
Abstract
We report a case of a porter who presented with acute dyspnea during an expedition in Nepal at 5000 m above sea level. We present the difficulties involved in making the correct diagnosis in this patient under austere conditions and discuss the difficult decisions that must be made in caring for such a patient.
Introduction
We were in Nepal as part of an expedition organized by Medex, a group that supports the work of Medical Expeditions, a research charity dedicated to investigating the mechanisms of altitude-related illness. The purpose of the expedition was to establish a temporary high-altitude medical research facility at Chamlang base camp (5000 m) (Figure 1). The expedition consisted of 60 Medex members separated into 5 teams in occasional radio contact. Each group had at least 1 medical officer (MO) and 1 chief MO. Each group brought medical equipment from the United Kingdom.
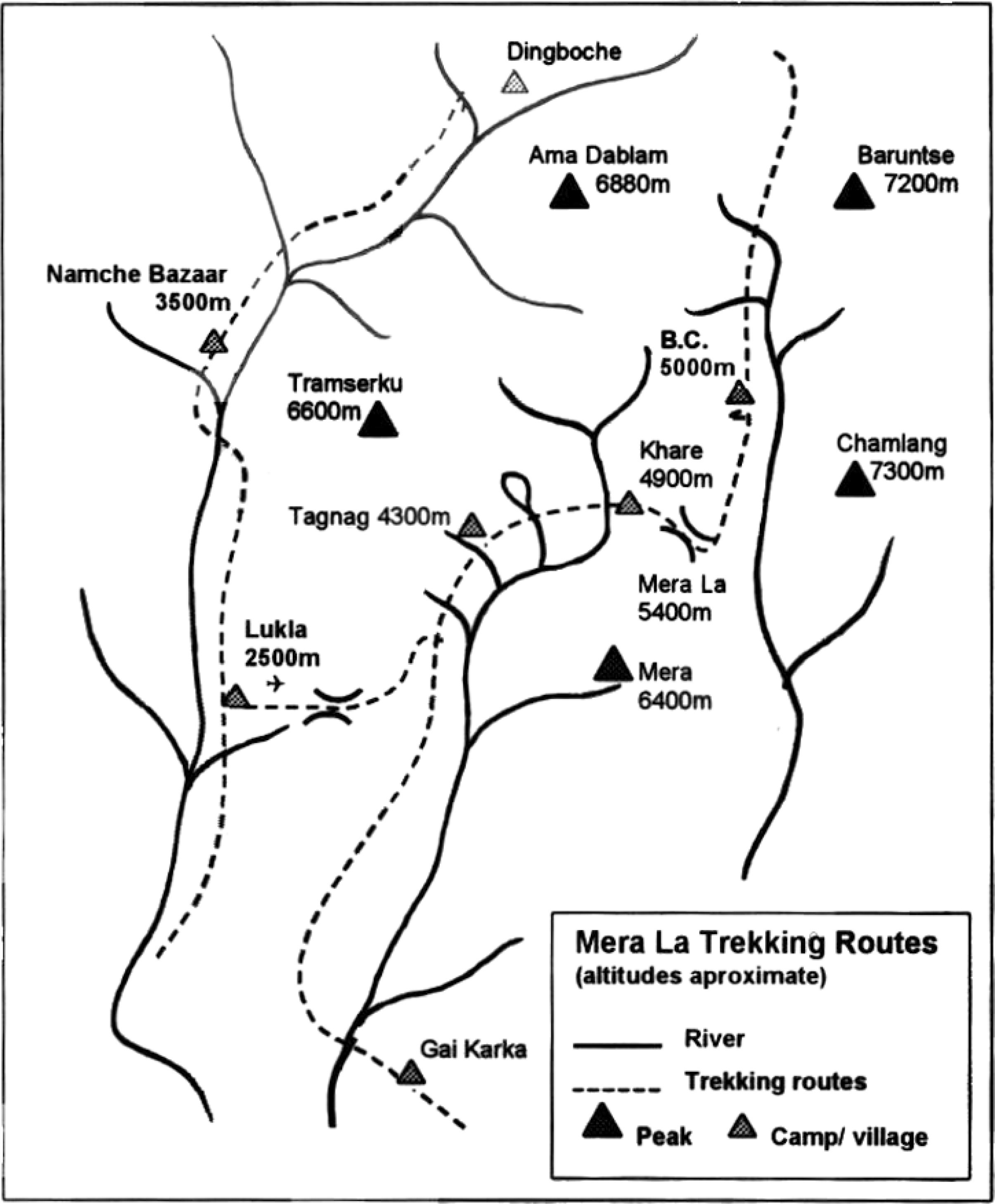
Mera La trekking routes.
A porter from the expedition became unwell near the Mera La, a high-altitude pass at 5400 m between the Hinku and the Honku valleys (Figure 2). The Honku valley, on the far side of the Mera La, is extremely remote and far from the usual trekking routes. Direct descent in the Honku valley is not possible; the only trekking route out is over the Mera La.

The Mera La.
Case report
A 32-year-old porter crossing the Mera La (5400 m) presented with a 1-day history of watery diarrhea, arthralgias, and exhaustion. He was a resident lowlander but had spent 2 weeks at base camp (5000 m) with a 4-week gradual ascent profile. He was previously healthy with no known existing medical conditions. Following the MO's advice, the porter's colleagues immediately carried him down to Khare (4900 m). He arrived at Khare 3 hours later in the early evening and was seen immediately by 2 of the expedition MOs. The smoke-filled hut was dark, crowded, and poorly lit, and the air temperature was 4°C.
Via a translator, the porter complained of a “problem with his breathing.” He felt breathless but had no pain. His cough produced a small amount of yellow sputum. He looked unwell, was hot to the touch, and was mildly dehydrated. He was tachypneic at 40 breaths/min and tachycardic at 140 beats/min and had an arterial oxygen saturation (Sa
The diagnosis was lobar pneumonia and possible tuberculosis. Intravenous access was secured, and the porter was given 500 mL normal saline, 500 mL Hartman's solution, 1 g intravenous ceftriaxone, and 1.2 g intravenous Augmentin (amoxicillin/clavulanate) as well as 500 mg oral azithromycin. There was little immediate response to this treatment. Fortunately, a respiratory physiotherapist was part of the trekking party at Khare (Figure 3). Physiotherapy did not initially result in sputum production, but a cough response was evoked, which, with the low flow oxygen, raised the porter's Sa

Physiotherapy by flashlight.
Despite the time of night and the difficult terrain anticipated, another descent was advised. The porter was carried down an additional 600 m to Tagnag (4300 m) that same night to be received by more members of the expedition. His intolerance of the facemask prevented continuation of oxygen overnight. A Canadian respiratory physiotherapist, who was not a member of the expedition, was staying at the lower camp and provided physiotherapy the next morning that resulted in the production of 0.5 L of bloodstained purulent sputum.
A total of 3 doses of intravenous ceftriaxone was administered with a course of oral Augmentin and azithromycin. Because of the amount of pus expectorated, flucloxacillin was added to cover the possibility of a staphylococcal lung abscess. The porter continued twice-daily physiotherapy for 3 days, producing yellow sputum from the right upper and middle lobes. He made a remarkable clinical improvement within 24 hours upon arriving at Tagnag and was able to remain with the expedition until its end in Lukla (2500 m) 4 days later. His last measured Sa
Clinical Diagnoses and Decision-Making Processes
Dyspnea at high altitude should be considered to be high-altitude pulmonary edema (HAPE) until proven otherwise. However, the clinical findings in this case were not consistent with HAPE, and additional treatment for HAPE with vasodilators could have worsened the patient's condition.
The patient was a resident lowlander but had been symptom free during a 4-week gradual ascent to and 2-week stay at 5200 m. After a further ascent of just 200 m to the pass and with no improvement upon descent, it was therefore improbable that his clinical condition had resulted from HAPE.
A diagnosis of pneumonia was made, and the patient was treated with physiotherapy, intravenous fluids, oxygen, and antimicrobials. This is in keeping with more pragmatic advice that although HAPE should be considered in the differential diagnosis of dyspnea at altitude, other conditions occur and should be recognized and treated accordingly. 1
The choice of antimicrobials was limited by availability but was still appropriate, with amoxicillin and clavulanate added for anaerobic coverage.2,3 Because tuberculosis is endemic in the region, the upper lobe signs in this patient presented a high probability of underlying tuberculosis.
The options available to increase inspired P
Review of treatment options at high altitude
Oxygenation at High Altitude
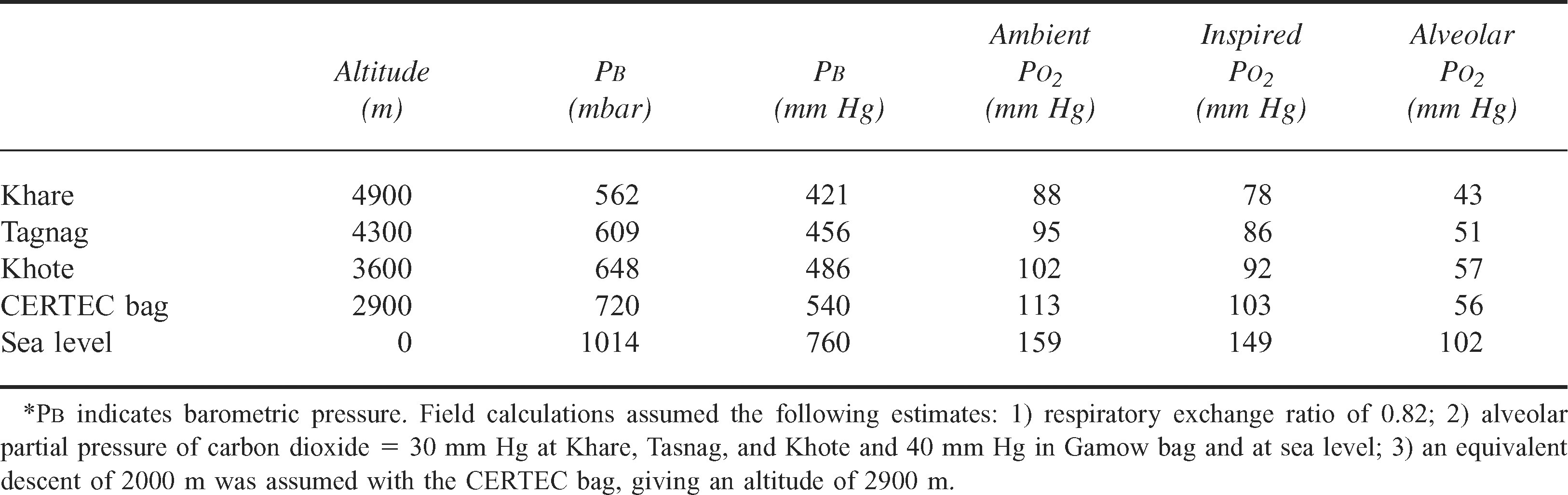
Physiologists in the expedition group used a range of assumptions to calculate ambient P
The fractional concentration of oxygen (F
This was in addition to the ventilation-perfusion ratio mismatch and increased alveolar-pulmonary capillary diffusion distance associated with lobar pneumonia imposed on a background global pulmonary hypoxic vasoconstriction. This resulted in a dramatic reduction in Sa
We recognize that such calculations are often impractical (Table) and accordingly suggest the carriage of a laminated card showing the oxygen dissociation curve and alveolar gas values for use in such situations. Refer to Pickard 5 (table 2.5, page 34) for a useful example.
With an estimated P
Comparison of estimated oxygen tensions according to altitude and within a hyperbaric bag*
Hyperbaric Oxygen Therapy
Since its introduction in 1989, 6 portable hyperbaric therapy with Gamow or CERTEC bags has been used effectively to treat acute mountain sickness (AMS). 7 –9 The concurrent use of supplemental oxygen is not recommended. The bags are pumped to a pressure of 104 or 165 mm Hg, respectively. The equivalent descent depends upon the current altitude but is between 2000 and 2500 m. Such therapy is a temporary measure for use only when descent is impossible or as a holding measure while means to effect an immediate descent are established.
Randomized studies on patients with AMS have compared the use of hyperbaric therapy, or simulated descent, with either bed rest, 7 dexamethasone, 8 or oxygen. 9 Results confirmed that hyperbaric therapy is an effective acute therapy for AMS but with no long-term effect.
There are no published data on the use of portable hyperbaric therapy at altitude for conditions other than AMS, HAPE, or high-altitude cerebral edema. Increasing the P
However, a hyperbaric bag would have limited our access to the patient, potentially reducing his functional residual capacity with him lying flat and increasing the work of breathing while decreasing oxygenation. Monitoring the patient would have been more difficult, and postural choice would have been restricted. The experience would have been stressful to the patient because of a lack of familiarity and confidence exacerbated by cultural differences and would have required a constant operator pumping effort to maintain pressure and air renewal. Also, the benefit of increasing P
Evacuation
Helicopter evacuation from the Honku valley is difficult if not impossible; the lowest pass into the valley is 5410 m, which may be impassable by helicopter in certain weather conditions. Because of political instability in Nepal at the time of this case report, it was possible that no helicopter would have been available for medical evacuation, and any available helicopter may have taken up to 48 hours or more to arrive. The cost would have been covered by the expedition's insurance policy.
Descent
Descent was favored as the treatment of choice for a number of reasons. First, the patient's P
Discussion: the challenges of expedition medicine
Diagnosis and Treatment of Disease in the Wilderness
At very high altitude (3500–5800 m), the Sa
Thorough predeparture planning meant the expedition group was well equipped with a large range of pharmaceuticals. The CIWEC Clinic Travel Medicine Centre 12 in Kathmandu updated the group with information of antibiotic resistance to local infections. Each team had oxygen; intravenous fluids; a stethoscope; a sphygmomanometer; an otoscope and ophthalmoscope; a wide range of oral and intravenous antibiotics, including a third-generation cephalosporin; and all medications required for the treatment of altitude-related disorders. As part of the research, each team had a reliable oxygen pulse-oximeter (Nonin, Onyx). Although sourced oxygen from the United Kingdom was available, it could not be transported to Nepal because regulations enacted after the Gulf War restricted commercial airlines that could freight oxygen cylinders. A supply of oxygen cylinders was found in Kathmandu, although they were of doubtful provenance.
Most commercial organizations who plan treks to these regions and use a similar number of local staff that we used should not expect to be so thoroughly medically staffed or equipped; our MOs had experience or training in expedition and altitude medicine, and having a physiotherapist and 2 physiologists in the group was a rare luxury. Should the patient in this case report have been so unwell with a less well-equipped and experienced group, his outcome may not have been as favorable. Many westerners traveling to such environments are deeply unaware of the real potential for life-threatening illness and the general lack of medical provision available. 13
Ethical Decision Making
The expedition MOs had agreed on a working philosophy before leaving the United Kingdom: while individual trekkers retained their own responsibility for routine health care matters, we would provide any necessary urgent or emergency medical treatment for all Medex members and anyone employed locally on our behalf for the duration of the trip.
That we had a duty of care to our porters in the acute event was unarguable. 14 But where does the duty of care end? The loss of contact with the porter upon arrival in Lukla was a cause of concern. His compliance with oral therapy became poor once his clinical condition improved, and we were dependent upon translators to emphasize the need to continue the course of antibiotics. His noncompliance represents one of the cultural differences encountered, and as he was not portering he had no source of income, so his main priority was to return to work.
Having made the diagnosis of a possible cavitating lung lesion or tuberculosis, we felt an obligation to arrange further investigation. Given the possibility of open tuberculosis, we had been advised that the porter would not be allowed to travel to Kathmandu by air. The other route to Kathmandu involves a 4-day walk and a 12-hour bus ride. Once the porter was paid, we lost contact with him and could offer him no further advice. This was despite frequent discussions with him via our sirdar and discussions with the local MO at Lukla. We sent a message asking that the porter seek follow-up treatment at the Himalayan Trust hospital at Khunde, a 1-day walk from Lukla.
Conclusion
Expedition or wilderness medicine is increasingly recognized as a specialty in its own right, with the first UK Diploma of Mountain Medicine having started in 2003. Many doctors work on treks to remote mountainous regions, either formally as part of an expedition or informally while on vacation. Concerns have been raised about the training and lack of experience of many of these doctors acting in such a capacity. 14 This case report highlights many of the difficulties of managing an acutely ill patient in the wilderness by a well-resourced experienced team. We hope it will emphasize the risks of adventure travel to both prospective tourists and doctors who offer their services in the wilderness.
Footnotes
Acknowledgments
We thank Tracey Hughes, Will Sargent, and Simon Currin.