)’ as well as progesterone-agonist actions. These complex effects depend, among other things, on the hormonal status, the animal model selected, and the dose of PR ligand used [91–93]. It is also important to consider that the determination of the endometrial effects of PRMs is based on variable criteria. Earlier studies used histological analysis and studies of enzymes such as estradiol dehydrogenase and DNA polymerase-α [22]. More recently, proliferation markers such as Ki67, antiphosphorylated histone H3 antibody (phospho H3) and mitotic protein monoclonal antibody (MPM)-2 [94] have been used. Other methods of evaluation are histological dating as described by Noyes in 1950 [95], steroid-receptor expression levels, apoptosis markers or endometrial differentiation markers, (such as glycodelin, Hoxa 10, integrins, leukemia-inhibiting factor, cyclo-oxygenase 2 and calcitonin). Genomic identification of endometrial PR-regulated pathways, especially during the implantation period, has also been used to determine the effects of PRMs [96,97]. Catalano et al. have studied endometrium of women under a single dose of mifepristone during the secretory phase [96]. They found a role of the Wnt, chemokine, MMP and prostaglandin pathways in receptivity and early menstrual events. Obviously, conclusions based on the evaluation of different markers in different species can lead to discrepancies. Additionally, endometrial thickness is usually assessed using vaginal ultrasonography. However, endometrial thickness determined by ultrasound examination is poorly correlated to histologically defined proliferation. In a prospective trial in premenopausal women, ultrasound images appeared to correlate well with endometrial biopsies when endometrial thickness was less than 5 mm and showed only benign changes [98]. This may be related to edematous changes, cyst formation, the collection of fluid in the lumen of dilated glands or to the presence of benign stromal thickening through an increase in collagen production in the stromal cells [99–101].
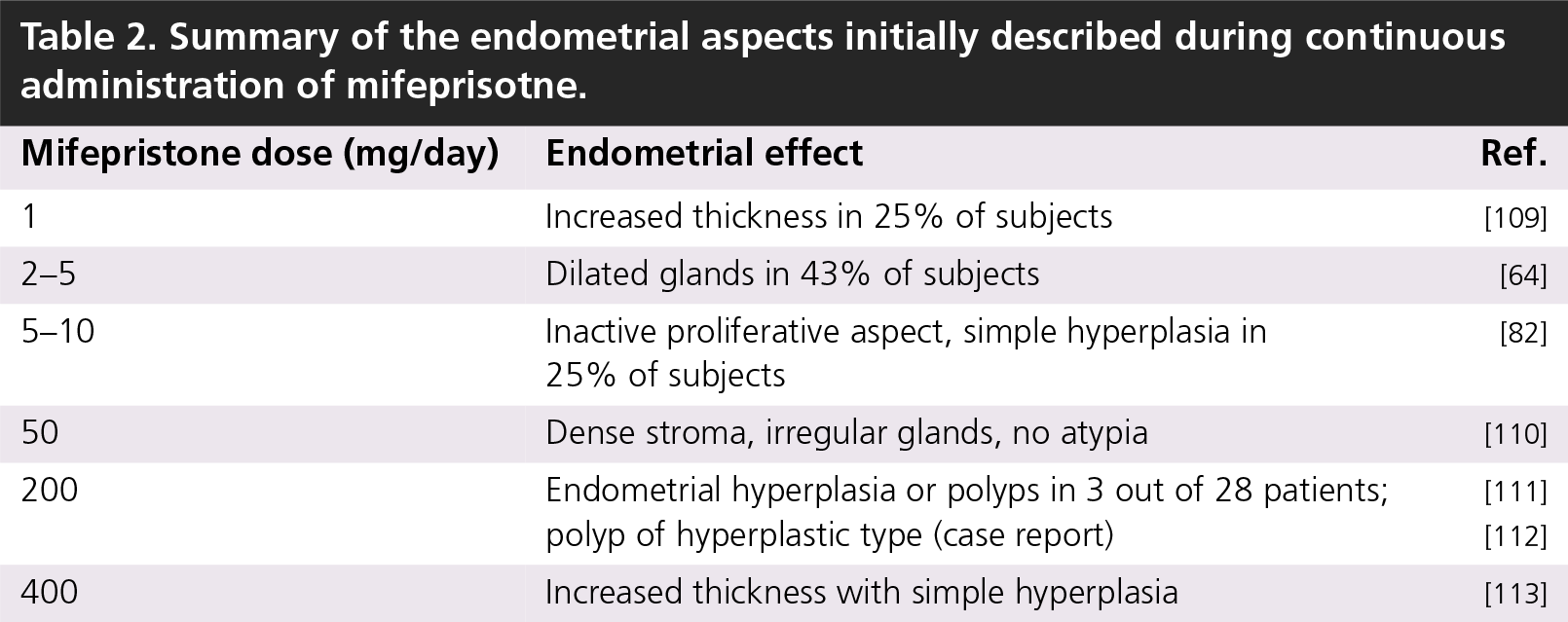
Histological analyses of the effects of mifepristone in the premenopausal endometrium have shown that different aspects, initially related to hyperplasia, could be observed without a clear dose dependency (Table 2), and have raised the issue of safety. It shortly appeared that the description of these endometrial aspects was impaired by the absence of an adequate histological classification [90]. During a meeting at the NIH in April 2006, a panel of pathologists blindly reviewed endometrial biopsies obtained after 3 months or more of treatment with different PRMs. The panel concluded that biopsies had an unusual architecture that could be characterized as glandular dilatation [90]. There were few mitotic figures, probably caused by the antiproliferative effect of PRMs. The biopsies could not be classified in either secretory or proliferative endometrium. It was thus concluded to be a specific aspect of the endometrium during mid- to long-term PRM treatment. Recently, histological ultrasound and hysteroscopic aspects observed in patients treated with mifepristone for 6 months were nicely correlated by Baird et al. [102]. This is the longest term study published to date. The ultrasound aspects showing cystic aspects of the endometrium and cervix could be correlated to a marked cystic dilation of the endometrial glands. This aspect was regressive 4 weeks after treatment discontinuation. None of the endometrial biopsies showed hyperplasia or atypia. Interestingly, in postmenopausal women treated with estradiol and onapristone [103] and compared with estradiol-only treatment, all endometrial biopsies showed a physiological proliferative aspect of the endometrium. A similar pattern and intensity of immunostaining for steroid hormone receptors and proliferation markers was observed in all subjects. By contrast, mifepristone [22] has shown agonistic and antiproliferative effects in postmenopausal endometrium.
Summary of the endometrial aspects initially described during continuous administration of mifeprisotne.
Although additional large-scale studies are needed to define the long-term effects of antiprogestins in the endometrium, currently available data are reassuring since there are no signs of hyperplasia or atypia. Additionally, the specific endometrial aspect observed during treatment returns to baseline shortly after treatment discontinuation.
Conclusion
Progesterone-receptor modulators are a class of steroidal derivates with potential applications in the fields of contraception, dysfunctional bleeding control, medical treatment of myomas, and breast cancer treatment or prevention.
Although the evaluation criteria are not homogeneous among the available studies, it appears that PRMs can induce specific ‘nonphysiological secretory’ aspects of the endometrium. Recent studies suggest that this aspect is associated with low mitotic activity. Although all PRMs seem to induce similar aspects, compound specific differences may be seen, in particular vascular modifications.
Owing to the unsolved question of endometrial safety during long-term treatment, clinical development of PRMs is currently limited to short-term applications, such as EC, bleeding control and obstetrical indications.
Future perspective
The development of PRMs within the next 5 to 10 years will depend on the results of the existing clinical trials as well as the studies, which are currently being undertaken. The use of mifepristone for EC is already currently ongoing in China, and Ulipristal will be available for the same indication in 2008. The main interest of these compounds compared with levonorgestrel is that they can be used with a high efficacy up to 5 days after the exposed intercourse.
Long-term use for contraception, treatment of myoma, or endometriosis will require more studies. In fact, specific new endometrial histological features have been identified in the biopsies performed in women treated with PRMs, especially for more than 3 months. Endometrial thickness measured by ultrasound scans can be increased, potentially suggesting the existence of endometrial hyperplasia [104]. Initial reports of endometrial histology in women treated with mifepristone have indeed reported some degree of hyperplasia. Recently available data demonstrate that this aspect is rather correlated with cystic dilated glands showing very limited mitotic activity [78,96,105,106], referred to as PRMs Associated Endometrial Changes [105]. However, the abnormal aspect observed on ultrasound scans may lead physicians to ask for endometrial biopsies and to eventually interrupt treatment. Association of SPRMs with sequential progestin administration, as well as new treatment schedules including drug-free intervals will be evaluated in the near future to control endometrial thickness.
Although this has not been discussed in this review focused on the uterus, use of PRMs in breast cancer treatment or prevention in women with a high risk will be studied as well. Some clinical data are already available on metastatic breast cancer treatment with PRMs [107]. Importantly, a high efficacy of mifepristone has been recently reported in preventing breast cancer development in a breast-specific BRCA1-knockout mouse model [108].
Executive summary
The mechanisms of action of progesterone-receptor modulators are still incompletely understood.
Progesterone-receptor modulators already have several applications in women's health, such as emergency contraception, pregnancy termination, management of early fetal demise and cervical maturation.
The main indications that will be developed in the future include dysfunctional bleeding and preoperative treatment of uterine myomas. They could also be developed as an estrogen-free contraception, for treatment of endometrisosis and prevention and treatment of breast cancer.
The endometrial safety of those compounds needs to be raised before allowing long-term continuous administration.
Association of progesterone-receptor modulators with sequential progestin administration, as well as new treatment schedules including drug-free intervals, will be evaluated in the near future to control endometrial thickness.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending or royalties.
No writing assistance was utilized in the production of this manuscript.