
Abstract
Although the incidence of breast cancer has increased, there is a concurrent decrease in the death rate, and the outlook for women with early-stage breast cancer remains positive. The current 5-year survival rate of women diagnosed with breast cancer is nearly 90%, due, in part, to the use of effective adjuvant therapies that often include aromatase inhibitors. However, long-term treatment with these therapies is known to have adverse effects on bone metabolism, leading to bone loss. Bone loss during adjuvant endocrine therapy may be higher than that observed during menopause and may require more potent therapy. Although there are approved treatments for osteolytic bone lesions from bone metastases, there is no approved therapy for bone loss associated with adjuvant cancer therapy. Bisphosphonates have demonstrated promising results in this setting, and zoledronic acid is currently under consideration by the US FDA and Europe (EMEA) for the treatment of aromatase inhibitor-associated bone loss.
Breast cancer is one of the most common cancers among women and, in the USA, will account for an estimated 26% of new cancer diagnoses and 15% of cancer-related deaths in women in 2007 [1]. Although the incidence of breast cancer has increased over the years, advances in the screening, diagnosis and treatment of this disease have greatly improved overall survival rates. The 5-year rate of survival in the USA from 1996 to 2002 was 89% [1]. As a result, patients receive anticancer therapies for longer durations than they had in the past, increasing their risk for side effects from these therapies. For example, cytotoxic chemotherapy and hormonal therapy agents have been linked to bone loss, and patients with early-stage breast cancer survive long enough for the cumulative effects of cancer treatments to manifest in fractures. Moreover, women undergoing treatment for breast cancer often have pre-existing risk factors for bone loss, including lifestyle and genetic factors, as well as existing or treatment-induced postmenopausal status in younger patients [2,3]. For example, women without breast cancer who are more than 65 years of age (postmenopausal) have a reported mean bone mineral density (BMD) T-score of −1.26, which is in the osteopenic range [4]. In addition, breast cancer itself may be associated with an increased incidence of vertebral fractures, as one study found that vertebral fractures occurred five times more frequently in patients with breast cancer than in a healthy population (odds ratio: 4.7; 95% confidence interval = 2.3, 9.9) [5]. Women affected with bone loss have a greater risk of developing bone fractures, experiencing associated morbidity and functional impairment and incurring increased healthcare costs. Although vertebral fractures may be asymptomatic, they are still associated with clinically relevant morbidity, including decreased physical function and social isolation, which negatively affects the patient's overall quality of life. This may be especially challenging for the elderly, who may have comorbidities or pre-existing impairments in their quality of life [6]. Increasing survival rates will enlarge this subpopulation of elderly patients with breast cancer who have been under-represented in clinical trials.
These reports underscore the importance of maintaining bone health in patients undergoing treatment for breast cancer. Strategies for the prevention of bone loss include lifestyle changes, diet modifications and bisphosphonate treatment. The goal of these strategies is to maintain bone health to prevent or delay the onset of fragility fractures that can undermine the patient's functional autonomy, thereby preserving the patient's quality of life throughout the continuum of care.
Causes of cancer treatment-associated bone loss
Accelerated bone loss during cancer treatment is a relatively common but under-recognized complication in the primary care setting in women receiving long-term estrogen-reducing therapies. Since many breast cancers are estrogen-receptor positive (ER+) and may be stimulated to grow by estrogen, interfering with estrogen signaling is an effective way of preventing disease progression. Treatments can block estrogen signaling by inducing ovarian ablation, blocking the formation of estrogen or functioning as complete or partial antagonists of the estrogenic signaling pathway. These agents typically produce premature menopause or temporary amenorrhea during treatment in premenopausal patients. Bone integrity is harmed because estrogen plays an important role in maintaining bone health by stimulating new bone formation and inhibiting bone resorption [3].
Loss of estrogen signaling, acceleration of bone loss and increases in fracture risk can occur in response to both cytotoxic and hormonal therapies. For example, cyclophosphamide is a major cause of hypogonadism from ovarian ablation. Indeed, the efficacy of cyclophosphamide-based regimens may be enhanced by the resulting loss in estrogenic signaling in patients with ER+ tumors, which results in bone loss [7]. For example, Bruning and colleagues reported that women who became amenorrheic after cyclophosphamide-based chemotherapy had lumbar spine BMD values that were 9% lower than age-matched BMD averages [8]. Furthermore, a large, retrospective cohort study of 14,604 women with early-stage breast cancer investigated the combined prevalence of osteoporosis and osteopenia at the 31-month follow-up in patients who did (n = 8762) or did not (n = 5842) receive anticancer therapies [9]. After adjustment for significant covariates, patients who received anticancer therapies had a 30% higher risk of osteopenia/osteoporosis than patients who did not receive such therapies.
Aromatase inhibitors (AIs), such as anastrozole, exemestane and letrozole, are approved for the treatment of metastatic breast cancer and as adjuvant therapy for early-stage ER+ breast cancer in postmenopausal women. These agents have become a popular treatment alternative in the adjuvant setting as they have improved efficacy and general tolerability compared with tamoxifen [10–12]. However, because AIs effectively suppress residual estrogen levels by approximately 90% in postmenopausal women, they are often associated with bone loss and increased risk of fractures (
Adjuvant aromatase inhibitor studies in breast cancer.
Safety-evaluable patients.
Letrozole versus placebo.
ATAC: Anastrozole, Tamoxifen, Alone or in Combination; BIG 1–98: Breast International Group 1–98 collaborative group; IES: Intergroup Exemestane Study; NCIC CTG: National Cancer Institute of Canada Clinical Trials Group.
Similar results to those observed in the ATAC study have been observed in the Zometa®-Femara® (zoledronic acid and letrozole) adjuvant synergy trial (Z-FAST), the Breast International Group 1–98 (BIG 1–98) trial, and the Intergroup Exemestane Study (IES) trial. Results from Z-FAST, which studied the prevention of AI-associated bone loss (AIBL) in postmenopausal women with early-stage breast cancer, demonstrated that patients receiving letrozole had 2.6% and 2.1% decreases in lumbar spine and total hip BMD, respectively, after 1 year of therapy [16]. In the BIG 1–98 trial, patients receiving the AI letrozole experienced significantly more bone fractures than patients receiving tamoxifen (p < 0.001) [11]. In the IES trial, patients receiving the AI exemestane experienced significantly more skeletal fractures than patients receiving tamoxifen (7.0% versus 4.9%, respectively; p = 0.003) [12]. However, in the latter two AI studies there were no protocols for BMD screening, supplemental calcium and vitamin D, or bisphosphonate use; therefore, these patients would be expected to have a higher risk of fractures than that of patients receiving the more recent standard of care as outlined by the American Society of Clinical Oncology [17]. Tamoxifen displays estrogen agonist activity in bone and has been associated with lower levels of bone loss and fractures compared with AIs in postmenopausal women [18]. However, tamoxifen does not appear to provide sufficient protection to bone because recent preliminary data from a clinical trial suggests that 23.7% of patients are osteoporotic and 41.5% of patients are osteopenic after 5 years of tamoxifen treatment [19]. Furthermore, tamoxifen has shown fewer skeletal protective effects than estrogen and bisphosphonates in postmenopausal women and has been associated with significant bone loss in premenopausal women [20,21]. In premenopausal women with breast cancer, an association between the bone loss from tamoxifen and increased risk of fractures has not yet been established, and skeletal changes after discontinuation of tamoxifen have not been evaluated.
In a placebo-controlled National Cancer Institute of Canada Clinical Trials Group (NCIC CTG), MA-17 trial in postmenopausal women who had completed 5 years of tamoxifen therapy, patients receiving the AI letrozole experienced more bone fractures than patients receiving placebo; however, the difference did not achieve statistical significance after a median follow-up of 30 months (p = 0.25) [15]. Nevertheless, in a BMD substudy analysis at 24 months, a significant decrease in lumbar spine and total hip BMD was observed in patients receiving letrozole compared with patients receiving placebo (p = 0.044 and p = 0.008, respectively) [22]. Longer follow-up may be necessary in order to evaluate the clinical implications of the observed bone loss in this study.
Although fragility fractures can occur in any bone, fractures of the hip, vertebra and wrist are most commonly linked to bone loss. The bone loss associated with AIs has been reported to be approximately 1.4%/year compared with 1% after menopause [23,24]. Bone loss has long-term implications on a patient's risk of fractures. Decreases in BMD result in exponential increases in fracture risk [2]. For example, a 10% to 15% decrease in BMD (−1 in T-score) is associated with an approximately doubled risk of fracture [2]. In turn, fractures can lead to decreased quality of life. Fractures result in acute pain, potentially disabling skeletal instability, and the cumulative erosion of physical functioning and emotional well being. Fractures can also lead to increased mortality. A retrospective analysis of a Phase III clinical trial in patients with bone metastases from breast cancer (n = 1130) demonstrated that fractures were associated with a 32% increased risk of death [25]. Therefore, because the AIBL and bone loss associated with other cancer therapies may be accelerated in relation to normal postmenopausal bone loss, more aggressive observation and treatment (i.e., intravenous versus oral bisphosphonates) may be necessary to prevent fractures. As bone loss is manageable with available therapies, and AIs have demonstrated potent efficacy in this setting, current guidelines support the use of AIs as adjuvant therapy [26–30].
Management of aromatase inhibitor-associated bone loss in patients with breast cancer
Early diagnosis and treatment of AIBL are essential for effectively reducing the risk of fracture in patients with breast cancer. As bone loss may be asymptomatic until a fracture occurs, the American Society of Clinical Oncology has developed strategies to manage AIBL through monitoring of BMD. These guidelines stress the importance of early diagnosis and recommend baseline and regular screening of BMD by radiography and dual-energy x-ray absorptiometry in patients who are at high risk for bone loss. BMD measurements are typically defined against a standard value, and the WHO defines osteoporosis as a loss in BMD of greater than 2.5 standard deviations (SD) below the mean value of healthy 30-year-old adults and osteopenia as a BMD of between 1 and 2.5 SD below the mean (
Bone mineral density diagnostic categories.
SD: Standard deviation from young adult mean. Data from World Health Organization [32].
Diet, exercise and appropriate vitamin intake are important factors in the prevention of bone loss. Daily supplements of 500 mg calcium and 700 units vitamin D are beneficial in preventing osteoporotic fractures in elderly women and may slow the development of osteoporosis in women over 65 years of age [33]. Combined calcium and vitamin D supplements have also been shown to reduce the number of femoral neck fractures in elderly women [34]. However, because bone loss is especially rapid in patients with cancer, bone-directed therapies may be necessary.
Bisphosphonates can prevent therapy-associated bone loss in patients with breast cancer
Currently, there are no treatments specifically approved for cancer treatment-associated bone loss. Several studies have examined the use of bisphosphonates in this setting (
Summary of clinical studies for the prevention of bone loss in breast cancer.
Patients in the BMD protocol only.
BMD: Bone mineral density; DOC: Docetaxel; iv.: Intravenous.
In premenopausal women with early-stage breast cancer, small studies with oral bisphosphonates suggest that, compared with placebo, daily oral clodronate or risedronate can prevent bone loss in women with chemotherapy-induced menopause [17,35]. In a study investigating the efficacy of oral clodronate (1600 mg/day) in the prevention of bone loss in premenopausal patients with breast cancer (n = 148) who were receiving adjuvant chemotherapy, clodronate significantly reduced the risk of bone loss (p < 0.05) [35]. In a similar study in breast cancer patients with chemotherapy-induced premature menopause (n = 52), oral risedronate (30 mg/day) effectively prevented trabecular and cortical bone loss [37]. However, in clinical practice, compliance and persistency with oral bisphosphonates have been low, and this may impair efficacy. A recent report of intravenous clodronate (1500 mg for seven cycles) failed to demonstrate a significant preservation of BMD compared with placebo in 45 premenopausal women during treatment with agents that induce premature menopause [36]. There are no published studies on the use of ibandronate in the AIBL setting; however, ibandronate does prevent bone loss in recently postmenopausal healthy women [39].
Zoledronic acid has demonstrated broad clinical utility for the treatment of malignant bone disease and clinical efficacy in the prevention of cancer treatment-associated bone loss. Results of a bone subprotocol (n = 401) of the ongoing Austrian Breast and Colorectal Cancer Study Group 12 (ABCSG 12) trial demonstrated that zoledronic acid effectively and safely prevents AIBL in premenopausal women receiving adjuvant endocrine treatment with goserelin plus anastrozole or goserelin plus tamoxifen. Bone loss was 14.4% at 3 years in patients who were not treated with zoledronic acid, whereas no bone loss was experienced by patients treated with zoledronic acid [38]. Moreover, zoledronic acid (4 mg every 6 months) completely prevented the bone loss in the trochanter and lumbar spine normally induced by tamoxifen or anastrozole in combination with goserelin across 36 months of treatment (p < 0.0001 compared with patients who did not receive zoledronic acid).
The Z-FAST study investigated the effect of immediate versus delayed administration of zoledronic acid for the maintenance of bone health in postmenopausal women with hormone receptor-positive (ER+ or progesterone-receptor-positive) breast cancer receiving the AI letrozole (2.5 mg/day) [16]. Patients were randomized to receive either upfront zoledronic acid or delayed zoledronic acid when their T-scores decreased to less than −2 SD or upon experiencing a fracture. At 12 months, lumbar spine BMD increased by a mean of 2.02% in the upfront zoledronic acid group but decreased by a mean of 2.61% in the delayed group, which was a significant difference of 4.63% between groups (p < 0.001; Figure 1). Similarly, the upfront zoledronic acid group experienced a mean increase of 1.40% of total hip BMD, but there was a decrease of 2.10% in the delayed treatment group (p < 0.001). Analyses of serum markers of bone turnover indicated that N-telopeptide and bone-specific alkaline phosphatase levels were significantly decreased in patients receiving upfront compared with delayed zoledronic acid (p < 0.0001 for both). The 1-year results of this trial demonstrate the benefits of upfront treatment with zoledronic acid compared with symptomatic treatment in the prevention of AIBL in postmenopausal women receiving adjuvant letrozole treatment.
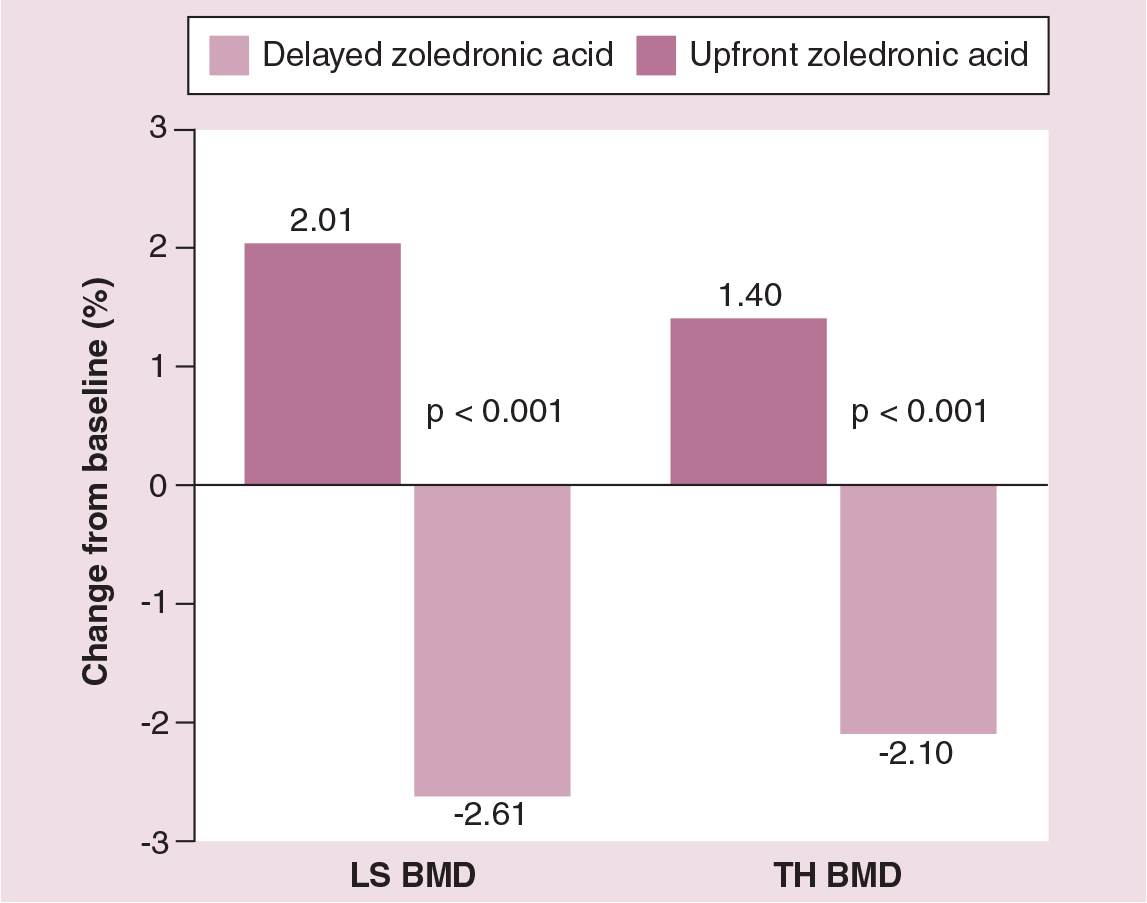
Z-FAST: difference in the percent change in lumbar spine and total hip bone mineral density in letrozole-treated, postmenopausal women with breast cancer randomized to upfront or delayed zoledronic acid treatment.
A similar trial (ZO-FAST) investigating upfront and delayed zoledronic acid in post-menopausal patients or patients with chemotherapy-induced premature menopause in Europe is ongoing, and results are anticipated in 2007 [40].
Estrogen-based therapies have been used in the osteoporosis setting; however, these may be contraindicated in patients with ER+ breast cancer. Raloxifene, which is approved for the treatment and prevention of osteoporosis in postmenopausal women [41], was investigated versus tamoxifen for the prevention of breast cancer in postmenopausal women [42]. Raloxifene was found to be as effective as tamoxifen in reducing the risk of developing invasive breast cancer, but was associated with an increased risk of developing noninvasive breast cancer. Tamoxifen provides modest protection against bone loss and fractures in post-menopausal women; however, it is not approved for bone loss.
Conclusion
The efficacy of AIs in the adjuvant setting for breast cancer is contributing to their emergence as a treatment of choice. However, patients with breast cancer receiving adjuvant therapies, especially AI-based regimens, are at risk for accelerated bone loss, which is typically higher than the bone loss associated with natural menopause. Bone loss results in significant decreases in BMD and subsequently increases the risk for fractures and spinal cord compression. Moreover, patients may incur greater hospital expenses and experience a decline in quality of life because of a loss of autonomy.
Early detection and treatment of bone loss are critical to prevent fractures and preserve a patient's quality of life, and bisphosphonates have demonstrated efficacy in this setting. Although patients have differing rates of bone metabolism, biochemical markers of bone metabolism may also be of use in monitoring or even scheduling the treatment of bone loss. Future studies will provide insights into optimized treatment strategies.
Future perspective
Oncology professionals have historically focused on treatment of the primary cancer. However, with increases in survival, oncologists must now consider the cumulative effects of therapy on their patients' long-term health. One such area where significant improvements can be offered is in the maintenance of bone health in women undergoing treatment for breast cancer. In this setting, bisphosphonates have demonstrated significant efficacy for the prevention of AIBL. Currently, many physicians might not detect the accelerated bone loss associated with cancer therapies unless their patients first develop a fracture. However, preservation of BMD during AI therapy could lower the incidence of fractures, and physicians should be encouraged to take a more proactive approach to maintaining bone health during AI therapy. To ensure adequate prevention and intervention strategies, physicians must recognize the importance of regular BMD screening to detect bone loss in women undergoing treatment for breast cancer. Indeed, regular BMD screening is supported by the guidelines of the American Society of Clinical Oncology [17]. Furthermore, as breast cancer treatments continue to improve survival, regular BMD screens will become a critical component of patient monitoring and follow-up.
Both oral and intravenous bisphosphonates have demonstrated clinical utility in the treatment of postmenopausal bone loss. However, AIBL appears to be more aggressive than post-menopausal osteoporosis, and a more active treatment may be needed. Zoledronic acid effectively blocks AIBL in both pre- and post-menopausal patients, as demonstrated in large randomized, controlled clinical trials, and this agent is currently being considered for regulatory approval in this setting. Ongoing clinical trials, such as CALGB-79809, will further define the role of bisphosphonates during treatment for breast cancer [101].
Executive summary
Chemotherapy and hormonal therapy have been linked to accelerated rates of bone loss in women with breast cancer.
Increased bone loss is associated with increased fracture risk.
The superior efficacy of aromatase inhibitors (AIs) compared with tamoxifen is leading to increased AI use in the adjuvant setting for breast cancer.
Bone loss associated with AIs is more rapid than that reported during menopause.
The American Society of Clinical Oncology has developed strategies to manage bone loss through monitoring of bone mineral density.
Diet, exercise and appropriate vitamin intake are important factors in the prevention of bone loss, but may not be sufficient for the prevention of AI-associated bone loss.
Bone-directed therapies may be necessary to maintain skeletal health in patients undergoing endocrine therapy.
Goals of therapy are to prevent bone mineral density loss before patients develop fractures during long-term endocrine treatment, thereby preserving the patient's quality of life throughout the continuum of care.
Bisphosphonates are effective inhibitors of osteoclast-mediated bone loss.
Upfront concomitant therapy with zoledronic acid prevents bone loss and optimizes therapy in patients receiving AIs.
Due to advances in screening, diagnosis and treatment, patients with breast cancer are surviving long enough for the skeletal effects of cancer treatments to manifest in fractures.
A more proactive approach to maintaining bone health during AI therapy should be encouraged through regular bone mineral density screening.
Zoledronic acid effectively blocks AI-associated bone loss in both pre- and post-menopausal patients and is currently being considered for regulatory approval in this setting in Europe (EMEA) and in the USA (FDA).
Footnotes
Dr Lipton has received speaking honoraria and is a consultant on bisphosphonates for Novartis Pharmaceuticals. Dr Gnant has no information to disclose. Dr Aapro has conducted studies and is a consultant on bisphosphonates for Novartis Pharmaceuticals and Roche AG.
Financial support for medical editorial assistance was provided by Novartis Pharmaceuticals. We would like to thank Carol Sledz, PhD, at ProEd Communications, Inc.® for her medical editorial assistance.