
Abstract
Objective:
This article describes the women population and work at a unique Women’s Health Cardiology Clinic in order to raise cardiovascular disease awareness with an emphasis on women-specific risk factors, and thus to improve women’s clinical outcomes. This expectantly will aid in opening similar centers allowing more women to get superior care.
Methods:
Electronic medical records of women referred to the Women’s Health Cardiology Clinic were analyzed. The statistical analysis is descriptive in nature. Women’s Health Cardiology Clinic personnel work as a multidisciplinary team, and patients receive specialized diagnostic tests and treatments. Referrals are by physicians according to traditional and women’s specific risk factors for cardiovascular disease.
Results:
985 women visited the Women’s Health Cardiology Clinic, accumulating 2062 visits. Median age was 57.5 years. The majority of the women were menopausal (575 women, 58%), 62 pregnant with complications and 25 oncology patients. At least, 30% of women had diabetes/hypertension/or dyslipidemia. 72 women had a history of either cerebrovascular event or acute coronary syndrome, and 139 women had evidence of atherosclerosis. Overall, 388 women underwent endothelial function test, 40% of these women had a score indicating endothelial dysfunction. 277 women underwent a psychological intervention.
Conclusion:
Described here are the experiences from a multidisciplinary Women’s Health Cardiology Clinic using a gender-specific cardiovascular care approach for women geared toward improved health and wellbeing. It is of utmost importance that this report will raise women-specific cardiovascular disease risk factors awareness in order to promote women’s cardiovascular and overall health.
Introduction
According to the World Health Organization, cardiovascular disease (CVD) is the number one cause of death globally, more people die annually from CVD than from any other cause. The Centers for Disease Control and Prevention (CDC) database reveals that it is the leading cause of death for men and women in the United States causing one death every 36 seconds from CVD. Although mortality is similar between men and women, 1 we cannot relate to them the same as gender and sex matter to the heart.
Well-established data show differences in the pathophysiology, clinical presentation, and diagnosis of CVD in women compared to men. Furthermore, these disparities are even more robust when considering ischemic heart disease (IHD) syndromes. 2 In fact, IHD is the most substantial cause of CVD mortality in women worldwide. 3 Specifically, in acute coronary syndrome (ACS), female gender has been associated with worse clinical outcomes. 4 Unfortunately, in young women, the incidence of ACS continues to rise largely because of the increased prevalence of comorbidities. 5 The women’s health initiative was first to change the practice of CVD in women, by increasing the global awareness of women to their cardiovascular risk status and improving their clinical management. 6 Nonetheless, awareness and education of women-specific aspects of IHD and risk factors are lacking, and these important aspects are still understudied. 7
Most of the burden of CVD can be explained by traditional risk factors that affect both men and women, including elevated blood pressure, smoking, obesity, diabetes mellitus (DM) and dyslipidemia. These risk factors generally overlap among genders, yet studies have shown that DM and smoking have a worse impact in women. 6 Beyond these traditional risk factors, risk factors specific to women, such as adverse pregnancy outcomes, menopausal transition, history of breast cancer, and psychological aspects are under recognized.
Women experiencing adverse pregnancy outcomes have been shown to have early manifestations of vascular changes and endothelial dysfunction. 8 Studies have consistently shown an association between a history of pregnancy complications, including hypertensive disorders of pregnancy, gestational diabetes, stillbirth, preterm birth, placental abruption, and intrauterine growth restriction and subsequent CVD in women. 9
Postmenopausal women show distinct patterns of sex hormone changes, as well as adverse alterations in body composition, lipids and lipoproteins, and measures of vascular health, all can increase a woman’s risk of developing CVD. 10 In 2018, the American Heart Association and the American College of Obstetricians and Gynecologists issued a joint call to action urging clinicians in both specialties to team up to identify women at risk using gender-specific risk information, in a manner that will bridge disciplines.
Breast cancer is the leading cause of cancer in women. Increasing survival of women with breast cancer has led to the emergence of CVD as a major cause of morbidity and mortality in survivors. 11 Although robust data relate sex-specific risk variables related to hormonal and reproductive status to CVD risk, the weight of these variables remains to be elucidated. 3 However, there is wide agreement that CVD risk assessment in women without including enhancing women’s specific risks factors lead to underestimation of future CVD risk. 12
Evidence gained from the WISE (Women’s Ischemic Syndrome Evaluation) study indicates that the full spectrum of IHD in women extends beyond atherosclerotic stenosis of the coronary arteries to dysfunction of the coronary microvasculature and endothelium. 13 In addition, endothelial dysfunction known as an early manifestation of atherosclerosis is a significant independent risk factor for IHD events, particularly in women.14–16
Awareness of women-specific risk factors and the need to change their impact on CVD outcomes, as well as sex differences in CVD manifestations, have raised the need for women’s specific cardiac health centers which have been emerging in the United States and Europe since 1990 in both private and academic medical centers. 17
In our medical center, we opened a multidisciplinary holistic Women’s Health Cardiology Clinic (WHCC) in 2014, with a vision to collaborate with family physicians, gynecologists, breast cancer oncologists, psychologists, and naturally cardiologists (Figure 1). The clinical team offers centered diagnosis and treatment in women’s specific cardiac health issues, by putting an emphasis on detecting risk factors that are both general and distinctive to each patient. By establishing gyneco-cadriology and onco-cardiology collaboration, the WHCC translates these gaps in risk assessment of CVD to action items.
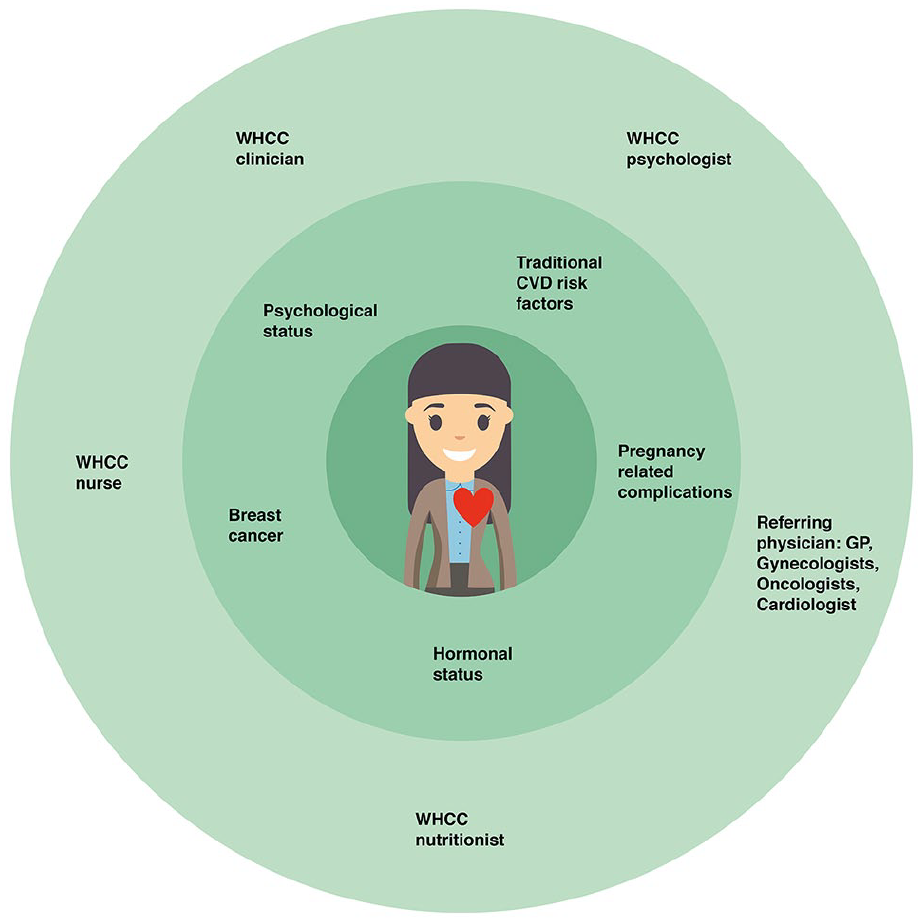
A unique multidisciplinary Women’s Health Cardiology Clinic using a holistic, centered diagnosis, and treatment approach according to women-specific cardiovascular care with emphasis on traditional and women-specific risk factors.
Our aim is to raise CVD awareness with an emphasis on women-specific risk factors. By capturing relatively young women who have not yet developed CVD, we can improve women’s clinical outcomes. This expectantly will also aid in opening similar centers allowing more women to get superior care.
Methods
Design
A regional campaign was initiated for women’s referral to the WHCC according to robust data regarding women’s specific risk factors, we directed physicians to refer women with multiple risk factors for CVD, menopausal symptoms with need for hormonal replacement treatment (HRT) consideration, chest pain syndromes, myocardial injury with and without obstructive coronary artery disease, high-risk pregnant woman mainly who suffered from hypertensive disorder of pregnancy (HDP) and/or gestational diabetes mellitus (GDM), and women with active or past history of breast cancer.
Setting
The WHCC is an integral part of the cardiology division in the Rabin Medical Center, one of the largest and leading tertiary medical complexes in Israel affiliated with the Faculty of Medicine at Tel Aviv University.
The personnel work as a multidisciplinary team composed of a cardiologist, nurse, medical psychologist, nutritionist, and social worker all trained in the field of women’s cardiology and health. Also, we collaborate with specialist doctors according to specific needs. Women receive specialized diagnostic tests and treatments within the setting of the center, providing the women with professional care that is holistic and nurturing.
Data collection
Electronic medical records of all women referred to the WHCC were analyzed, starting in January 2014 through December 2018. Collected data included demographic details, referral reasons, medical history including traditional and women’s specific risk factors, medication and physical activity level (categorized at the time of visit as: none, light, or vigorous). Existence of atherosclerotic disease was based on findings from coronary angiography, computerized coronary tomography, or Doppler ultrasound of carotid arteries.
One of the diagnostic tests that the WHCC implemented is a non-invasive test to assess endothelial function test (EFT) using peripheral arterial tonometry (PAT) signals using the EndoPAT device (Itamar Medical Inc., Caesarea, Israel). 18 The usage of the EndoPAT device (in addition to conventional cardiac imaging tests as needed and/or indicated) provides non-invasive, automatic, and quantitative evaluation of endothelial dysfunction by providing a reactive hyperemia index (RHI) score. 18 The cut-off value 1.67 was used, determined in previous studies, to diagnose endothelial dysfunction. 19
Women were referred to EFT, nutritional consultation, and psychological intervention according to clinical judgment and women’s personal preference. A protocol was built offering referred women 1–3 nutritional consultations and 1–12 psychological interventions.
Data analysis
The statistical analysis was generated using SAS Software, Version 9.4. The analysis was descriptive in nature; no hypotheses were tested, and thus, no p-values are presented. Mean value ± standard deviation presented continuous variables for symmetrical measures and median (interquartile range (IQR)) for skewed measures. Categorical variables are presented by N (%).
Ethical considerations
Data collection was approved by the Rabin Medical Center ethics committee in compliance with the Declaration of Helsinki (approval no. 0678-14-RMC), with a waiver for the need of individual informed consent in this registry-based, non-interventional study.
Results
Between January 2014 and December 2018, 985 women visited the WHCC. There were 2062 visits (an average of two visits per woman). The women’s median age at first visit was 57.5 years (Q1 = 44 and Q3 = 66). The baseline characteristics including risk factors, medications, and hormonal status are summarized in Table 1. Main referral reasons included personal initiative (37%), referral from within the hospital (17%), pregnancy-related complications (18%), oncology-related (11%), and referral by treating physician (10%). Seventy-two women (7%) had a history of either cerebrovascular event or ACS, and 139 women (14%) had evidence of atherosclerosis established by imaging or angiography. Overall, 388 (39%) of all women visiting the WHCC underwent EFT, and 40% of these women had an RHI <1.67 indicating endothelial dysfunction measures.
Baseline characteristics of WHCC patients and their cardiovascular risk factors.

WHCC: Women’s Health Cardiology Clinic; CVD: cardiovascular disease; CVA: cerebral vascular accident; TIA: transient ischemic attack; HRT: hormone replacement therapy; RHI: reactive hyperemia index; ACEi: angiotensin converting enzyme inhibitor; ARBs: angiotensin II receptor blockers.
Data are presented as medians (25th, 75th quartiles) or as percentages, as appropriate.
Percentages are out of known numbers of each variable.
Established atherosclerosis according to angiography or imaging.
Within the women population, 62 (6%) were pregnant with complications at the time of visit (Table 2), median age was 33 years (Q1 = 29 and Q3 = 35.8), with GDM being the leading complication (61%) followed by pre-eclampsia (24%) and gestational hypertension (15%). Twenty-three (37%) of the pregnant women underwent an EFT, with a median RHI of 1.42. Of the women who underwent EFT, 82% of the pregnant women experienced endothelial dysfunction (RHI <1.67). The majority of the women in our cohort included 575 women (58%) who were menopausal (Table 3). Their median age at time of visit was 65 years (Q1 = 59 and Q3 = 70) and median menopausal age was 50 years, 11% used hormone replacement therapy and 8% suffered from vasomotor symptoms, and 67% of these women were not physically active. Moreover, 231 (40%) of the menopausal women underwent EFT with a median RHI of 1.93, of them 15% presented with endothelial dysfunction.
Baseline characteristics of pregnant women visiting the WHCC.

WHCC: Women’s Health Cardiology Clinic; CVD: cardiovascular disease; CVA: cerebral vascular accident; TIA: transient ischemic attack; RHI: reactive hyperemia index; ACEi: angiotensin converting enzyme inhibitor; ARBs: angiotensin II receptor blockers.
Data are presented as medians (25th, 75th quartiles) or as percentages, as appropriate.
Percentages are out of known numbers of each variable.
Established atherosclerosis according to angiography or imaging.
Baseline characteristics of menopausal women visiting the WHCC.

WHCC: Women’s Health Cardiology Clinic; CVD: cardiovascular disease; CVA: cerebral vascular accident; TIA: transient ischemic attack; HRT: hormone replacement therapy; RHI: reactive hyperemia index; ACEi: angiotensin converting enzyme inhibitor; ARBs: angiotensin II receptor blockers.
Data are presented as medians (25th, 75th quartiles) or as percentages, as appropriate.
Percentages are out of known numbers of each variable.
Established atherosclerosis according to angiography or imaging.
The latest subpopulation to be included comprises 25 women (3%) forming the active/postbreast cancer subpopulation (Table 4). Median age at time of visit was 64 years (Q1 = 54 and Q3 = 70), with a median of two visits per woman, and 23 (90%) of these women were menopausal. Fifteen (60%) of the women underwent EFT with a median RHI of 1.68. Of note, only seven women (28%) had an RHI lower than 1.67.
Baseline characteristics of women with active or past history of breast cancer visiting the WHCC.

WHCC: women’s health cardiology clinic; CVD: cardiovascular disease; CVA: cerebral vascular accident; TIA: transient ischemic attack; HRT: hormone replacement therapy; RHI: reactive hyperemia index; ACEi: angiotensin converting enzyme inhibitor; ARBs: angiotensin II receptor blockers.
Data are presented as medians (25th, 75th quartiles) or as percentages, as appropriate.
Percentages are out of known numbers of each variable.
Established atherosclerosis according to angiography or imaging.
Psychological intervention
About a third of the women were referred to the WHCC medical psychologist and 277 of them arrived to the first appointment and started a psychological assessment and intervention. The interventions focused on six different therapeutic themes: stress management, changing life habits, depression/anxiety, coping with medical procedures, coping with disease, and increasing self-care. It was the women’s, doctor’s, and psychologist’s subjective notion that the intervention was of pivotal importance.
Discussion
Women health initiatives have been growing worldwide. In cardiovascular medicine, risk stratification is of utmost importance in primary and secondary prevention. Women-specific risk factors, related to reproductive years, hormonal changes, breast cancer, and psychological status, are often not sufficiently embedded in the “standardized” cardiovascular evaluation. These risk factors impact women’s CVD outcomes, as well as lifetime risk stratification, diagnostic measurements, and management. We opened the WHCC with a vision that a distinctive integrative and multidisciplinary approach directed toward women at different stages and ages in life, and specific high-risk populations, can improve their CVD care and outcomes. The WHCC has been focusing on the following four major groups.
Women with gestational complications
Our WHCC cohort included 62 young women who suffered from HDP or GDM, yet were for the most part with no other medical history. We tested 37% of these women for EFT, of them 82% had an RHI score <1.67 indicating endothelial dysfunction.
History of GDM doubles the risk of developing DM in the following 4 months postpartum and remains a lifelong risk factor for chronic kidney disease (CKD) and DM. 13 These women also have at least 1.5 times greater risk of CVD compared to pregnant women who did not suffer from GDM. Women with a history of pre-eclampsia have a 3.6- to 6.1-fold greater risk of developing hypertension. 20 Given evidence supporting the association between pregnancy complications and later CVD, professional societies (American College of Obstetricians and Gynecologists and the American Heart Association) have included recommendations for long-term management of these women.21,22 Accordingly, incorporating the history of gestational complications and referral of those women to a WHCC can help in education and implementation of therapeutic lifestyle changes in these women throughout their lives. 20 By including these young women in the WHCC, we are able to start monitoring risk factor evaluation and modification, providing essential lifestyle education and early intervention whenever needed.
Menopausal period
The majority of women are postmenopause, of them 50% suffered from hypertension, 30% had DM, and 54% had dyslipidemia. 11% of the women were treated with HRT.
The postmenopausal state has been recognized as a stage of increasing CVD risk for women. 23 In healthy menopausal women, normal decline in endothelial function usually starts in the early stages of menopause; these women have over a threefold risk of developing atherosclerosis.16,24 It has been shown that vascular health in women is dependent on the hormonal status and therefore may be detected by EFT, 25 and this potentially could help with early risk stratification in order to appropriately manage this high-risk population. Evidence regarding HRT and CVD is still somewhat of a conundrum ever since the Women’s Health Initiative (WHI) study caused the usage of HRT to drop dramatically. Recent studies with an emphasis on the ELITE trial 26 and reanalysis of the WHI have shown that when the time of administration and age is appropriate, HRT could be very beneficial (e.g. the “timing hypothesis”). Women are undertreated for menopausal symptoms and many feel that clinicians do not recognize the impact of menopause symptoms on their quality of life. 27 Our WHCC is putting a great emphasis to get menopause management “back on track” by assuring to stay up-to-date on current evidence regarding menopause management and available treatment options as to ensure improved quality of life and CVD risk reduction in this population.
Women with non-obstructive coronary artery disease
14% of the women had established atherosclerosis according to angiography or imaging, and 40% of women who underwent EFT showed signs of endothelial dysfunction, which is known to be an early stage of atherosclerosis.
Chest pain or myocardial injury with non-significant findings on coronary angiography poses a diagnostic challenge. The prevalence of non-obstructive coronary artery disease (NOCAD) in patients undergoing coronary angiography for chest pain is up to 50%. Of them, over 60% have coronary microvascular dysfunction, this is especially important in women, and is related to endothelial dysfunction. The long-term prognosis is not benign, and it has been associated with an increase in adjusted mortality and higher risk of major adverse cardiovascular events. 28 Current data highlight the different pathophysiology of IHD in women. 75% of women with chest pain, evidence of ischemia in non-invasive evaluation, and NOCAD, have abnormal coronary reactivity.29,30 In line with that, we routinely combine the assessment of endothelial dysfunction in the evaluation of women in the WHCC.
Another example of unique women-specific IHD presentation is the Takotsubo syndrome, which occurs predominantly in postmenopausal women. 31 Despite increasing awareness and recognition, this syndrome still remains largely underdiagnosed, with a prognosis that is not benign. 32 Women with NOCAD or Takotsubo often have an atypical presentation and are therefore underdiagnosed. Moreover, compliance to lifestyle changes and medical treatment are usually suboptimal in these women. Thus, our belief is that care of these women should be centered in a WHCC and should also include psychological and stress management interventions.
Women with active or past history of breast cancer
This is the smallest subpopulation in our cohort comprising 25 women, as referrals of this subpopulation to the WHCC only began in 2017.
Breast cancer occurs mainly in women, and it is the leading malignancy among them. According to the American Cancer Society, breast cancer screening has decreased mortality significantly due to early detection and efficient treatment. 33 Therefore, most women with an early diagnosis of breast cancer have a good prognosis and can expect to survive the disease. Data show that breast cancer is more commonly diagnosed after the age of 50 years, and this group is more susceptible to CVD, which is a major cause of death in postmenopausal women. 34 Among survivors of local breast cancer, CVD is the leading cause of morbidity and mortality. Cancer treatment contributes to high CVD risk with secondary cardio-toxic and atheromatous effects. 34 As breast cancer constitutes an important women-specific risk factor, we believe that the integration of these women at the WHCC is of utmost importance in order to educate, monitor, and reduce their CVD risk.
Cardiac psychology
Depression and anxiety, both common in the aging women, negatively affect health and ones well-being. 35 It is well established that adjunctive psychological intervention improves psychological symptoms and reduces cardiac morbidity and potentially also mortality among patients with IHD. 36 Approximately, a third of the women underwent psychological intervention, reflecting the strong association between women, CVD, and medical psychology.
Limitations
Described here is a single-center experience, which may not be relevant to all.
Some of the women subpopulations are quite small and more women are needed for future research. Also data was collected from medical files, not all files had all the data regarding each patient, specifically data did not include EFTs in all women. CVD outcome was not explored in the women included.
Future research
Behavioral interventions can be used effectively to reduce adverse CVD profiles in women.
The number of randomized trials and observational studies including women after complicated pregnancies or during menopausal transition is remarkably limited. Therefore, definitive recommendations cannot be given, and future research is needed in order to use behavioral interventions as an effective tool to reduce CVD. As mentioned in the limitations, CVD outcome was not examined in this study and it would be of utmost importance to further research this.
Conclusion
Described here are our experiences from a multidisciplinary women’s health cardiac clinic using a holistic, gender-specific cardiovascular care approach. By collaborating with gynecologists, breast cancer oncologists, family physicians, medical psychologists, and cardiologists, we offer centered diagnosis and treatment for women, with emphasis on their unique risk factors and clinical presentation, geared toward improved health and overall well-being. We strongly believe that this unique approach will raise CVD awareness and improve women’s clinical outcomes.
Footnotes
Authors’ note
“All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.”
Author contributions
S.S.L. is the lead to the writing—original draft. T.B. provided support to the data curation. O.I.B.Z. provided support to the writing—review and editing. A.E. provided support to the writing—review and editing. T.S. is the lead to the formal analysis. I.H. provided support to the writing—review and editing. R.K. provided support to the writing—review and editing. A.P. is the lead to conceptualization and supervision, and is the lead to writing—original draft.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Data collection was approved by the Rabin Medical Center ethics committee in compliance with the Declaration of Helsinki (approval no. 0678-14-RMC), with a waiver for the need of individual informed consent in this registry-based, non-interventional study.
Funding
The author(s) received no financial support for the research or authorship, publication of this article was funded by the Rabin Medical Centers Cardiology fund.
Guarantor
A.P. is the guarantor of this study.