
Abstract
Chronic diseases present a growing challenge to women's health. This paper presents data from the Australian Longitudinal Study on Women's Health to show prevalence and incidence among three cohorts of women of six chronic conditions: hypertension, heart disease, diabetes, asthma, osteoporosis and arthritis. It also examines the role of five important risk factors (body mass index, level of physical activity, smoking, alcohol consumption and level of education) on these chronic conditions. The most striking finding is that being overweight or obese is the most important risk factor for chronic disease for women in all three age groups.
Keywords
Chronic diseases such as heart disease, hypertension and diabetes contribute to a growing burden on the health of individuals and families, and on healthcare systems worldwide. From an estimated 58 million deaths worldwide in 2005, chronic diseases accounted for 35 million. It has been estimated that a focus on prevention and control of chronic diseases would prevent 36 million deaths by 2015 [1]. This paper presents data on chronic conditions from the Australian Longitudinal Study on Women's Health (ALSWH). The study is designed to run until at least 2016 and the 40,000 participants have now been resurveyed at least three times over the past 10 years, providing a large amount of data on the women's lifestyles and health outcomes. Three cohorts of women are surveyed: younger women who were aged 18–23 years in 1996, mid-aged women who were aged 45–50 years, and older women, aged 70–75 years.
The three cohorts of women in the ALSWH provide an opportunity to explore health at three critical stages in women's lives. Current models of health promotion emphasize that health promotion needs to start at conception and continue across the life course [2]. In early life, the emphasis is on building resources that affect adult capacity, such as education, good nutrition, physical activity and healthy weight. For younger and mid-aged adults the emphasis is on minimizing health risks by avoiding damage (such as from smoking and alcohol, or through hypertension or high cholesterol), and on reducing loss of health (for example, through good nutrition and by maintaining physical and mental activity). At older ages, the emphasis is on minimizing the impact of disease through good management of chronic conditions, protection against injury and other stressors, and physical and social support.
In this paper we focus on six chronic conditions: hypertension, heart disease, diabetes, asthma, osteoporosis and arthritis. We examine the prevalence and incidence of each condition among three cohorts of Australian women. We also examine the risk factors that are associated with these conditions. Finally we consider the long-term effects that trends in the risk factors are likely to have on women's health.
Method
Study design
Background
The ALSWH is a broad-ranging project examining relationships between many biological, physiological, social and lifestyle factors and women's physical health, emotional well-being, and use of and satisfaction with health services. It is funded by the Australian Government Department of Health and Aging and involves three age groups of women who were first surveyed in 1996 and will be followed-up for at least 20 years. In 1996 women in the younger sample were aged 18–23 years, the mid-aged women were aged 45–50 years, and the older women were aged 70–75 years. Women were selected from the Australian national health insurance database (Medicare), which includes all citizens and permanent residents. Stratified random sampling was used to select the sample with systematic oversampling of women from rural and remote areas. Table 1 provides an overview of the schedule of surveys. The sample is generally demographically representative of the Australian population of women [3]. Despite intensive follow-up and participant tracking, loss of participants has occurred, particularly among the younger women who were highly mobile in the early years of the study, and the older women, more of whom die or become too ill to complete the survey as they age. Details of the sample, recruitment methods and attrition have been described elsewhere [3,4] and further information, including copies of surveys and data books, is available online [101].
Schedule of surveys for the Australia Longitudinal Study on Women's Health.
Measures & analysis
Prevalence & incidence
At each survey, women were asked about diagnosed medical conditions. In earlier surveys the question was framed as “Have you ever been told by a doctor that you have…?”. However, in later surveys, the question was revised to: “In the past three years have you been diagnosed or treated for…?”. Prevalence and incidence calculations assumed that the conditions of interest were enduring.
The prevalence of each of the six conditions at Survey 1 was calculated as the number of women who indicated that they had been told by a doctor that they had each condition (the numerator), divided by the total number of women who provided any information about the condition (the denominator) multiplied by 100 (to give prevalence per 100 women). Women who did not provide information at Survey 1, but who subsequently reported not having the condition, could be considered to be free of the condition at Survey 1 and so were included in the denominator.
For the purposes of this analysis, incidence was defined by new cases of conditions that emerged since the women were first surveyed in 1996. Thus a woman who did not have diabetes at Survey 1 but reported the disease at Survey 2 or at subsequent surveys would be defined as a new case. The number of women without the condition at Survey 1 formed the denominator and the incidence rate was calculated as number of new cases per 100 women per year by dividing the number of new cases by the denominator then multiplying by 100 and dividing by the number of years between surveys.
Risk factors
Risk factor levels were categorized as follows. Body mass index (BMI) (self-reported weight in kg divided by the square of self-reported height in meters) was categorized as underweight (≤ 18.5), healthy weight (18.5 to ≤ 25), overweight (25 < BMI ≤ 30) or obese (BMI > 30). A high BMI refers to the overweight and obese categories. Level of physical activity was calculated as estimated units of energy expenditure and categorized as nil/low or moderate/high [5]. Smoking was categorized according to whether women had never smoked, were ex-smokers or were current smokers. Alcohol consumption was categorized into three groups: nondrinkers, low/occasional drinkers and high-risk drinkers. The nondrinkers may have included both lifetime abstainers and ex-drinkers. Education was categorized according to whether or not the women had any post-high school qualifications.
Data are presented from the first three surveys for the younger cohort and from the first four surveys for the mid-aged and older cohorts. The analysis of incidence compared women who had developed disease since 1996 with women who had never had the disease. The analysis of prevalence compared existing cases at Survey 1 with women who did not have the disease at Survey 1. The data analysis for this paper was generated using SAS software, Version 9 of the SAS System for Windows (©2002–2003 SAS Institute Inc. SAS and all other SAS Institute Inc. products or service names are registered trademarks or trademarks of SAS Institute Inc., NC, USA). The analysis examined the associations between risk factor levels at Survey 1 and prevalence and incidence of each chronic disease. Relative risk estimates and 95% confidence intervals were calculated using Poisson regression for all risk factor/chronic condition combinations.
Results
Prevalence of chronic conditions
The prevalence and incidence figures for each chronic condition examined are shown in Table 2. Asthma was the most common condition among the younger women, with arthritis and hypertension the most common among mid-aged and older women. Hypertension, heart disease and diabetes showed similar trends across the cohorts, with very low prevalence and incidence among the younger women but higher prevalence in the mid-aged and older cohorts.
Prevalence (at Survey 1) per 100 women and incidence per 100 women per year of conditions for the younger, mid-aged and older cohort.
Incidence/100/year was calculated over 7 years for the younger cohort, 8 years for the mid-aged cohort and 9 years for the older cohort.
Incidence/100/year was calculated over 3 years for the mid-aged cohort (Survey 3 to 4) and 6 years for the older cohort (Survey 2 to 4). NA indicates condition was not included in surveys for this cohort. Figures are rounded to the nearest whole number, or to the nearest first or second decimal place where values less than 1 or 0.1.
Younger women were not asked about osteoporosis and arthritis, but there was an increase in the prevalence and incidence of these conditions between mid-aged and older women. Asthma was the only disease for which younger women reported higher prevalence and incidence than mid-aged and older women.
Risk factors in each cohort
Table 3 shows the prevalence of risk factors for each cohort at Survey 1. The proportion of women who were overweight or obese was lowest among the younger cohort, with over 10% underweight. Only a small proportion of mid-aged and older women were underweight, around half were a healthy weight and the remaining women were overweight or obese. Moderate or high rates of physical activity were most common among the younger cohort, less common among mid-aged women, and the older cohort were the least active. Almost a third (31.9%) of younger women were current smokers compared with only 7.6% of older women. Conversely, 33.8% of older women, were nondrinkers in comparison with 9.3% of younger women.
Prevalence (at Survey 1) of risk factors for the younger, mid-aged and older cohorts.
Associations between chronic conditions and risk factors
Younger women
Table 4 summarizes the associations between prevalence and incidence of chronic conditions and risk factors for the younger women in the study. Risk factors for heart disease in younger women were not examined due to the low prevalence, and this cohort was not asked about osteoporosis or arthritis. BMI was the most important risk factor in this cohort. Compared with younger women of normal weight, those who were overweight were at higher risk of hypertension, diabetes and asthma.
Relative risk estimates (and 95% confidence intervals) for chronic conditions from Surveys 1–3 and risk factor levels at Survey 1 for the Younger cohort of the Australian Longitudinal Study of Women's Health.
Values in bold indicate statistical significance as the confidence interval does not include unity and where RR > 1.20 or RR < 0.8.
RR: Relative risk
Younger women with lower levels of physical activity were at higher risk of diabetes, but level of physical activity was not related to the risk of any of the chronic conditions among the younger women (possibly due to inadequacies of the measure used [5]). Younger women who were smokers (either current smokers or ex-smokers) were more likely to have hypertension and asthma. However, over time the proportion of smokers in this cohort decreased, with 23% smoking at survey 3 compared with 28% at survey 1. Younger women who did not drink alcohol were less likely to report hypertension and asthma. New cases of hypertension and asthma were more likely among women with lower levels of education.
Mid-aged women
Table 5 shows that being overweight or obese was associated with hypertension, heart disease, diabetes, asthma and arthritis among mid-aged women. Lack of physical activity was an important risk factor for hypertension, heart disease, diabetes, asthma and incidence of osteoporosis. Activity levels increased among the mid-aged women across surveys. At Survey 3, 46% of the women were engaged in moderate or high levels of physical activity and the most common activity was walking. However, 16% of mid-aged women did no physical activity other than house or yard work and this may not be enough to protect against chronic disease [6].
Relative risk estimates (and 95% confidence intervals) for chronic conditions from Surveys 1–3 and risk factor levels at Survey 1 for the mid-aged cohort of the Australian Longitudinal Study of Women's Health.
Values in bold indicate statistical significance as the confidence interval does not include unity and where RR > 1.20 or RR < 0.8.
BMI: Body mass index; RR: Relative risk.
Compared with nonsmokers, current mid-aged smokers were more likely to have heart disease and arthritis, and to develop asthma. Ex-smokers were at higher risk of developing asthma. Of mid-aged women, 13% were smokers and there were few changes in smoking over time. Nondrinkers and high-risk drinkers were more likely to have hypertension, and nondrinkers were more likely to have diabetes, heart disease and osteoporosis. A lower education level was associated with higher incidence and prevalence of diabetes, and prevalence (but not incidence) of hypertension, heart disease, osteoporosis and arthritis.
Older women
Table 6 shows that women who were overweight or obese were at higher risk of all the conditions except osteoporosis, for which higher BMI was protective. Low levels of physical activity were associated with prevalence of heart disease, diabetes, asthma and arthritis, and incidence of diabetes and arthritis. Levels of physical activity decreased as the women aged. At Survey 3, 54.6% of the younger women were considered ‘active’ compared with 45.5% of the mid-aged women and only 34.1% of the older women. Current and ex-smokers were at higher risk of osteoporosis, and ex-smokers were at higher risk of asthma. Current smokers were at less risk of hypertension and heart disease. This finding could be influenced by earlier deaths among smokers, and also because women with chronic conditions may have been more likely to have quit. Prevalence of heart disease and diabetes was higher among older women who were nondrinkers. Risky drinkers had higher incidence of asthma. Those with lower levels of education had higher rates of diabetes.
Relative risk estimates (and 95% confidence intervals) for chronic conditions from surveys 1–3 and risk factor levels at survey 1 for the older cohort of the Australian Longitudinal study of women's Health.
Values in bold indicate statistical significance as the confidence interval does not include unity and where RR > 1.20 or RR < 0.8.
BMI: Body mass index; RR: Relative risk.
Women's weight over time
As BMI was found to be the most important risk factor for all the chronic conditions examined in these analyses, further investigation was made regarding trends over time. Figure 1A shows the average weight in kilograms and Figure 1B shows the BMI for each cohort for each survey. The mid-aged cohort had the highest average weight of 67.8 kg at survey 1 compared with the older women (average weight 65.6 kg) and the younger women had the lowest average weight (62.2 kg). However, over time, younger women have gained weight more rapidly, averaging 733 g gain per year, in comparison with mid-aged women who gained an average of 300 g per year. If this trend continues, the younger women's average weight will greatly exceed that of the mid-aged women. In fact, the younger women at Survey 3 (aged 25–30 years) were already approaching the average weight of 67.8 kg of the mid-aged women aged 45–50 years at Survey 1, and 3 years later at Survey 4 younger women are heavier on average than mid-aged women at Survey 1. The pattern of weight gain is reflected in changes in BMI over time, except in the older cohort where average BMI remained largely unchanged over time, reflecting decreases in both height and weight. It should be considered that BMI was calculated using self-reported height and weight, and therefore women might have underestimated their weight, especially as they are gaining weight actively.
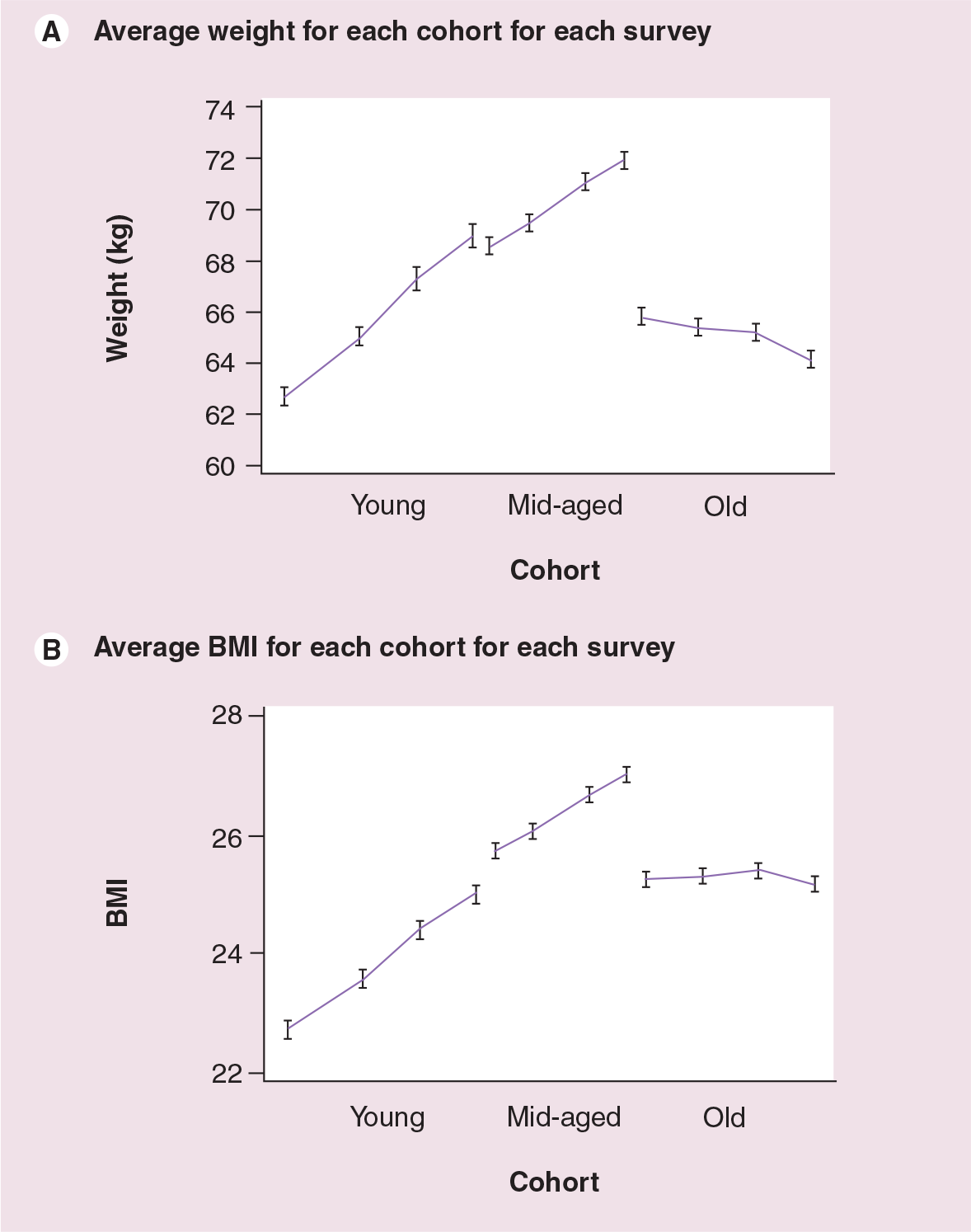
Average weight and average BMI for each cohort for each survey.
Conclusion
The most striking finding of these analyses is that being overweight or obese is the most important risk factor for chronic conditions in women at all ages. Women who are overweight are more likely to have hypertension, heart disease, diabetes, asthma and arthritis. In comparison, none of the other risk factors showed such consistent and strong associations with chronic conditions. For example, while higher levels of physical activity were generally protective (possibly by moderating the effects of weight) the direction of causation was sometimes unclear, with the onset of chronic conditions such as arthritis potentially limiting physical activity.
The most common among the chronic conditions examined in this paper was hypertension, which is important in terms of cardiovascular disease. Heart disease increased markedly among mid-aged women. Arthritis was the second most common condition. While diabetes, asthma and osteoporosis were less common, they were still important causes of morbidity. All conditions increased across cohorts and across time, except for asthma, which had the highest prevalence among the younger cohort and the lowest among the older cohort. One limitation of our study is that data are unconfirmed self reports of a diagnosis by a doctor. However, while some of the data may be unreliable, there is evidence that questionnaire data are of value in assessing chronic conditions [7,8]. Also, the data are unlikely to be systematically biased, except where other factors may affect diagnosis, such as clinical uncertainty regarding asthma in older people, or access to bone density testing, which forms the basis for a diagnosis of osteoporosis. Analyses of associations between risk factors and these conditions may be misleading due to these diagnostic issues.
The impact of socioeconomic status on women's health is demonstrated by the association between lower levels of education and risk of chronic conditions in later life, particularly evident among mid-aged women. However, level of education was not found to be as important as other risk factors overall. From a life course perspective, level of education is a more distant determinant of health than proximal factors such as BMI [2].
Smoking was most strongly associated with chronic conditions among mid-aged women and to some extent among younger women. Survivor effects may have affected the results for the older cohort, where women who smoked and had chronic conditions were least likely to remain in the study as time went on.
Future perspective
It is worrying that younger and mid-aged women are getting heavier. However, it is most concerning that if the trends of increasing weight continue among the younger women, weight will be an even greater problem for them in mid-age than for the current mid-aged women in the study. It is also concerning that these trends are evident so strongly in self-reported weight data, which are likely to significantly underestimate rates of overweight and obesity [9].
Australia is experiencing a growing epidemic of overweight and obesity [10]. Between 1980 and 1999–2000, the percentage of obese women rose from 8 to 20% and among men rose from 9 to 17% [11]. As a consequence, the prevalence of diabetes is rising [12], although morbidity and mortality from cardiovascular disease for men and women are still falling [13,14]. Weight gain clearly poses a major threat to the health of Australian men and women.
One of the original goals of the ALSWH was to monitor physical activity and weight [15]. The study is also well placed to provide population-level surveillance data on weight gain and its major determinants of energy intake and expenditure. Indeed, data from the most recent surveys of the mid-aged women indicate that walking is increasing and that there may be a decline in the rate of weight gain in this cohort. Many of the younger women, who are already gaining weight more rapidly than the mid-aged women, are now in their early thirties, when many are having babies. This increases their risk of further long-term weight gain, so their risk of future chronic disease is high unless there is a very substantial change in population behavior with respect to weight gain. The consequences of weight gain in terms of burden of chronic disease and costs of health services are the topics of ongoing work by ALSWH researchers.
Executive summary
Chronic conditions such as heart disease, hypertension and diabetes contribute to a growing burden on the health of women worldwide.
The Australian Longitudinal Study on Women's Health first surveyed 40,000 women in 1996 and now has a decade of longitudinal health data at three critical stages in women's lives.
The Study provides an ideal opportunity to examine trends in chronic conditions and the important risk factors that contribute to their development.
All conditions increased across cohorts, except for asthma, which had the highest prevalence among younger women and the lowest among older women.
Hypertension and arthritis were the most common conditions among mid-aged and older women.
Body mass index was the most important risk factor for all the chronic conditions examined, demonstrating that weight gain poses a major threat to the health of Australian women.
Further information about the Australian Longitudinal Study on Women's Health can be found at