
Abstract
A discussion of rational endpoints in clinical trials seeking regulatory approval for new anti-neoplastic agents involving the three major gynecologic malignancies, cancers of the ovary, cervix, and endometrial, is particularly interesting as (in the opinion of this commentator) the conclusion will be different in the individual cancers.
Keywords
Ovarian cancer
The major role played by ovarian cancer in anti-neoplastic drug development over the past several decades cannot be overstated. It was in the management of ovarian cancer that the initial regulatory approval of cisplatin, carboplatin, and paclitaxel occurred. 1 These cytotoxic agents remain today extremely important in the treatment of a number of human malignancies.
However, since the landmark study reporting improved overall survival associated with the substitution of paclitaxel for cyclophosphamide, when combined with cisplatin, as therapy of advanced ovarian cancer, primary cytotoxic “standard-of-care” anti-neoplastic therapy in this malignancy has not changed in now more than 20 years. 2 And while carboplatin has been substituted for cisplatin as a result of a more favorable toxicity profile, 3 and some have substituted docetaxel for paclitaxel due to a different (but not clearly more favorable) side effect pattern, 4 there has been little change in the primary chemotherapeutic armamentarium for ovarian cancer.
Yet, despite these sobering facts, there has been considerable progress made in extending survival in the malignancy as a result of the availability of an increasing number of anti-neoplastic drugs with both demonstrated biological and clinical activity in the malignancy that individually may favorably impact survival. 5 Some (including this commentator) have begun to describe the natural history of ovarian cancer in many women as being a very serious, but “chronic disease process,” where the ultimate cause of death is highly likely to be the result of progression of the malignancy, but where extended survival (measured in “years”) is realistically possible. 6
As a result, it is critical to fully understand the impact of a more prolonged natural history of disease on randomized controlled trial endpoints, and particularly studies designed to consider overall survival as the primary goal/endpoint of treatment.
A most provocative and quite elegant model from two prominent cancer biostatisticians addressing this particular issue emphasizes the magnitude of the problem. 7 In their analysis, a theoretical “trial” was employed which involved 280 patients and demonstrated a statistically significant median 3-month improvement in progression-free survival. The researchers next asked how many additional patients would be required to be included in this study if the goal was to also document a statistically significant improvement in overall survival, and taking into careful consideration the anticipated patient post-progression survival (following completion of this trial).
The investigators noted that if the median post-progression survival was anticipated to be only 2 months, a total trial population of only 350 patients would be required to demonstrate a statistically significant improvement in overall survival. However, if the median post-progression survival was anticipated to be 24 months, a total of 2400 patients would be required to have been entered into the trial and followed to observe a statistically significant improvement in overall survival.
Recognizing the analysis noted above is based on a theoretical construct of a possible post-progression survival outcome, it is relevant to inquire if such extended survival may occur in ovarian cancer and if there are data to support the argument that with the availability of more effective anti-neoplastic therapy in ovarian cancer survival is truly increasing.
In fact, highly provocative data strongly supporting this assertion are provided by an examination of the results of two completely independent phase-3 randomized trials initiated 8 years apart in the treatment of recurrent potentially platinum-sensitive ovarian cancer (Table 1).8,9
Study outcomes of carboplatin plus gemcitabine in recurrent potentially platinum-sensitive ovarian cancer.
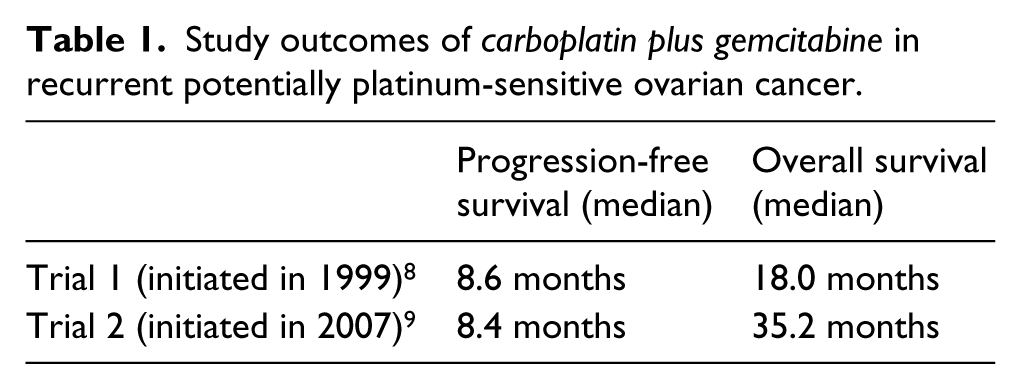
The first study, initiated in 1999, compared the combination of carboplatin/gemcitabine (“experimental arm”) to single agent carboplatin. 8 The second study, initiated in 2007, used the identical carboplatin/gemcitabine regimen, but in this study the combination served as the “control arm” to be compared to the “experimental” three-drug combination of carboplatin/gemcitabine/bevacizumab. 9
While “cross-trial” comparisons are always fraught with danger due to recognized and unrecognized differences in the patient populations entered into different studies, it is notable that the carboplatin/gemcitabine regimens in the two independent studies produced almost identical median progression-free survival outcomes.8,9 These results provide a highly relevant level of assurance that the populations included in the two different studies were similar with regard to baseline clinical characteristics, and the combination chemotherapy regimens produced a comparable degree of clinical utility.
Yet, the median overall survival outcomes observed in the two patient populations separated in time by approximately 8 years was strikingly different (Table 1). In view of the similar degree of efficacy associated with the trial-based therapy (carboplatin/gemcitabine), the logical conclusion for the almost doubling of overall survival in the more recent trial was the impact of various therapies employed following treatment within this trial. Such therapy may have included one of several available cytotoxic approaches, or even a “cross-over” to bevacizumab (subsequently used alone or in a combination regimen with chemotherapy).
In fact, while the “experimental” carboplatin/gemcitabine/bevacizumab was found in the trial to substantially improve progression-free survival, there was no difference in overall survival compared to the carboplatin/gemcitabine “control arm.” 9
In sum, today, the failure of a randomized study in ovarian cancer to reveal an improvement in overall survival when it is documented to favorably impact progression-free survival is simply not because of the absence of utility of the strategy, but almost certainly as a result of post-therapy treatment that positively influences the overall survival endpoint.
Therefore, it is appropriate to conclude that today the most appropriate endpoint to evaluate the clinical utility of a new anti-neoplastic strategy in ovarian cancer is an improvement in progression-free survival. Of course, this does not mean it will be impossible for a future novel approach to be shown to impact overall survival in a randomized trial in ovarian cancer, but only that the failure to achieve this goal does not mean the approach is without meaningful clinical merit.
Cervix cancer
In striking contrast to ovarian cancer, it is particularly distressing that despite decades of clinical trials, there remains only one class of even moderately active anti-neoplastic cytotoxic agents in this malignancy. Since the introduction of cisplatin into the oncologist’s armamentarium more than 40 years ago and the demonstration of its administration could result in partial shrinkage of metastatic or locally advanced cervical cancer, this drug has been the main anti-neoplastic agent employed in the malignancy. 10
While various combination platinum-based chemotherapy regimens have been examined in cervix cancer, differences in clinical outcomes (compared to single agent cisplatin) are quite modest and there is currently no evidence that any particular cytotoxic combination program is superior to one of several other options. The general selection of “cisplatin plus paclitaxel” is based both on its familiarity within the oncology community and generally somewhat more favorable toxicity profile compared to other cisplatin combinations.11,12
And despite the fact cisplatin is currently routinely employed earlier in the course of the illness as a critical component of a chemo-radiation strategy that has been documented to improve overall survival in locally/regionally advanced cervix cancer, a recent phase-3 randomized trial revealed the administration of a cisplatin/paclitaxel regimen in recurrent or persistent cervix cancer (following the use of cisplatin with radiation) was equally or more active than a non-cisplatin containing cytotoxic program (paclitaxel/topotecan). 13
Of note, the addition of bevacizumab to a regimen of either cisplatin/paclitaxel or paclitaxel/topotecan has been shown to modestly improve overall survival (median = 3.7 months) in patients with metastatic, persistent, or recurrent cervix cancer compared to either of these two cytotoxic chemotherapy regimens alone. 13 This is a relevant study result, but the fact it must be highlighted as one of the very few “positive” studies in cervix cancer over the past several decades emphasizes the paucity of therapeutic advances in this clinical setting.
In summary, based on the very limited current availability of anti-neoplastic agents in cervix cancer that have been shown to produce either meaningful biological or clinical effects, and the recognized toxicity profile of all existing therapies in this malignancy, it would be most reasonable to conclude that any agent or regimen proposed for regulatory approval should be required to demonstrate an improvement in overall survival in a well-defined clinical setting.
And in sharp contrast to the situation in ovarian cancer, an overall survival endpoint would be most unlikely to be obscured by the known effects of any anti-neoplastic approach following disease progression on a randomized trial.
Endometrial cancer
For several reasons, there has been a rather striking paucity of large meaningful studies in endometrial cancer. First, advanced or metastatic disease is fortunately not common, at least compared to cancers of the ovary and cervix. Second, it has been well-recognized that endometrial cancer represents a quite heterogeneous group of conditions, with some cancers responding to hormonal manipulations (e.g. low-grade malignancies), and others being highly responsive (at least for a short period of time) to cytotoxic chemotherapy (e.g. papillary serous subtype). Finally, sarcomas are not uncommonly seen in this setting and these malignancies exhibit limited responsiveness to current anti-neoplastic regimens.
While there has been considerable effort undertaken to define unique molecular subtypes of endometrial cancer and a variety of “targeted” approaches have been actively explored, to date these efforts have been largely unsuccessful.14,15
As a result, it would be reasonable to propose that a number of novel trial strategies be permitted to be explored in endometrial cancer with the hope that a unique strategy, perhaps targeting a small subset of patients with the malignancy may be discovered and subsequently “approved” to benefit that specific patient population. This might include single arm phase-2 studies that require a high objective response rate (e.g. > 50%) in a reasonably large trial (e.g. > 50 patients) with a mandated prolonged progression-free survival of the responding population (perhaps compared to a well-defined historical control) to permit regulatory approval.
Conclusion
Drug development in the gynecologic malignancies represents different ends of the spectrum regarding the effectiveness of therapy and the need to be flexible in study design based on the current status of both clinical research and existing therapeutics in the specific areas.
Footnotes
Declaration of conflicting interests
The author(s) declared following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: I have served on both the speakers bureau and a medical advisory board for Genentech and Astra-Zeneca.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.