
Abstract
Planning for and managing radiological terrorism incidents that involve the release of radionuclides from a dirty bomb requires considering the potential lifesaving impact of protective radionuclide decorporation countermeasures (e.g., lung lavage). Lung lavage therapy could prevent deaths via the pulmonary mode (which involves radiation pneumonitis and fibrosis) by reducing the radiation dose to the lung from inhaled radionuclides. The risk avoidance (
INTRODUCTION
Recent terrorist actions throughout the world underscore the growing threat of radiological terrorism (DHS 2003; CDC 2005; DHHS 2009). This has stimulated research on and development of medical countermeasures for protecting humans against radiation harm, including harm resulting from use by terrorist of a radioactivity dispersal device (RDD) such as a dirty bomb.
During a radiological terrorist incident radionuclides could be inhaled (e.g., after a dirty bomb detonation). Inhaling large quantities of radionuclides could lead to lives lost among the general public from radiation-induced deterministic effects that evolve over time. Deterministic effects are threshold-type effects that include lethal damage to the lung (e.g., radiation-pneumonitis-related). The threshold dose for lethal damage varies for different individuals and depends on how dose rate changes over time (Scott and Hahn 1989). The time to deliver a lethal dose increases as dose rate decreases. For long-lived radionuclides inhaled in highly insoluble forms, the accumulation of a lethal radiation dose may require more than a year after inhaling the radioactive material. The effective management of dirty bomb incidents requires careful planning that includes considering the impact of radionuclide decorporation (removal from the body) countermeasures that could be employed to reduce the radiation dose and associated risk of harm to first responders, members of the general public, and others.
Employing lung lavage (bronchoalveolar) is a possible countermeasure to remove excess radioactivity from the respiratory tract in the case of inhalation exposure to airborne radionuclides resulting from a dirty bomb incident (Nolibé et al. 1989; Muggenburg et al. 1990; Breitenstein 2003). The removal leads to a reduction in the committed radiation dose (the dose that builds up over time) and also may reduce the risk of radiation-induced harm depending on the endpoint considered and residual radiation dose (Scott 2005). Pharmaceutical and other products are also being developed for possible employment as radioprotectors and as decorporating agents to facilitate removing radionuclides from the body after uptake into the systemic circulation. However,
The related paper (Scott 2009) introduces health risk assessment (HRA) tools that facilitate planning for and managing radiological terrorism incidents such as those that involve an RDD. The indicated HRA tools include analytical functions for evaluating the lethality risk avoidance (
The hypothetical scenarios considered in the main text involve circumstances where the low linear-energy-transfer (LET) beta/gamma radiation dose rate to the lung (critical target considered) decreases as a single, negative-exponential function of time. The single negative-exponential characterization is used for illustrative purposes to facilitate understanding of how to evaluate the lethality
METHODS
Evaluating Pulmonary Mode Lethality RAV and RAP
Lethality risks are evaluated based on the HF model (Scott 2004) using the approach described in the cited related paper (Scott 2009). For the HF model and for the pulmonary mode of death, the risk function

The pulmonary-model lethality hazard

where
The normalized dose (i.e.,

Equation 3 was developed for exposure to low LET beta and/or gamma radiation but was also applied to high-LET alpha radiation via adjusting model parameters (Scott 2007) or via using RBE-weighted dose (Scott and Peterson 2003). For the pulmonary mode of death (radiation pneumonitis and fibrosis related) and for internal low-LET beta/gamma radiation, central estimates for HF model parameters are
Analytical Solution for X for Single, Negative-Exponential-Decaying Dose Rate
The following analytical solution applies for a single negative-exponential-decaying dose-rate pattern with initial dose rate

The terms on the right-hand side of Equation 4 represent the following:

and

The function
The function
Asymptotic Solution for Normalized Dose
Over time and for a single, negative-exponential-decaying dose-rate pattern to the lung,

where:

and

The term
RESULTS AND DISCUSSION
Time Period over which Radiation Dose Should Be Evaluated
Plotting
Table 1 shows calculated values (rounded) of
Expected ratio

Values in italics that occur at
For multiple negative exponential decaying dose-rate patterns,
Evaluating Lethality Risk Avoidance due to Lung Lavage
Scenarios considered here involve a single application of lung lavage to remove a deposited radionuclide inhaled and deposited as a result of dirty bomb incident.

The normalized dose increment

For such scenarios, the initial dose rate

Please note that λ1 now replaces λ when using Equations 8 and 9 to evaluate
The total lethality risk (central estimate) without decorporation countermeasures is indicated as

The subscript
Central estimates of the lethality risk

A value of

The shape parameter value of

The corresponding equation for the

Figure 1 shows the calculated pulmonary-mode-lethality
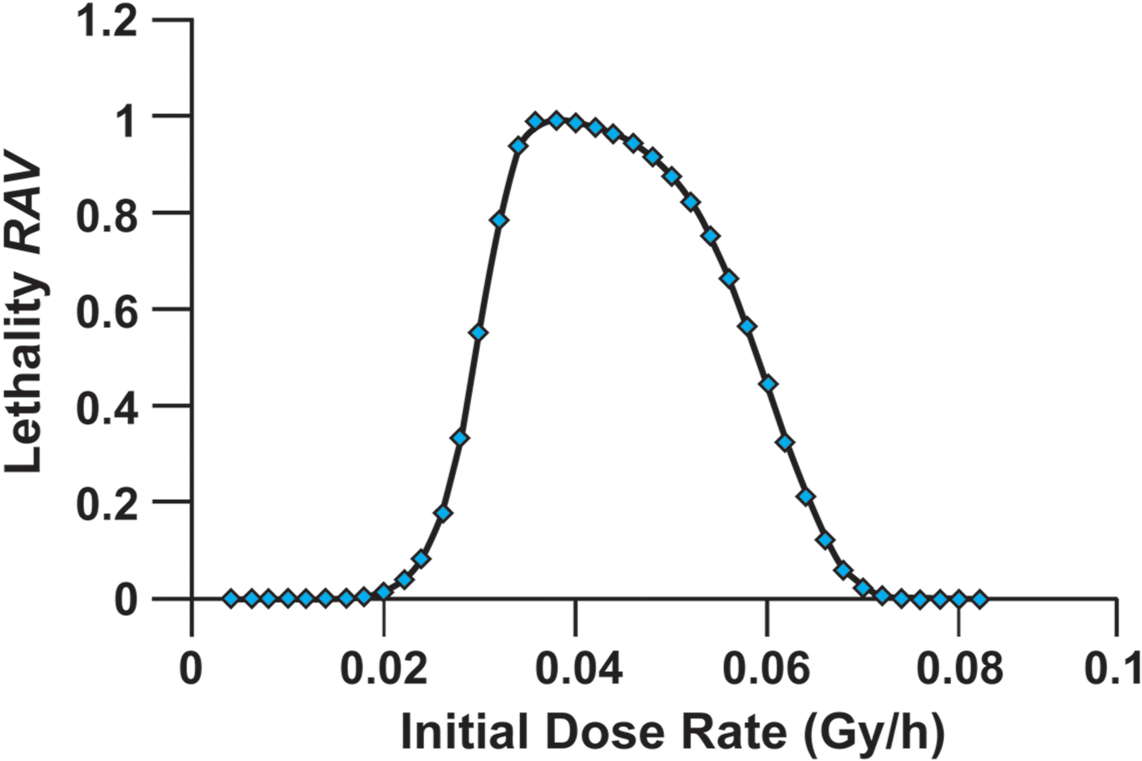
Central estimates of the pulmonary-mode-lethality
Figure 2 shows corresponding modeling results (central estimates) for the

Central estimates of the pulmonary-mode-lethality
The dose-rate (initial) boundaries for the green, yellow, and red zones will depend on the radionuclide decorporation therapy scheme and exposure scenario. When the HF-model and countermeasure-related uncertainties are considered, the boundaries will likely become blurred. Zone boundaries should therefore be considered highly uncertain; however, new research is needed to address uncertainty-related issues.
The results presented in figures and tables relate to single, negative-exponential-decaying dose-rate patterns. However, the more general relationships provided in the Appendix can be used to evaluate the lethality
Some exposure scenarios of interest may involve an initial rise in dose rate over time followed by a period of steady decreases in dose rate. For such dose-rate profiles, the increment in the normalized dose that occurs during the rising dose-rate phase could be evaluated based on taking small time increments over intervals (
The modeling framework presented here could also be applied to inhalation exposure scenarios that involve combined exposure to alpha-, beta-, and gamma-emitting radionuclides provided that absorbed dose was replaced with RBE-weighted dose. Further, competing modes of death (e.g., pulmonary, hematopoietic, and gastrointestinal) could also be included.
The research described here and also in the closely related paper (Scott 2009) is an extension of much earlier research conducted by the author. Unfortunately, support for continuing the earlier research disappeared some years ago and interest in supporting the type of theoretical/modeling research presented in these papers has not increased since that time. Unless more appreciation is develop by the scientific community and funding agencies of the important contributions that theoretical/modeling research (e.g., radionuclide biokinetics/biodistribution, dosimetry and risk modeling) can make to the advancement of scientific knowledge related to planning for and managing radiological terrorism incidents, the next generation of scientist may be devoid of essential knowledge needed for addressing the types of issues that are addressed in this paper.
CONCLUSIONS
A theoretical framework was presented for evaluating both the expected pulmonary mode lethality
Footnotes
ACKNOWLEDGMENTS
This research was supported by Lovelace Respiratory Research Institute. I am grateful to Vicki Fisher for editorial assistance and to Wendy Piper for graphics support.