
Abstract
Ovarian cancer is the leading cause of death for all gynecologic malignancies in developed countries, largely owing to the late stage of diagnosis. Despite response to initial surgery and chemotherapy, more than 65% of patients will have recurrent or persistent diseases. Approximately 50% of patients with recurrent ovarian cancer are asymptomatic. Recurrences are often diagnosed using a combination of tests, including cancer antigen 125, computed tomography, magnetic resonance imaging and positron emission tomography scan. The most significant prognostic factor among women with recurrent ovarian cancer is the length of time from initial diagnosis to recurrence. Treatment of recurrent ovarian cancer involves chemotherapy, with or without surgery. In selected patients, secondary cytoreductive surgery might significantly improve survival. Radiotherapy may have a role in the treatment of a small group of patients with localized symptomatic masses. New treatment modalities for women with recurrent ovarian cancer are needed, as none of the available treatments are curative.
Ovarian cancer is the leading cause of death for all gynecologic malignancies in developed countries [1]. Worldwide, there are an estimated 166,000 new cases and 101,000 deaths annually from ovarian cancer [1]. At the time of diagnosis, only 36% of patients are diagnosed with stage I/II disease (23% stage I and 13% stage II), whereas 64% of patients present with advanced-stage disease (48% stage III and 16% stage IV) [1,2]. Despite aggressive treatment with cytoreductive surgery and combination platinum-based chemotherapy, 70–90% of patients with advanced-stage disease and 10–20% of patients with early stage disease will reoccur. In general, approximately 65% of patients diagnosed with ovarian cancer (regardless of stage) will have either recurrent or persistent disease following initial management.
Numerous attempts have been made to find the optimal chemotherapeutic, radiologic or surgical treatment modality for women with recurrent ovarian cancer. Numerous studies have demonstrated that the most important factors in predicting outcome following tumor recurrence are the patient's initial response to platinum-based therapy and the length of the disease-free interval prior to tumor recurrence. Patients are classified into three subsets according to sensitivity. Platinum-sensitive patients experience a recurrence of disease more than 6 months after discontinuation of therapy, platinum-resistant patients experience recurrence within 6 months of completion of primary therapy, and platinum-refractory patients have disease progression during primary treatment. In general, second-line chemotherapy among patients with recurrent ovarian cancer will lead to response rates of 50–60, 20–30 and 10% in platinum-sensitive, platinum-resistant and platinum-refractory patients, respectively [3].
Diagnosis of recurrent ovarian cancer
Patients with recurrent ovarian cancer may have symptoms related to the tumor recurrence or they may be asymptomatic. In the latter group, the diagnosis is often made based on routine follow-up of the tumor marker cancer antigen (CA) 125 and confirmed by imaging studies with or without biopsy. Symptoms attributable to recurrent ovarian cancer vary according to the site of recurrence and might include pelvic or abdominal pain, sense of pelvic pressure, abdominal distension, cough, shortness of breath, weight loss, leg edema or a mass that can be felt by the patient. On examination, the patient might have a pelvic or an abdominal mass(es), ascites, pleural effusion or enlargement of the axillary, supraclavicular or inguinal lymph nodes. Occasionally, patients with recurrent disease present with nausea and vomiting secondary to small-bowel obstruction, or increasing constipation secondary to colonic obstruction. In a study by Tay and colleagues, only 50% of the patients with recurrent ovarian cancer had symptoms [4].
The site of recurrent ovarian cancer can be local or distant. Local recurrence can either be a single pelvic or abdominal mass, or widespread intraperitoneal disease. Patients can experience tumor recurrence anywhere in the abdomen; the liver, spleen, kidneys, small and large bowel or diaphragm, for example. In addition, patients can experience distant disease, such as lung, brain or supraclavicular lymph node metastases.
CA 125 is commonly elevated in patients with recurrent ovarian cancer if elevated at initial diagnosis, and can be the first signal of such recurrence. However, as in the primary diagnosis of ovarian cancer, CA 125 could be normal among women diagnosed with recurrent ovarian cancer. Increases in CA 125 can be detected in 90% of patients before clinical evidence of disease recurrence. Rustin and colleagues demonstrated a lag of 63–99 days between CA 125 re-elevation and clinical evidence of disease recurrence [5].
Computed tomography (CT) is a commonly employed technique for diagnosing ovarian cancer recurrence, with a reported sensitivity of 40–93% for detecting recurrent disease [6]. Factors affecting CT accuracy include: tumor location and size, bowel preparation, associated or unrelated body changes and radiologist experience. Other factors affecting the use of CT include allergy to the intravenous contrast agent and inability to tolerate the oral contrast agent in patients with bowel obstruction. Patients with renal insufficiency can have deterioration of their renal function following the use of the intravenous contrast material. In one study, the limits of CT were especially evident in detecting peritoneal tumor deposits less than 2 cm in size, infiltrations of soft tissue between bowel loops and small pelvic masses [6]. On the other hand, liver and splenic metastases were easily detected by CT.
Magnetic resonance imaging (MRI) is believed to be equally accurate as CT for detecting ovarian cancer recurrence and has the advantage of avoiding the use of contrast material. However, except for the central nervous tissue, anatomic details are probably superior with CT compared with MRI. MRI is more advantageous for patients with a severe allergy to the intravenous contrast agent and those with renal insufficiency.
Positron emission tomography (PET) has been tested recently in conjunction with CT (combined PET/CT) for the detection of ovarian cancer recurrence. PET seeks to identify the uptake of 18F-flurodeoxyglucose (FDG) and has been shown to be successful in other solid tumors, such as colon cancer [7]. In a study by Nakamoto and colleagues, a PET scan confirmed disease recurrence in eight out of ten patients in one group, and demonstrated true positive in two out of 12 and true negative in eight out of 12 in another group of patients with recurrent ovarian cancer [7]. The sensitivity and specificity for detecting recurrence was 92.3 and 100%, respectively. In a smaller study, Makhija and colleagues were able to detect disease recurrence in 62% of patients using PET/CT, where CT scans alone were negative for disease [8]. Bristow and colleagues demonstrated a high sensitivity (83.3%) and a high positive predictive value (93.8%) for combined PET/CT in identifying potentially resectable macroscopic recurrent ovarian cancer among patients with biochemical evidence of recurrence and negative or equivocal conventional CT findings [9].
However, there are some inherent limitations of PET scans. First, chemotherapy has been noted to suppress FDG uptake and, as in the study by Nakamoto and colleagues, PET can therefore miss lesions as large as 3 cm [7]. Second, PET identifies FDG uptake, which can be seen in normal tissue, such as the alimentary and urinary tracts [7]. Finally, small foci of cancer may not have sufficient FDG uptake to register on PET scans.
Treatment of recurrent ovarian cancer
Factors affecting the treatment of recurrent ovarian cancer include: response to first-line therapy, interval from first-line therapy to disease recurrence, patient-performance status, associated comorbidities, the site and size of recurrence and patient wishes. The most commonly available treatment options include secondary cytoreductive surgery and chemotherapy, either in combination or individually. Radiotherapy and novel immune-modulated therapies have also been explored with limited success. A schema for the treatment of women with ovarian cancer is shown in Figure 1.
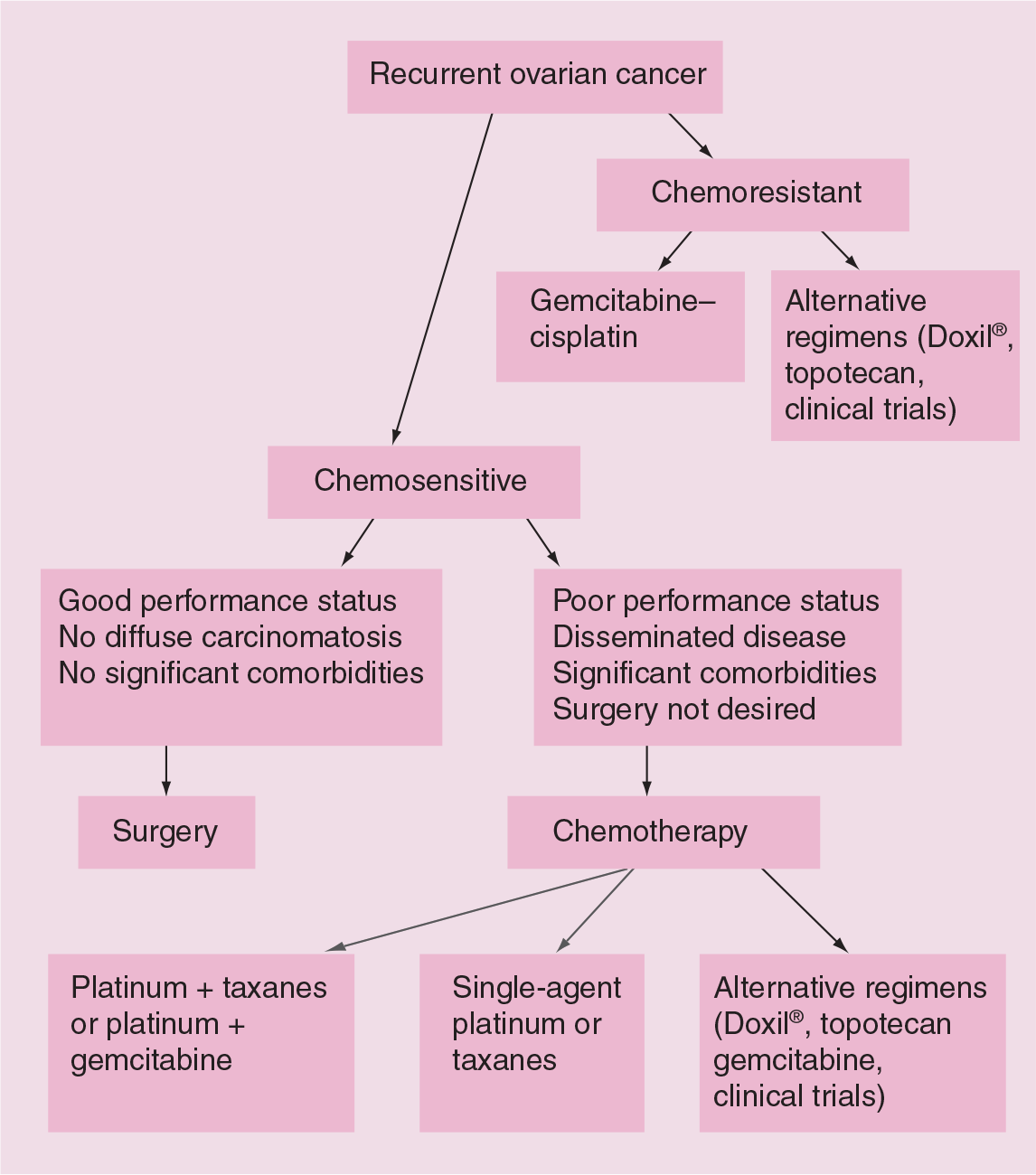
Schema of treatment of women with recurrent ovarian cancer.
Secondary cytoreductive surgery
The rationale for secondary cytoreductive surgery among women with recurrent ovarian cancer is reducing overall tumor burden, ameliorating symptoms, removing the poorly perfused/anoxic cells and reducing the number of tumor cells likely to undergo spontaneous mutations resulting in drug resistance [10]. There are different opinions concerning the treatment of recurrent ovarian cancer. For this reason, it is recommended that a gynecologist oncologist be involved in the formulation of any treatment plan.
Several retrospective and prospective studies have demonstrated a survival advantage for patients with recurrent ovarian cancer who underwent secondary cytoreductive surgery and had their tumor removed completely or cytoreduced to less than 2 cm, compared with women with recurrent ovarian cancer who did not undergo secondary cytoreductive surgery or in whom such surgery was unsuccessful in removing the bulk of the tumors [4,10–16]. Table 1 summarizes the studies that addressed secondary cytoreductive surgery among women with recurrent ovarian cancer.
Studies of secondary cytoreduction in recurrent ovarian cancer.
Statistically significant differences.
NA: Not available.
Following secondary cytoreductive surgery, most patients receive chemotherapy. However, patients occasionally receive no additional treatment or radiation therapy. Eisenkop and colleagues demonstrated that cytoreduction could increase the disease-free interval and maximize survival if secondary cytoreduction was undertaken prior to secondary chemotherapy [12]. The median survival for patients who received salvage chemotherapy prior to surgery was 15.8 months, versus 47.4 months for those not pretreated with salvage chemotherapy [12]. In a meta-analysis of studies reporting on secondary cytoreductive surgery, Munkarah and Coleman reported a survival of 44–60 months among patients who underwent secondary cytoreduction and had no gross residual disease after surgery and were then treated with chemotherapy, versus 35 months among patients treated with combination chemotherapy without surgery [17].
All authors agree that patient selection is the most important factor in achieving a positive impact on survival following secondary cytoreductive surgery. The longer the disease-free interval following the primary treatment, the more likely it is that secondary cytoreductive surgery will improve survival. It is unclear whether this reflects tumor biology or surgical aggressiveness. Other factors found to be associated with favorable outcome for secondary cytoreductive surgery include single or few tumor nodules, a tumor size of less than 6 cm, absence of ascites and diffuse carcinomatosis. Patients with chemoresistant or chemorefractory tumors are unlikely to benefit from secondary cytoreductive surgery. A recent study found that response to prior chemotherapy and completeness of secondary cytoreductive surgery correlated with a median survival duration of greater than 50 months compared with 4–8 months for those with neither of these factors [11]. Various studies have demonstrated that complete surgical cytoreduction was possible in 42–77% of recurrent ovarian cancer cases [4,10–16]. Complete cytoreduction was achievable in a larger portion of solitary occurrences versus multiple sites (p = 0.03) [12].
On the other hand, secondary cytoreductive surgery can be associated with significant morbidity and occasional mortality. Tay and colleagues reported an 8.7% incidence of significant postoperative morbidity and 2.2% mortality secondary to the procedure [4]. In their meta-analysis, Munkarah and Coleman reported major perioperative complications in 11% (95% confidence interval [CI]: 8–13%) and a mortality rate of 1.4% (range 0–3.4%) [17]. Major perioperative complications included myocardial infarction, pulmonary emboli, major infections, bowel injury and wound dehiscence.
Finally, the concept of tertiary cytoreduction in recurrent ovarian cancer has been entertained. A Memorial Sloan-Kettering Cancer Center study retrospectively examined 26 patients operated on over 12 years in what was termed tertiary surgery for indications other than bowel obstruction [18]. The median disease-specific survival was 36.3 months in those completely cytoreduced versus 15 months (p = 0.05) in those with visible residual disease. A median disease-specific survival of 36.3 months was observed among patients with 0.5 cm or smaller residual tumors versus 10.6 months among patients in whom the residual tumor was larger than 0.5 cm (p < 0.001) [18].
Chemotherapy
Several chemotherapeutic agents have been utilized among women with recurrent ovarian cancer, either singly or in combination. Tables 2 & 3 summarize the major studies reviewing chemotherapy for recurrent ovarian cancer.
Chemotherapeutic regimens in recurrent ovarian cancer.
Carboplatin and paclitaxel as second-line therapy in women with recurrent ovarian cancer.
NA: Not available.
Platinum
Carboplatin and cisplatin are two platinum-containing compounds that have been employed in the treatment of recurrent ovarian cancer, both as monotherapy and in combination with other chemotherapeutic agents. The main mechanism of action of both drugs is DNA cross-linking and the major toxicity is myelosuppression. Carboplatin appears to have a better toxicity profile and faster time of onset of action than cisplatin. Carboplatin as a monotherapy appears to have some efficacy against recurrent ovarian cancer treated initially with platinum and taxanes. Kavanagh and colleagues demonstrated that 21% of patients with ovarian cancer who recurred following platinum and taxane chemotherapy demonstrated a partial response with 300 mg/m2 of carboplatin at 28-day intervals once disease was diagnosed as progressing on intervening taxane monotherapy [19]. In 2001, Bolis and colleagues stratified patients to receive either 300 mg/m2 of carboplatin on a 28-day cycle versus epidoxorubicin (120 mg/m2) and carboplatin (300 mg/m2) every 28 days for a total of five cycles [20]. A total of 36 and 20.2% of the patients in the carboplatin group alone and 32 and 30% of the patients in the carboplatin and epidoxorubicin group experienced a complete and partial response to chemotherapy, respectively. Women receiving the combination chemotherapy had a higher incidence of grade 3/4 myelotoxicity.
Carboplatin and paclitaxel in combination have been well studied in the treatment of women with recurrent ovarian cancer. Several studies involving platinum-sensitive patients demonstrated excellent overall response rates (ORRs) (partial and complete) of between 70 and 90% to the combination of carboplatin and paclitaxel given every 3 weeks or weekly, with tolerable toxicity [21–25]. Most of these patients were initially treated with paclitaxel and platinum first-line chemotherapy. The median progression-free survival was between 9 and 13 months using carboplatin doses at 5–6 area under the curve (AUC) every 3 weeks and paclitaxel weekly at 60–80 mg/m2 or every 3 weeks at 135–188 mg/m2 [22–24].
In a parallel, international, multicenter, randomized trial, the combination of paclitaxel and carboplatin was compared with conventional platin-based chemotherapy among women with platinum-sensitive recurrent ovarian cancer [26]. The majority (71%) of patients in the conventional platinum-based group received carboplatin alone. The authors demonstrated that paclitaxel in addition to carboplatin significantly improved OS (OS) and progression-free survival in patients with platinum-sensitive recurrent ovarian cancer (p = 0.023). Patients who received the combination of carboplatin plus paclitaxel had a higher response rate than those who received carboplatin alone. However, the difference was not statistically significant (66 vs 54%, respectively; p = 0.06).
Paclitaxel
Paclitaxel is one of the most commonly used chemotherapeutic agents in patients with recurrent ovarian cancer. Paclitaxel exhibits cytotoxic effects through microtubule stabilization, thus arresting the cell reproductive cycle. Paclitaxel has been used as monotherapy and in combination therapy. The most commonly reported toxicity was grade 3/4 leukopenia, seen in approximately 49–78% of patients treated [27,28]. Paclitaxel has been studied in various doses and infusion protocols.
Every 3 weeks
Paclitaxel was initially administered as a 24-h infusion every 3 weeks at a dose of 135 mg/m2. A complete response of 4%, a partial response of 18% and a median survival rate of 8.8 months was reported in the first 1000 patients with platinum-refractory ovarian cancer treated with paclitaxel [27]. The lower response rate could be attributed to the fact that the majority of patients had been treated with at least three prior chemotherapeutic regimens. Later, Gore and colleagues examined paclitaxel administered as a 3-h infusion every 21 days, using either 35 mg/m2 for patients who had received three or more prior treatments or 175 mg/m2 for those who had received two or fewer prior regimens [28]. The ORR was 16% and the toxicity profile was similar to the 24-h infusion protocols.
In 1994, the question of optimal infusion protocols was examined by the National Cancer Institute of Canada Clinical Trials Group. Patients were randomized to receive paclitaxel 135 or 175 mg/m2, either as a 3- or 24-h infusion every 21 days. There was a nonsignificant higher response rate using 175 versus 135 mg/m2 (20 vs 15% respectively; p = 0.2) [29]. However, the progression-free interval was 19 weeks in the higher-dose group versus 14 weeks in the lower-dose group (p = 0.02). There was also a nonsignificant difference in response rates (19 and 16% for 24-and 3-h infusions, respectively). No survival difference was noted between the 3- and 24-h infusion groups, but a significantly lower toxicity profile was noted with the shorter infusion [29].
A randomized study compared single-agent paclitaxel with platinum-based combination chemotherapy (cyclophosphamide, doxorubicin and cisplatin in combination) among women with platinum-sensitive recurrent ovarian cancer [30]. The authors demonstrated that the response rate, progression-free survival and OS were better among the patients receiving combination chemotherapy compared with single-agent paclitaxel in this study of patients. As expected, the incidence of myelotoxicity as well as nausea and vomiting were higher among patients receiving the platinum-based combination chemotherapy.
Weekly dosing
The efficacy and safety of weekly paclitaxel was first demonstrated in 1997 by Andersson and colleagues [31]. This study, which involved 40 patients with recurrent ovarian cancer, revealed response rates of 28 and 42% in patients with platinum-resistant and -sensitive disease, respectively. The toxicity was acceptable, indicating that weekly therapy could be as safe as 3-weekly therapy. A later study involving head-to-head comparison of weekly (67 mg/m2) versus 3-weekly (200 mg/m2) paclitaxel demonstrated a total response rate of 35.2 and 36.9%, respectively [32]. Of note, there was a significantly lower grade 3/4 toxicity profile associated with the weekly dosing regimen. These results were later confirmed by Havrilesky and colleagues, who demonstrated a high ORR (82.2%) with an acceptable toxicity profile (grade 3/4 neutropenia and thrombocytopenia of 32 and 14.2%, respectively) for weekly paclitaxel and carboplatin [33]. In 2005, Watanabe and colleagues reported a total response rate of 88% in patients treated with weekly carboplatin at an AUC of 2 and weekly paclitaxel at 60 mg/m2 [24]. Of note, none of these patients experienced higher than a grade 1 thrombocytopenia or neurotoxicity. In a similar study, Kikuchi and colleagues demonstrated a response rate of 77.8% using the same dose of carboplatin and a weekly dose of paclitaxel (80 mg/m2) [25]. In this study, grade 3/4 neutropenia, thrombocytopenia and peripheral neuropathy were 1.7, 90 and 5.1%, respectively.
Docetaxel
Docetaxel has a different toxicity profile from paclitaxel and could replace paclitaxel in the treatment of women with recurrent ovarian cancer, especially those with significant peripheral neuropathy or an allergy to paclitaxel. In a recent study by Niwa and colleagues, docetaxel at a dose of 70 mg/m2 every 3 weeks given to a group of heavily pretreated patients with recurrent ovarian cancer demonstrated a 13% ORR and a median progression-free interval and OS of 4.6 and 13.7 months, respectively [34]. In this study, grade 3/4 neutropenia, leukopenia and anemia were seen in 83.3, 70.8 and 25% of participants, respectively. The only nonhematologic grade 3/4 side effects observed were asthenia/fatigue and nausea/vomiting in 20.8 and 8.3% of participants, respectively [34].
In a larger study of recurrent platinum-resistant ovarian cancer, Rose and colleagues demonstrated a 17% partial and a 5% complete response to docetaxel given at a dose of 100 mg/m2 every 3 weeks [35]. However, 38% of the patients required a dose reduction secondary to grade 3/4 toxicities. In another small study, two out of nine patients experienced a response to biweekly docetaxel at a dose of 70 mg/m2 [36].
Carboplatin and docetaxel have also been studied in combination for the treatment of recurrent ovarian cancer [37]. A study by Beldermann and colleagues demonstrated a significant response rate (30%) with acceptable grade 3/4 toxicities despite previous treatment with first-line carboplatin and paclitaxel [37].
Gemcitabine
Gemcitabine is a synthetic analog of deoxycytidine that exerts its antitumor effect by inhibiting ribonucleotide metabolism, blocking DNA processing and increasing DNA strand crosslinks and adducts, leading to a block in the cell cycle [38]. Gemcitabine has been studied as monotherapy and in combination with other chemotherapeutic drugs, including platinum, etoposide, topotecan and doxorubicin, among women with recurrent ovarian cancer. In Phase II trials involving gemcitabine, a response rate of 13–22% was observed using a dosing schedule ranging from 800 to 1250 mg/m2 [39,40]. Gemcitabine has been shown to be well tolerated with an acceptable toxicity profile, easy administration and an average response rate. Like topotecan, gemcitabine's major toxicity, myelosuppression, is both noncumulative and reversible. Other significant side effects of gemcitabine include hepatic toxicity, nausea, vomiting and fatigue.
Gemcitabine and cisplatin seem to demonstrate synergistic effects when given in combination. The combination of cisplatin and gemcitabine has yielded good response rates (16–64%) among women with recurrent platinum-resistant ovarian cancer [41]. In addition, a relatively high rate of disease stabilization has been observed.
The combination of carboplatin and gemcitabine has been shown to be effective in both platinum-sensitive and -resistant disease. In a Phase II study in potentially platinum-sensitive patients [42], gemcitabine (1000 mg/m2 days 1 and 8) and carboplatin (AUC 4 day 1) every 21 days demonstrated a total response rate of 62.5%, with a 15% complete response. In this study, 78% of patients experienced grade 3/4 neutropenia. In a subsequent study evaluating gemcitabine (1000 mg/m2 days 1 and 8) and either cisplatin (75 mg/m2 day 1) or carboplatin (AUC 5 day 1), an ORR of 55% was observed [43]. A total of 69% of participants experienced grade 3/4 hematologic toxicity, with 63% requiring growth-factor support by cycle four. A recent collaborative study using gemcitabine (1000 mg/m2 days 1 and 8) and carboplatin (AUC of 4 day 1) in a 21-day cycle among women with platinum-sensitive recurrent ovarian cancer demonstrated a total response rate of 47.2% and a statistically significant progression-free advantage in those treated with the combination therapy versus carboplatin alone (8.6 vs 5.8 months, respectively; p = 0.003) [44].
Gemcitabine in combination with paclitaxel has been studied in recent trials [44–46]. Garcia and colleagues demonstrated that weekly paclitaxel (80 mg/m2) and gemcitabine (1000 mg/m2) on days 1, 8 and 15 every 4 weeks was associated with a 40% response rate and an overall median survival of 13.1 months among women with recurrent platinum-resistant ovarian cancer [44].
The combination of gemcitabine (600 mg/m2 days 1 and 3) and topotecan (0.9 mg/m2 days 1–3) has demonstrated a response and stable disease in 13 and 38% of patients with platinum-resistant disease, respectively [47]. The significant toxicities associated with this regimen were thrombocytopenia and leukopenia.
Liposomal doxorubicin
Doxorubicin has several mechanisms of action: it inhibits DNA synthesis by selectively binding to certain base pairs, it is a potent generator of oxygen free-radicals, and finally, it inhibits topoisomerase II. In its pure form, doxorubicin's major side effect is cardiac toxicity. It is now available in a better-tolerated form as liposomal doxorubicin, surrounded by a polyethylene glycol coat, therefore referred to as pegylated liposomal doxorubicin. Liposomal doxorubicin is currently approved by the US Food and Drug Administration (FDA) for the treatment of platinum-resistant and -refractory recurrent ovarian cancer [48].
In a randomized study, Gordon and colleagues compared liposomal doxorubicin (50 mg/m2 every 28 days) with topotecan (1.5 mg/m2 on days 1–5 of a 21-day cycle) among women with recurrent ovarian cancer [49]. Patients treated with liposomal doxorubicin experienced a statistically significant survival of 63.6 versus 57 weeks for those treated with topotecan. In the platinum-sensitive subset of patients, there was a significant survival advantage for liposomal doxorubicin compared with topotecan (108 vs 70 weeks, respectively) [49]. Grade 3/4 leukopenia, anemia and thrombocytopenia were observed in 12, 5 and 1% of patients treated with liposomal doxorubicin, respectively [49]. The most common grade 3/4 nonhematologic toxicities associated with liposomal doxorubicin were hand–foot syndrome (23%) and stomatitis (8%), both of which appear to be dose related and occur in those receiving doses of 50 mg/m2 or greater [49,50]. Liposomal doxorubicin has significantly lower rates of cardiac toxicity compared with doxorubicin, and the majority of cases of cardiac toxicity reported with liposomal doxorubicin were among patients with pre-existing cardiac conditions [49]. Uyar and colleagues demonstrated that prolonged liposomal doxorubicin chemotherapy was not associated with significant cardiac toxicity [51].
D'Agostino and colleagues examined liposomal doxorubicin and gemcitabine in combination [52]. In this Phase II study, 70 patients received liposomal doxorubicin (30 mg/m2 day 1) and gemcitabine (1000 mg/m2 days 1 and 8) every 21 days. A total response was observed in 45% of platinum-sensitive and 25% of platinum-resistant patients [52]. A total of 42% of patients experienced grade 3/4 hematologic toxicity and 34% experienced palmar–plantar erythordysesthesia [52].
Liposomal doxorubicin-associated palmar–plantar erythrodysesthsia could be reduced by lowering the dose to 40 mg/m2 every 4 weeks, avoiding heat and pressure before, during and after infusion and prolonging the infusion time.
Topotecan
Topotecan is a topoisomerase I inhibitor which directly causes single-strand DNA breaks, which then translate into double-stranded breaks in replicating tumor cells. Topotecan has been used for the treatment of both platinum-sensitive and -resistant relapsed ovarian cancers. As expected, the response is generally greater in platinum-sensitive tumors. A compilation of noncomparative trials by Herzog demonstrated a response rate of 19–33% in platinum-sensitive and 12–33% in platinum-resistant and -refractory tumors [53].
Topotecan is currently approved by the FDA as an intravenous infusion of 1.5 mg/m2 for 5 consecutive days of a 21-day cycle. Although effective, this dosing schedule is associated with significant morbidity, including grade 3/4 myelosuppression, which fortunately is noncumulative and reversible. Other associated side effects are fatigue, nausea and neuropathy, all of which are generally grade 2 or less [54]. To overcome myelosuppression, a weekly regimen of 4 mg/m2 has demonstrated adequate activity with reduced toxicity [54–56]. Using this regimen, the main toxicities observed were grade 2/3 thrombocytopenia and fatigue [54–56]. The ORRs were 47–52% in both platinum-sensitive and -resistant tumors [58–60]. Topotecan (1.5 mg/m2 for 5 consecutive days) has also been compared with paclitaxel (175 mg/m2) every 3 weeks. A response rate of 20.5% was observed with topotecan versus 13.2% for paclitaxel; a nonsignificant difference [57]. Similar response rates (17 and 19%) were observed in a study comparing topotecan (1.5 mg/m2 for 5 consecutive days) with liposomal doxorubicin (50 mg/m2 every 4 weeks), respectively [50].
Etoposide
Etoposide (VP-16) inhibits DNA synthesis by directly affecting topoisomerase II. Based on a Phase II trial by Eckhardt and colleagues, involving patients with recurrent ovarian cancer, etoposide at a dose of 150 mg/m2 intravenously on days 1 and 3 of a 28-day cycle achieved a response of 8.5%, and 67.6% of patients had stable disease [58]. The major toxicities in this study were myelosuppression, nausea and vomiting. Studies have demonstrated that prolonged oral etoposide (50 mg/m2 orally daily for 21 days every 28 days) induced response rates of 16 and 27% in patients with platinum-resistant disease [59,60]. Significant toxicities associated with etoposide include myelotoxicity and the risk of developing secondary myelodysplasia or acute leukemia [61].
The combination of etoposide and topotecan has been studied among women with recurrent ovarian cancer. A group of 22 patients with recurrent ovarian cancer were treated with intraperitoneal topotecan (1 mg/m2 on days 1–5) and oral etoposide (100 mg/day on days 6–9) every 28 days [62]. Topotecan and etoposide plasma levels and half-lifes were evaluated throughout the treatment schedule. In this study, 64% of patients completed all six cycles. The most common grade 4 toxicities were neutropenia and thrombocytopenia, seen in 36 and 18% of patients, respectively. The ORR was 38%.
In a subsequent multicenter trial, 28 patients with recurrent platinum-resistant ovarian cancer received a fixed dose of topotecan (1 mg/m2 days 1–5) and an escalating dose of etoposide (50, 75 or 100 mg/day on days 6–12) every 28 days [63]. A total of 32% of patients achieved an objective response by Response Evaluation Criteria In Solid Tumors (RECIST) or CA 125 response criteria. In this study, the dose-limiting toxicity was grade 4 neutropenia and sepsis in 3 and 2% of patients, respectively. One patient developed acute myeloid leukemia 10 months after completion of 12 cycles of topotecan–etoposide. Hematologic toxicities and sepsis mandated a halt to the study and the authors concluded that combined topotecan and etoposide at this dose and schedule were inappropriate in patients with recurrent ovarian cancer, due to unpredictable hematologic toxicity.
Maintenance chemotherapy
There have been few data published on maintenance chemotherapy in recurrent ovarian cancer. Eltabbakh and colleagues studied maintenance chemotherapy among women with platinum-sensitive recurrent ovarian cancer who achieved complete response to salvage chemotherapy [64]. The authors compared disease-free survival between the patients who accepted maintenance chemotherapy and those who refused it. Patients who received maintenance chemotherapy had a significantly longer disease-free interval compared with controls (35 versus 6 months, respectively; p = 0.001). However, there was no significant difference in the OS from initial diagnosis between the two groups.
Radiation therapy
Radiation therapy could be an effective treatment modality for localized recurrences of ovarian cancer, especially those involving the vagina or causing symptoms. However, the role of radiation therapy for women with disseminated intraperitoneal recurrence is questionable. Firat and colleagues reported on 28 patients with ovarian cancer who had vaginal or perirectal recurrences [65]. Most of these patients were treated with external pelvic radiation therapy and some of them received vaginal brachytherapy, either alone or in combination with external pelvic radiation. The authors reported that vaginal bleeding was controlled in all patients and that symptomatic response was achieved in 79% of patients who had symptoms.
Dowdy and colleagues reported on 62 patients with recurrent ovarian cancer who received whole abdominal radiation therapy following secondary cytoreduction [66]. The median dose to the whole abdomen was 25.5 Gy and some patients received pelvic or para-aortic boosts. Three patients died of treatment-related causes and 15% of the patients developed small-bowel obstruction. The latter complication was more common among the patients who had received a pelvic boost. The authors concluded that the therapeutic index for whole abdominal radiation therapy may not be acceptable in patients with recurrent ovarian cancer regardless of the degree of cytoreduction. A recent study examined the impact of tumor volume-directed involved-field radiation therapy integrated in the management of 35 patients with recurrent ovarian cancer [67]. A total of 20 patients received tumor volume-directed involved-field radiation therapy for localized extraperitoneal recurrences (either as consolidation following debulking surgery or as attempted salvage if unresectable). The response rate following radiation therapy was 85% and the toxicity was acceptable. One (5%) patient required surgery for bowel obstruction. The authors concluded that tumor volume-directed involved-field radiation therapy was effective in controlling localized recurrences of ovarian cancer, especially after they are optimally debulked.
Novel treatment modalities
Despite aggressive cytoreductive surgery and effective chemotherapy, most women with recurrent ovarian cancer will eventually succumb to their disease. New and novel treatment modalities are needed. Several recent studies have explored new treatment options for these patients. Zanon and colleagues attempted extensive cytoreductive surgery, including peritonectomy followed by intraperitoneal chemohyperthermia with cisplatin, among 30 patients with recurrent ovarian cancer [68]. The authors concluded that this treatment modality was feasible, with acceptable morbidity and mortality, and seemed to promise good results in selected patients affected with peritoneal carcinomatosis from ovarian cancer.
Recent studies looked into the feasibility of using gene therapy among women with recurrent ovarian cancer [69,70]. Hasenburg and colleagues treated ten patients with recurrent ovarian cancer with secondary cytoreductive surgery to a residual tumor smaller than 0.5 cm [69]. Patients with good intraperitoneal flow then received intraperitoneal replication-deficient recombinant adenovirus containing the herpes simplex virus thymidine kinase gene. Vector delivery was then followed by intravenous administration of antiherpetic prodrug and topotecan. Three patients were alive more than 30 months following gene therapy. The authors recommended initiation of a Phase II study with a larger number of patients and application of multiple cycles of gene therapy.
Future perspective
The sequence of treatment for women with advanced-stage ovarian cancer (primary cytoreductive surgery followed by chemotherapy) might be challenged in some patients. Some patients could be offered neoadjuvant chemotherapy followed by interval cytoreductive surgery if they respond to chemotherapy.
The scope of surgery in some women with recurrent ovarian cancer might be expanded to include peritonectomy, partial hepatectomy and radiofrequency ablation of liver metastases. Some patients who achieve complete cytoreduction might be treated with heated intraperitoneal chemotherapy.
Maintenance chemotherapy might be used in a selected groups of patients who have chemosensitive tumors and achieve a response to salvage chemotherapy.
Targeted immune modulators might be used more widely among patients with recurrent ovarian cancer.
Executive summary
Ovarian cancer is the leading cause of death for all gynecologic malignancies in developed countries, owing in large part to the often late stage of diagnosis.
Approximately 65% of patients will have recurrent or persistent disease following initial surgery and chemotherapy.
Based on the interval between the original treatment and tumor recurrence, patients with ovarian cancer are classified into three groups: chemosensitive (recurrence >6 months from the end of treatment), chemoresistant (recurrence within 6 months from the initial treatment) and chemorefractory (progression during initial treatment).
Approximately 50% of patients with recurrent ovarian cancer are asymptomatic.
Recurrences are often diagnosed using a combination of tests, including cancer antigen (CA) 125, computed tomography, magnetic resonance imaging and positron emission tomography scan.
The most significant prognostic factor among women with recurrent ovarian cancer is the length of time from initial diagnosis to recurrence.
Treatment of recurrent ovarian cancer generally involves chemotherapy, with or without surgery. In a select group of patients, secondary cytoreductive surgery might significantly improve survival.
Radiotherapy may have a role in the treatment of a small group of patients with recurrent ovarian cancer who have localized symptomatic masses.
New treatment modalities for women with recurrent ovarian cancer are needed, as none of the available treatments are curative. Targeted gene therapy is one of the new treatment modalities that might have potential.