
Abstract
X-ray therapy was used to treat pertussis/whooping cough during a 13-year period from 1923 to 1936 in North America and Europe. Twenty studies from clinicians in the United States reported that approximately 1500 cases of pertussis were treated by X-ray therapy usually with less than 0.5 erythema dose. Young children (<3 years) comprised about 70% to 80% of the cases, with the age of cases ranging from as young as 1 month to 50 years. In general, symptoms of severe coughing, vomiting episodes, and spasms were significantly relieved in about 85% of cases following up to 3 treatments, while about 15% of the cases showed nearly full relief after only 1 treatment. The X-ray therapy was also associated with a marked reduction in mortality of young (<3 years) children by over 90%. Despite such reported clinical success from a wide range of experienced researchers, the use of X-rays for the treatment of pertussis in young children was controversial, principally due to concerns of exposure to the thymus and thyroid even with the availability of lead shielding. By the mid-1930s, the treatment of pertussis cases via vaccine therapy came to dominate the therapeutic arena, and the brief era of a radiotherapy option for the treatment of pertussis ended.
Introduction
Pertussis was a dreaded disease, especially for the very young, having a high risk of death for infants under the age of less than a year. It is characterized by paroxysms of cough, inspiratory whoop, and posttussive vomiting, with more severe forms leading to apnea in infants. The mortality rate for children less than 1 year was about 40% in the early 1900s in the state of Massachusetts. 1 Besides this mortality risk, the nature of the disease was extremely challenging to the affected individual as well as to parents, trying to care for the child, with substantial episodes of extreme coughing and projectile vomiting. Furthermore, the disease was highly contagious, leading to strict quarantining of the affected child. Lack of availability of treatment for pertussis resulted in clinical and psychosocial burden for both patient and the community. Numerous drug experiments were tried to accelerate recovery and enhance survival; however, none of the experiments achieved a significant therapeutic utility. In 1906, hope for a potential treatment arose when the bacterial cause of pertussis was identified. In fact, numerous groups competed to create an effective vaccine, with the next 3 decades witnessing a type of biomedical/clinical roller coaster of expectation and vaccine inadequacy being the norm. By the mid-1930s, an accepted vaccine emerged using a whole cell preparation. This preparation, while broadly effective, would itself pose an array of potential health concerns, giving way to a cell-free preparation by 2000. 2 However, during the earlier decades of the 20th century, between the frantic use of a plethora of failed drug remedies and the adoption of an acceptable vaccine, there emerged a new hope of radiotherapy that resulted in a range of therapeutic possibilities. This article provides a historical assessment of therapeutic use of X-rays in the treatment of pertussis, including the origin of this proposed therapy and a review of the studies assessing its efficacy and associated health concerns. Based on the available data, we also assessed the consistency and robustness of the reported results and various proposed mechanisms that account for reported beneficial effects.
Origin of X-Ray Treatment of Pertussis
The first reported case of pertussis treated by X-rays in the United States occurred as a last resort rather than by design. The case involved the treatment of a young child who exhibited an extremely severe form of pertussis. During the course of disease, the child had been treated with some of the commonly employed drug treatments, without apparent success. In fact, the child had lost much weight, became acutely ill, and there was considerable concern about the development of pneumonia. Given this situation, the mother desperately pleaded with the treating physician for some other treatment. At this point, the physician indicated that he had tried everything except the use of X-rays. Since X-rays had recently received publicity in the apparent successful treatment of several other diseases, the mother pleaded for its use for her child. Despite the presence of considerable skepticism of its therapeutic efficacy, Drs Henry I. Bowditch and Ralph D. Leonard, on the medical staff of the Floating Hospital in Boston, Massachusetts, decided to treat the child with a “low” dose of X-rays, which they estimated to about 1/10 of the erythema dose (ED; note 1). Although the occurrence of paroxysms was markedly reduced that evening, the symptoms recurred the next day with the same severity. A second identical X-ray treatment 48 hours after the first dose yielded a similar transitory improvement. Following a third identical dose at 48 hours after the second treatment, the paroxysms ceased, with no recurrence. As recounted in their 1925 reflection of that event, Bowditch 3 and his team began a major assessment of the effects of X-rays on children and adults with pertussis, with their first paper being first presented to the staff of the Floating Hospital on February 23, 1923, and then published in the Boston Medical and Surgical Journal on March 8, 1923 4 (to be renamed the New England Journal of Medicine on February 23, 1928).
Clinical Investigations of X-Ray Treatment of Pertussis
The publication of Bowditch and Leonard 4 was groundbreaking as it reported 21 (80%) of 26 individuals with marked clinical improvement, including significant reduction in severe bouts of cough and vomiting episodes, after 3 X-ray treatments given on alternative days. In a small proportion of cases, the improvement was more striking with a near complete elimination of symptoms following a single treatment. The cases ranged in age from 3 months to 43 years, with the dose being less than half of an ED. The authors expressed hope that these preliminary findings would encourage other investigators to evaluate the use of X-rays in the treatment of pertussis. In fact, a 1921 report of pertussis mortality in Massachusetts indicated a mortality rate of 6.4% for children under 3 years, with total annual deaths due to this disease approximating 3000. 1 Of particular significance is that for a sample of 850 cases in Massachusetts treated with the standard Bowditch protocol published by Smith 5 revealed mortality rate of only 0.4%, a more than 90% decrease.
By the end of 1923, there were several other reports on the effects of X-rays on cases with pertussis 6 -9 and other research in progress. 10 -14 Thus, the report of Bowditch had its intended effect. These follow-up investigations yielded results very much in line with the initial piloted findings of Bowditch and Leonard. 11 Smith and Kirby 12 reported 20 cases, exclusively including children of age ranging 1 month to 7 years, whereas Struthers 13 reported on 45 cases with an age ranging 3 months to 30 years. Both studies closely followed the protocol of Bowditch and Leonard 4 and Bowditch et al. 11 However, in the report of Bowditch 10 the number of cases was 300, with about 80% showing significant clinical benefit. The number of patients treated via X-rays at the Boston Floating Hospital would increase to 850, with consistent clinical success still approximating 80%. 5
Despite these striking findings, the use of the X-ray treatment of young children caused considerable concern for some treating physicians about potential adverse effects on the thymus and thyroid glands. Such concerns were raised by Cook 8 and Percy 15 who cautioned against giving multiple X-ray treatments to infants. Bowditch 10 defended these treatments by stating that the doses were well under those known to produce skin burns or thymic or thyroid atrophy. Moreover, he stated that when desired, a lead shield was provided to cover the glandular areas. The position of Bowditch was supported in summary remarks of McKibben 7 who cited the views of experienced roentgenologists who worked at the Boston Floating Hospital.
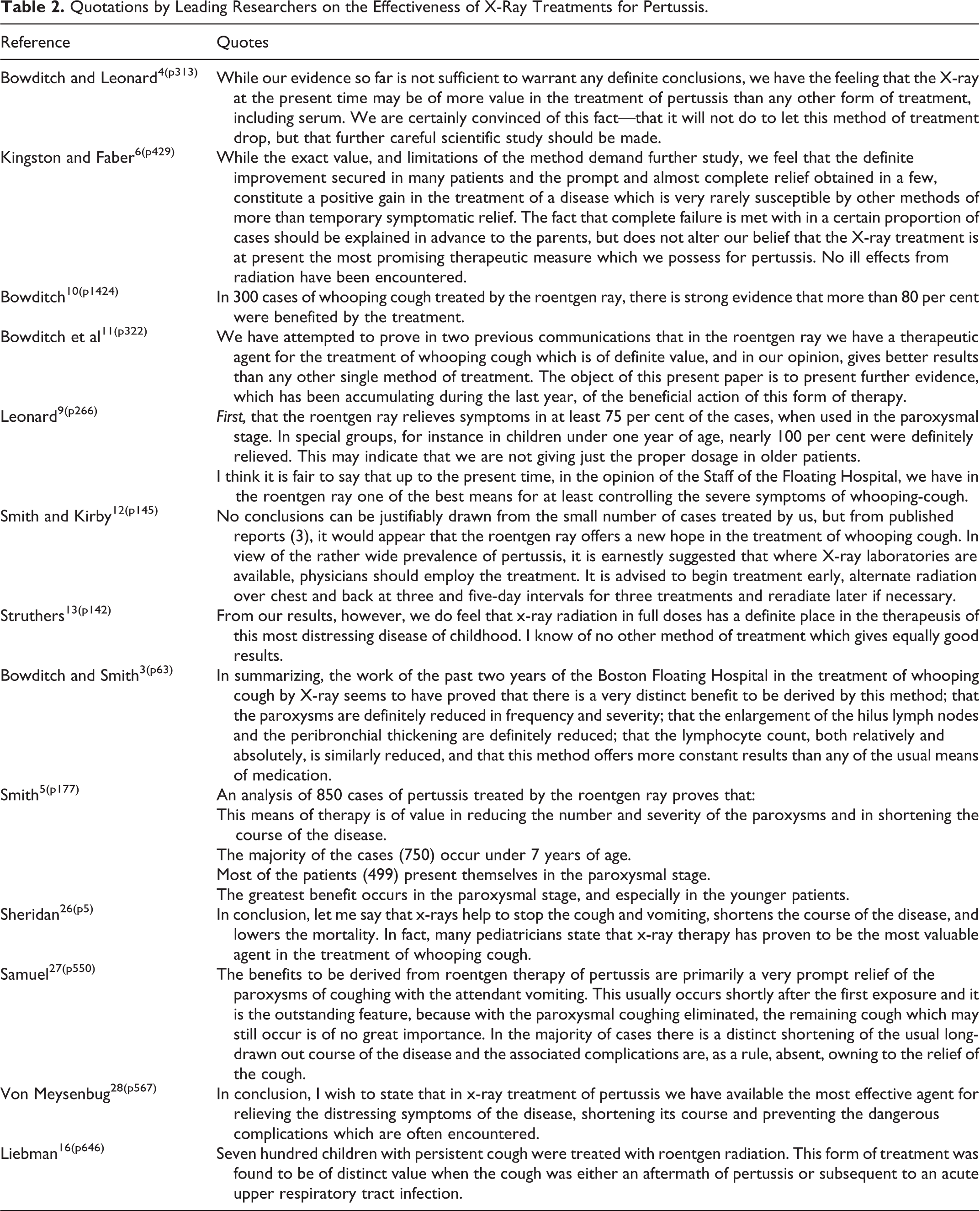
Interest in the therapeutic use of X-rays for pertussis continued until a final paper was published by Liebman 16 in 1936 concerning his 13 years’ experience in Montreal with approximately 170 patients with pertussis that started soon after learning of the original Bowditch report. It was during this time that sufficient progress had been made in the development and testing of a more reliable pertussis vaccine, leading to its widespread adoption and abandoning the use of X-rays for the treatment of pertussis. 2 Approximately 20 papers were published in 13 years, elaborating the therapeutic use of X-ray for pertussis. Table 1 summarizes key findings of these papers, while Table 2 provides a brief set of quotations from a sampling of these papers, permitting the authors to offer their perspectives on how effective they believed these treatments were. Over this time nearly 1500 patients were treated with X-rays, with over 75% being children. With 1 exception, the papers were uniformly consistent in concluding that the X-ray treatments were highly successful in the treatment of those of all ages. In the only study not showing a “successful” treatment, it was not possible to conclude that the X-ray treatment actually was not effective 21 due to limitations of study design. This is because during the experiment the 22 X-ray treated patients was compared to a group receiving the drug antipyrene, with both showing a comparable improvement, no unexposed control group was employed.
Summary of Studies Relating to the Effects of X-Ray Treatment of Pertussis.

Abbreviation: NA, not applicable.
Quotations by Leading Researchers on the Effectiveness of X-Ray Treatments for Pertussis.
Treatment efficacy via the use of x-ray therapy was higher with younger age-groups. In the experience of Bowditch and others, those children under 1 year of age were almost always reported to have significant reduction in symptoms after X-ray treatment. The marked success of the very young led to the suggestion that the dosing had been optimized for the young child but perhaps not so for the adult, 9 even though it was very successful with this age-group as well.
Dose of X-Ray Treatment of Pertussis
The dose of radiation employed in all reviewed studies was noted to be less than 1 ED. Only the Liebman 16 study provided a specific conversion into rad units, with his dose range being from 1/4 to 1/5 ED (135-225 rad). Using information provided in 7 papers, 6,10,12,16,21,22 a dose reconstruction was made using the RadPro software and making several reasonable assumptions depending on the study. These reconstructions confirmed that all doses were below the ED as indicated by the authors. The doses ranged across these 7 studies from a low of 52 27 to a high of 430 to 450 rad. 21,22 Doses were typically reduced by 50% to 70% in infants/very young children to the 50- to 60-rad dose range. 10,27 It is of interest that Faber and Struble 21 noted that “our single and total dosages appear to have been considerably larger than those of Bowditch and Leonard” (p. 816). This was the case for both dose rate and total dose. This conclusion would be consistent with the dose reconstruction presented here. It is unknown what the dose response may be for patients of different ages and gender as this was also confounded in the present series of papers by the existence of different disease stages and severity, all of which might affect treatment efficacy.
Discussion
Strengths and Limitations of Available Evidence
The clinical investigations revealed a range of strengths and limitations. On the strength side was the fact that most of the investigators were highly experienced clinicians with considerable knowledge of pertussis. They also worked closely with radiology experts. The patients do not appear to have been selected with any biased criteria. Usually, the cases were consecutively obtained and enrolled in the study. The studies, therefore, broadly included those of differing ages, gender, ethnicity, health status, and stage of disease. The most significant methodological limitation that was recognized was the lack of a concurrent control group in these studies. There were only 2 studies which reported the presence of concurrent control groups. One study was relatively small with only 22 treatment and 22 control individuals. 21 The other study reported some 400 treatment cases and 200 control group individuals. 9 Leonard 9 did not report details on characteristics and the basis of selection of the control group. However, Leonard 9 did report that the treated cases had an average disease duration of 5.5 weeks as compared to 8.7 weeks for the control. These findings indicate shortening of the illness by 3.2 weeks or nearly 40%. In the smaller study by Faber and Struble, 21 the control was generally selected by alternating patient’s enrollment into the study. However, the investigators failed to follow their limited protocol on 5 different occasions that intentionally directed more severe cases into the X-ray group. None of these studies were blinded.
Thus, the lack of control groups in the overall database, and even the 2 studies reporting such controls, did not assist in a significant manner in the assessment of the findings. There was also a type of quasi control reported in the 1936 study of Liebman. 16 He noted that at the start of the study cases treated with either UV or X-ray radiation were directly compared. After the first 10 patients for both groups were compared, the X-ray-treated patients fared so much better than the UV patients (data not shown in the Liebman study for the 20 patients) that they switched the treatment of all cases entirely to X-rays. Lacking the general presence of a concurrent control group, the researchers in this area of X-ray treatment effects on pertussis were left to infer the occurrence of a treatment-related effect when the cases displayed noticeable and quick relief from the various symptoms in a manner that substantially exceeded their professional experience.
A second issue of some importance that could affect judgment on the success of the treatment was the fact that a definite diagnosis of pertussis was difficult. This was due to reduced sensitivities of the diagnostic tests in the later stages of the illness. Since patients were treated at different stages, some patients would be negative for the presence of the causative agent. Thus, the diagnosis was often made based on the patient history, physical symptoms, diagnostic X-rays, and the experience of the treating physician.
Treatment Protocol Variation
The treatment technique, which originated with the initial publication of Bowditch and Leonard, 4 included the radiation of the anterior chest for the first session, followed by the second session on the posterior chest on alternative days. In a third and usually final session, it was applied on the anterior chest. Other investigators would subsequently modify this protocol such that both anterior and posterior X-rays were administered during the same session. Others also reduced the multiple exposure sessions to only 1 session with a single larger dose. Finally, in the case of multiple treatments, the duration between treatments could be varied from alternate days, up to 1 treatment per week. Despite such differences in exposure protocols over time, the clinical responses were generally similar across studies, suggesting that the effects were independent of exposure interval duration.
Optimizing Dose
The concept of radiation-induced mutation was not discovered until the findings of Muller, 29 with fruit flies. Linkage of X-ray exposure to enhancement of childhood associated tumors would not emerge until after X-ray treatments for pertussis had ended. However, the issue of whether children who were exposed to X-rays for the treatment of pertussis might experience an enhanced cancer risk was raised approximately 5 decades later by Webber 30 who wrote that “it is generally unappreciated by physicians that during the two decades from 1920-1940, hundreds of children received potentially carcinogenic doses of radiation therapy to the thorax for whopping cough” (p. 449). Webber 30 stated that the estimated dose was approximately 100 rad in air per exposure with a total X-ray dose in the range of 300 to 600 rad. In the mid-1930s, even after the introduction of the Sauer pertussis vaccine in 1934, it was likely that X-ray therapy for whooping cough continued for some time thereafter, noting a patient treated in 1937 in Michigan. Webber 30 concluded by raising the issue that as of the 1970s hundreds of adults may have potentially enhanced risk of thyroid cancer due to the radiation treatment during infancy for pertussis.
These speculative comments of Webber 30 are interesting but impossible to assess for multiple reasons. First, there is no record of which patients were lead shielded and the nature of the shielding protocol, if any. It is also unlikely that adult patients may even know that they were irradiated as an infant. Furthermore, the nature of the exposures were limited to generally 1 to 3 treatments, making any possible risks difficult to detect, especially with a very small sample size.
Mechanisms
The theoretical foundation for the use of X-ray treatment for pertussis, according to Bowditch, 10 was based upon the same reasons for its use in bronchitis, that is, the proposed involvement of the hilum lymph nodes in an acute inflammatory hyperplasia. In theory, the X-ray treatment reduced the inflammation, reducing the size of these glands. Although focused mechanistic research of this issue was not undertaken during this era, considerable recent research has indicated that X-ray treatment in the general range of that used to treat pertussis induces an anti-inflammatory phenotype in multiple animal models. 31,32 The radiation-induced anti-inflammatory phenotype has been extensively documented, being reported in a broad range of biological models. These findings suggest that this result may be broadly generalizable. These studies typically explored the underlying molecular mechanisms. Despite the broad range of biological models, consistent molecular patterns (Table 3) were reported that lead to the anti-inflammatory phenotype. Of particular significance is that the radiation-induced impact of disease end points was typically biphasic, showing decreases in disease-related responses at low doses, whereas at higher exposure levels adverse/undesirable health effects were typically noted. These findings have been hypothesized to provide a possible basis for the capacity of X-rays to affect therapeutic benefits on multiple diseases such as gas gangrene, 57 inner ear infections/deafness, 58 sinusitis, 59 shoulder tendonitis/bursitis, 60 arthritis, 31,32 pneumonia, 61 bronchial asthma, 62 and carbuncles and furuncles. 63 Whether such X-ray-induced biphasic dose responses mediated the therapeutic effects seen with pertussis is unknown, but a reasonable potential hypothesis, especially for those radiotherapeutic interventions which involved relatively low-level irradiations applied in fractions with sufficiently long intervals permitting the repair of inflammation-induced tissue injury.
Radiation-Induced Changes Leading to the Development of an Anti-Inflammatory Phenotype in Multiple Biological Models.
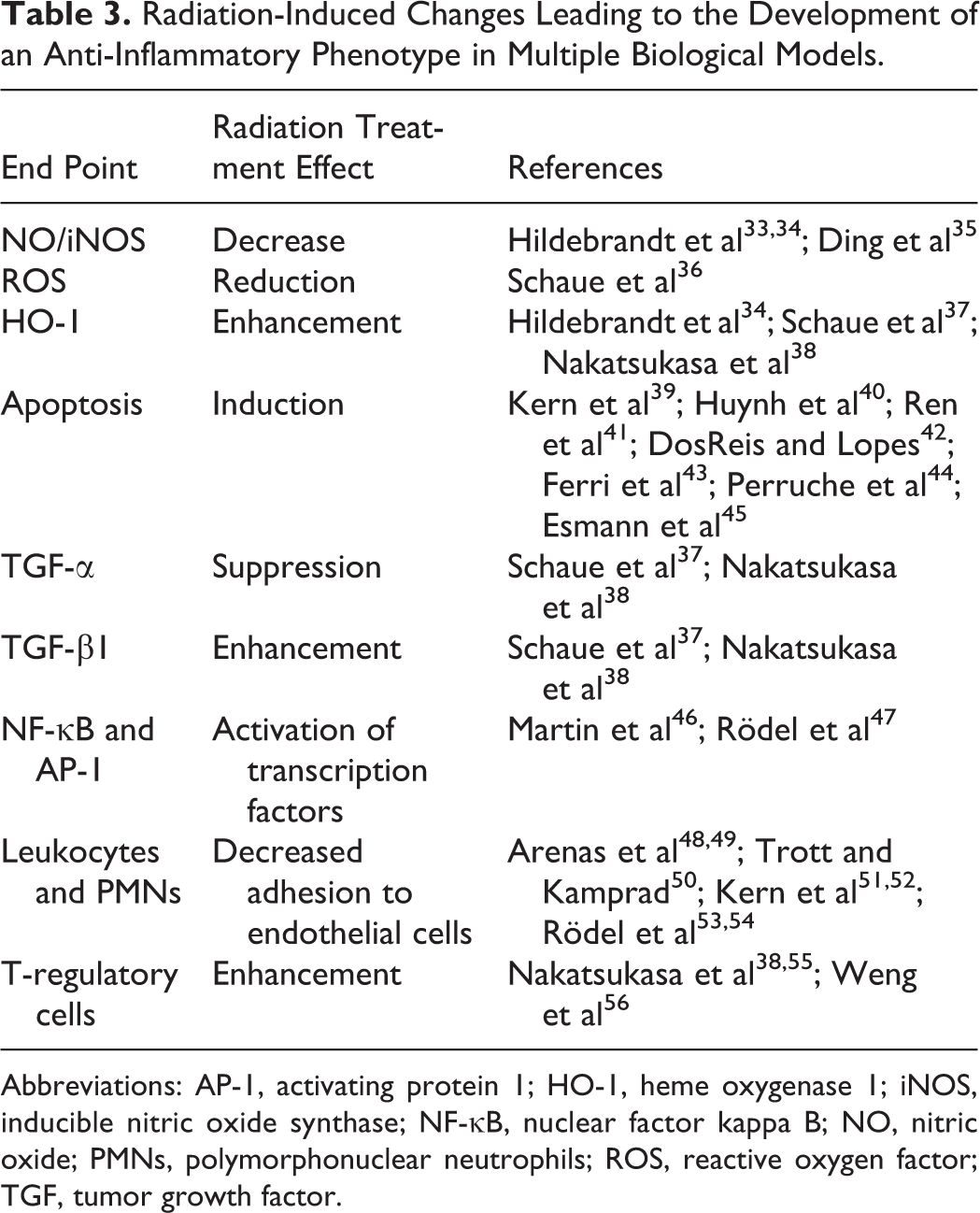
Abbreviations: AP-1, activating protein 1; HO-1, heme oxygenase 1; iNOS, inducible nitric oxide synthase; NF-κB, nuclear factor kappa B; NO, nitric oxide; PMNs, polymorphonuclear neutrophils; ROS, reactive oxygen factor; TGF, tumor growth factor.
Footnotes
Author’s Note
The US government is authorized to reproduce and distribute for governmental purposes notwithstanding any copyright notation thereon. The views and conclusions contained herein are those of the author and should not be interpreted as necessarily representing policies or endorsement, either expressed or implied. Sponsors had no involvement in study design, collection, analysis, interpretation, writing, and decision to and where to submit for publication consideration.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been supported by awards from the US Air Force and ExxonMobil Foundation.