
Abstract
The aim of this paper is to assess the historical role of radiotherapy in the treatment of sinus infections. This assessment involved a literature-based review of how radiotherapy was used to treat sinus infections in the first half of the 20th century. Low doses of x-rays were used with considerable success to treat nearly 3,000 patients of sinus infection in a span of 12 years with these cases being reported in leading medical journals as case studies. The mechanism of x-ray induced reduction of inflammation and increased tissue repair is uncertain but appears to be related to the development of a multifactorial and integrative anti-inflammatory phenotype.
INTRODUCTION
X-rays were widely used during the early decades of the 20th century in the treatment of a wide range of human diseases. During this period there were few reliable pharmaceutical options, and little government regulation on the use and applications of x-ray treatments. Thus, x-rays were widely explored and reported in leading medical journals via the use of case studies. As a result of such activities a number of apparently successful patient treatment strategies emerged for the clinical application of x-rays for various non-cancer diseases. Recent reviews have addressed the historical use of x-rays in the treatment of gas gangrene (Calabrese and Dhawan, 2012; Cuttler, 2007), dermal staphylococcus infections as seen with carbuncles and furuncles (Calabrese 2013a), and otitis media/deafness, and arthritis (Calabrese and Calabrese, 2013a; Calabrese and Calabrese, 2013b). In each of these areas, a substantial body of research was published which supported an overall conclusion that x-ray treatment had some significant positive measure of efficacy. With the discovery and availability of antibiotics in the 1940s, the use of x-rays in the treatment of gas gangrene, carbuncles/furuncles and otitis media quickly ended. In the case of arthritis, treatment via x-rays was quickly supplanted by various pharmacological agents, although 40,000-50,000 patients have been treated each year with low level x-rays in Germany for this condition (Trott, 1994). Mechanistic studies have now emerged that may help to explain those prior observations (Rödel et al., 2012). The present paper extends these historical observations by assessing how radiotherapy was used to treat sinus infections in the first half of the 20th century.
SINUS INFECTIONS AND RADIOTHERAPY
The first report in the medical literature concerning the effects of x-rays on sinus infections was by Osmond (1923). However, this author actually began investigations on this topic seven years earlier in 1916. After observing that patients' pain in the forehead was relieved following radiograms to diagnose frontal sinusitis, he initiated clinical investigations in this area. The 12 cases that Osmond (1923) reported were patients with sinus infections that ranged from as short as several weeks duration to about six months. In each of these cases pain and discomfort markedly diminished within several hours to several days with all symptoms being absent within 1–3 weeks. Typically there were 2–3 x-ray treatments, each separated by a few days. Some of these patients had a long history of constant watery discharge, multiple irritations of the antra, and daily treatments with agents such as argyrols, adrenalin and mild cocaine. This publication was to provide the initial incentive to others in this field to explore whether x-ray treatment would be of value in the clinical therapeutics of sinus infections.
The following paper assesses the published medical literature on the effects of x-rays on the clinical course of sinus infections. The subsequent literature spans the relatively brief period, from 1932 to 1943. After 1943 the use of x-rays for sinus treatment ended with the arrival of antibiotics. Nonetheless, there was a consistent and modestly robust clinical literature based principally in the field of radiology on sinus treatment. An assessment of this literature reflects a clear tension between the rhinologists and the radiologists. The typical treatments for sinus infections during the 1920–1930s involved inhalations, packing, suction, washings and surgery (Salinger, 1944), all performed under the direction of the rhinologist. However, the radiologist often treated the so-called failed cases of the rhinologist. Sometimes these two groups competed while this was not the case in others. The radiologists became convinced that their treatment should be provided during the early stages of the disease but not in postoperative conditions. Thus, there emerged the need for both medical disciplines to develop an effective degree of cooperation in order to better serve the health of the patient.
The research team that provided the most significant leadership in the assessment of x-rays on sinus infections was that of Frank E. Butler and Ivan Woolley at the Department of Radiology at the University of Oregon Medical School. Their interest in using x-ray therapy on chronic sinus infections was long-standing, originating from observations when physicians injected the antra with opaque substances along with the co-presence of early pathologic reports showing hyperplasia of the lymphoid tissue in the removed membranes.
In April of 1930 their first attempt to use x-rays in the treatment of a chronic sinus infection occurred when one of their technicians consented to such treatment as a last resort prior to surgery. Following a successful resolution to this initial case, they initiated a program to treat cases with chronic sinusitis, publishing a summary of 100 cases in 1932, 700 cases in 1934 and 2,000 cases by 1938 (Butler and Woolley, 1932, 1934, 1938), more cases than all other published papers combined (Table I). They also collaborated with animal model researchers at the University of Oregon to assess the capacity of cats as a model system, to assess the pathophysiological occurrence of chronic sinusitis (Fenton and Larsell, 1932). During this process Butler and Woolley (1934) assessed the effect of x-rays on a broad spectrum of sinusitis conditions, ranging from chronic infections with hypertrophic membranes, cases with polyps, atrophic sinusitis, chronic sinusitis with dense fibrotic membranes and with sinusitis following operations to treat this condition. There was a significant difference among the types of sinusitis and the efficacy of the x-ray treatment. The condition most amenable to a highly successful clinical outcome was the chronic infection with hypertrophic membrane. The chronic sinusitis condition with dense fibrosis and the post-operative cases yielded variable results. Likewise, some success occurred with polyp conditions but only after the removal of the polyp. Patients with atrophic sinusitis were generally not successfully treated. Optimalized techniques were summarized by Pendergrass and Hodges (1941) including typical patient exposure geometry.
Number of sinusitis cases treated with x-irradiation by study ∗

The number of cases listed here is 4,492. However, there is some degree of cumulative counting, especially in the listings of the Butler and Woolley cases. The number of unique cases is approximately 3,000.
OPTIMIZING RESULTS
X-rays were most effective when there were markedly thickened membranes with a small air-containing cavity in the center. According to Butler and Woolley (1938, 1942) such patients typically responded favorably to a single x-ray dose. Furthermore, these patients often had a decrease in their secondary symptoms including headaches, neuritis, and bronchitis. These authors also noted that they had better success in the treatment of maxillary as compared with ethnoid sinuses. The dose of x-rays to a lead shielded patient was 300 R measured in air for each side (Butler and Woolley, 1938, 1942).
The findings of Butler and Woolley (1932, 1934, 1938) were strongly supported by other investigations. In general, the variation amongst the studies may have resulted from how the terms “cured”, “improved” and “unchanged” were defined (Tables II and III). These papers were also not explicitly adjusted for the proportion of specific types of sinusitis treatment. This issue was typically reserved for the discussion portion of the published manuscripts. Furthermore, these papers also differed to some extent in x-ray dose, the nature of the exposure to the different sinuses, degree of lead shielding, differing intervals between x-ray treatments, and whether the dose was fractionated or not. Variability in response may have been affected based on the age and gender of the patients and the stage of the infection and infectious agent. Despite this set of possible confounding variables the results presented were highly consistent across studies.
Results reported from x-ray therapy (Source: partly from Maxfield and Martin 1940, page 309)
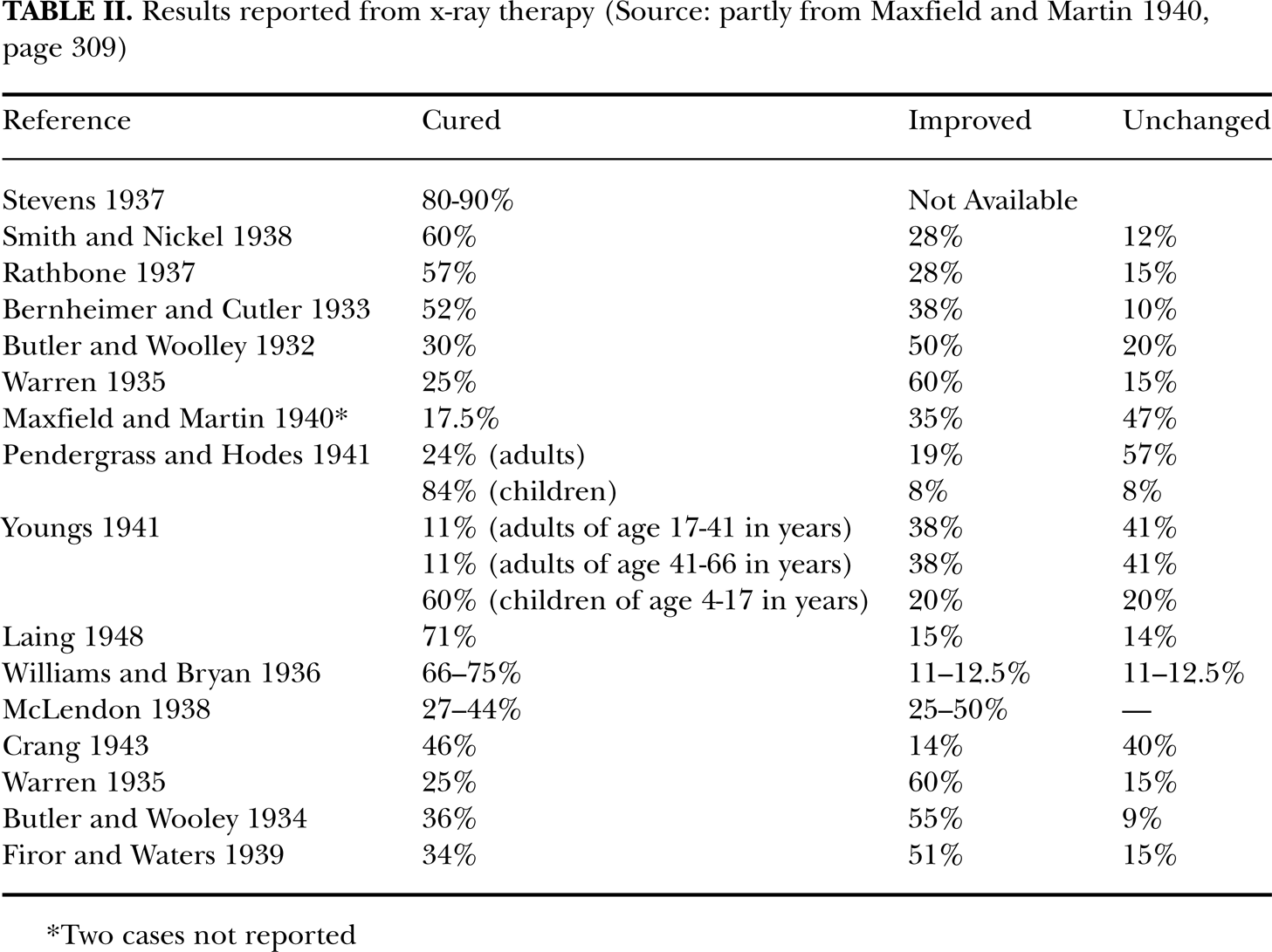
Two cases not reported
X-ray therapy for the treatment of sinus infections: Evaluative criteria

DISEASE PROCESS
The sinus mucosa is thinner and much less vascular than the nose. Thus, the sinus mucosa is more susceptible to infection than the nose. It has a large number of cilia which facilitate the movement of mucous from goblet cells toward the ostium. During an infection, engorgement of the mucosa occurs from increased blood and lymph flow. During this process the cilia become immobilized with large tracts of the surface epithelium being destroyed. There is an influx of histiocytic polymorphonuclear cells (PMNs). As lymphocyte destruction occurs, the histiocytes initiate fibrous repair or transform into macrophages that phagocytize bacteria and cell debris.
The swelling/engorgement of the mucosa adversely affects the function of the cilia. Such altered functioning leads to cilia stasis. Large surfaces containing cilia are eventually destroyed and sloughed out. As the infection becomes chronic, the entire cavity often becomes filled with engorged membranes with the swelling being sufficient to close the ostium and to block drainage. Bacteria are usually present in substantial numbers along the surface as well as buried into tissues. The treatment of such infected tissues by x-rays causes an early disruption of lymphocytes along with an enhancement of macrophages (Butler and Woolley, 1938).
The early influx and destruction of lymphocytes, the release of the antitoxic agents and the early appearance of macrophages in greater numbers, were proposed as a possible process by which x-rays may enhance the usual response to the infection and accelerate the repair process. According to Butler and Woolley (1934, 1938) this accounts for the response that occurs several days following treatments. The patients typically notice an increase in nasal discharge. Other sinus symptoms, starting a few days following treatment, last three or four more days. The above scheme provided the rationale of x-ray therapy in the treatment of sinusitis.
Recent findings have emerged showing an anti-inflammatory phenotype to be a consistent feature when low doses of ionizing radiation are administered to tissues with substantial inflammation. This highly integrated anti-inflammatory phenotype is mediated by: decreases in nitric oxide/inducible nitric oxide synthetase, decreases in reactive oxygen species, increases in heme oxygenase, suppression of TNFα, increases in TNFβ, activation of several transcription factors such as nuclear factor κB (NF-κB) and activating protein 1 (AP-1) as well as decreased adhesion of leukocytes and PMNs to endothelial cells (Calabrese and Calabrese, 2013a, b; Rödel et al., 2002; Rödel et al., 2007). This protective effect of low dose ionizing radiation has been confirmed by mechanistic studies with multiple animal and cell models with various types of inflammatory diseases inducing different forms of arthritis (Calabrese and Calabrese, 2013a, b; Rödel et al., 2002; Rödel et al., 2007). Further research will be necessary to clarify whether the x-ray induced anti-inflammatory phenotype can account, at least in part, for the reported protective effects of x-rays on the course of sinusitis.
DISCUSSION
Approximately a dozen studies have been published on the effects of ionizing-irradiation on sinusitis. These studies include approximately 3,000 patients over a 13 year time span. The methodology used was that for case studies, with cases typically obtained by physicians' referral following the failure of conventional therapy usually via the actions of a rhinologist.
Despite the fact that the methodology was case studies, the cases were typically allocated to differing types of sinusitis conditions and comparisons were made by type for efficacy. This methodology was able to consistently detect poor/low cure rates for some types of sinus conditions but excellent success with others. These consistent findings across studies, investigative teams and differences in research methods lend support to the overall conclusions of differential treatment efficacy according to the specific types of sinus condition. The findings also indicate that there was better success when the dose was given as a single exposure rather than with fractionated doses.
The use of x-rays in the treatment of non-malignant disease was widespread during the 1920 to mid 1940s. The x-ray treatment in the range of 0.3 to 0.7 Gy maximally decreased inflammation, reduced pain, and facilitated the healing process via the enhancement of phagocytosis and via various steps in the process of wound healing (Calabrese, 2013b). In the case of sinus infection, x-ray therapy was determined to be a useful vehicle, especially after conventional therapeutics were tried and failed and before surgery was adopted (Table IV). The use of x-ray therapy after a failed surgery was generally not an appropriate option since a number of studies revealed it to be ineffective in the treatment of the post-operative patient.
Quotations from selected papers reflecting authors' assessment of the capacity of x-rays to treat sinus infections

While this paper is principally intended to summarize the historical use of ionizing radiation in the treatment of sinusitis in the 1920–1940 period, it raises important questions about why x-ray treatments were viewed as successful, their possible underlying mechanisms and whether such historical successes might have clinical relevance today.
Footnotes
ACKNOWLEDGEMENTS
The research on the topic of hormesis has been supported by awards from the U.S. Air Force and ExxonMobil Foundation over a number of years. Study sponsors had no involvement in study design, collection, analysis, interpretation, writing, decision to submit.
DECLARATION OF INTEREST
The authors declare no conflict of interest.