
Abstract
C. Raymond Greene (1901–1982) was a man of many talents. After graduating from medical school in 1927, he spent a decade in general practice. He subsequently became heavily involved in the emerging specialty of endocrinology and went on to gain considerable recognition in the treatment of thyroid disorders before eventually becoming involved in the world of medical publishing. Aside from Greene's mainstream vocational and intellectual pursuits, from boyhood he nurtured a passionate interest in mountaineering—first in his native Great Britain, and then the European Alps, and ultimately in the high Himalayas. His involvement in landmark climbs, such as the successful Kamet venture in 1931 and Everest attempt in 1933, earned him a place in the pantheon of Himalayan explorers and mountaineers and stimulated Green's interest in high altitude physiology and medicine. He made notable additions to the literature on this subject in publications such as Nature and Journal of Physiology. Apart from his remarkable life achievements in the areas of medicine, mountaineering, and publishing, Greene was perhaps best remembered by those close to him (and by contemporary readers who are devotees of his writing) as a peerless storyteller with a sardonic sense of irony.
Introduction
C. Raymond Greene (1901–1982) (see Figure 1) was a brother of 2 well-known characters—Graham Greene, famous novelist, and Sir Hugh Greene, former Director General of the British Broadcasting Corporation. Perhaps not surprisingly, Raymond was a man of many gifts. The eldest son of a distinguished family, he won a scholarship to Pembroke College (University of Oxford) and went on to obtain a degree in medicine. Upon graduating in 1927, he practiced family medicine for 10 years before moving into the emerging specialty of endocrinology. He subsequently went on to gain considerable recognition in the treatment of thyroid disorders. Later in his clinical career, he became involved in the world of publishing and ultimately became chairman of Heinemann Medical Books. This article will briefly explore Raymond's multifaceted life and times. Special emphasis will be given to his contributions at the intersection of science, medicine, and mountaineering.
Portrait of Raymond Greene from the mid-1920s.
Background
There is little doubt that Graham, well known for authoring many critically acclaimed novels, became the most widely celebrated of the renowned Greene brothers. However, Raymond, 3 years Graham's senior, was perhaps the most academically and athletically gifted of them all. In Sherry's comprehensive biography of Graham Greene, Raymond is characterized as a man who possessed extraordinary talents. Of his formative years, Sherry wrote, “It is probable that Graham's failure, where physical prowess was concerned, was exacerbated by the fact that his elder brother Raymond was such a success at school, seemingly in all that he attempted … He [Raymond] was an ardent debater, but also a successful editor of The Berkhamstedian … Even in a field where you would think his presence and forcefulness would not aid him—poetry—he succeeded in winning the school's Arnold Medal … .”
1
In 1925, Graham commented: I used to have an absurd competition complex with Raymond. Raymond used to write and publish in the School Magazine, and win school prizes for verse. So I had to write too. I never succeeded in winning any prizes for verse … [Raymond] stopped writing verse directly when I began to get mine published, and his was much more promising. Then his new tack became adventure, and he became a first class mountaineer.
2
Nonetheless, perhaps it is not surprising to learn that the principal impression Raymond left with many people throughout his life was of an excellent storyteller with a wry—and sometimes notorious—sense of irony.
Alongside his working life, Greene developed a passionate interest for mountains and mountain medicine. As a boy, Raymond climbed and walked in the English Lake District and, when at Oxford, he became a member of the Oxford University Mountaineering Club. This association encouraged him to look for climbing challenges abroad and he made regular visits to the German and Austrian Alps throughout the 1920s. His first visit to the Himalayas, and introduction to the medical problems of high altitude, was as a climbing team member and medical officer on Frank Smythe's 1931 expedition to Kamet (7756 m). Kamet is an impressive peak situated in the Zanskar Range of the Indian Garhwal Himalaya, lying directly on the Indian-Tibetan border approximately 70 km as the crow flies to the northwest of the more famous mountain named Nanda Devi (7816 m). The expedition completed the first ascent of the mountain by climbing the northeast edge of the north face via the East Kamet Glacier and Meade's Col. This was notable for 2 reasons: not only was it the ninth attempt on the mountain but, at the time, it was the highest mountain to have ever been climbed in its entirety (ie, higher actual altitudes had been reached on Everest attempts in the previous decade, though the summit had not been achieved). Greene was among those who reached the summit, and his performance on Kamet went some distance towards earning him a place on Hugh Ruttledge's 1933 Mount Everest expedition. His contribution as climber and physician on Everest was, once again, of tremendous value to such a lengthy Himalayan venture.
Kamet 1931
The first ascent of Kamet in 1931, via the eastern approach of Meade's Col route, was a notable episode in Himalayan mountaineering history. To the upcoming generation of extreme altitude climbers on the Kamet team (Figure 2), it proved an ideal opportunity to gain experience in this hostile environment. Smythe led a strong party consisting of 6 Europeans and 10 Sherpas, many of whom had gathered considerable experience on Everest and Kangchenjunga. By June 21, 1931, Smythe, B.R. Holdsworth, E. Shipton, and Sherpas Lewa and Nima Dorje set out for the summit from a camp situated on a large snowfield just below Meade's Col. At 7620 m, Nima Dorje, who had been entrusted to carry a rather cumbersome cine camera, became too exhausted to continue. Lewa took his load, and the remaining 4 climbers reached the summit at 4:15 pm. They descended without incident through snow softened by the afternoon sun. Two days later, Raymond Greene, J. Birnie, and the local porter Kesar Singh successfully repeated the climb to the summit. The first ascent of Kamet has been described extensively in Frank Smythe's popular classic, Kamet Conquered. 3 This book has often been reprinted, and is included in a recently published anthology of Smythe's work. 4
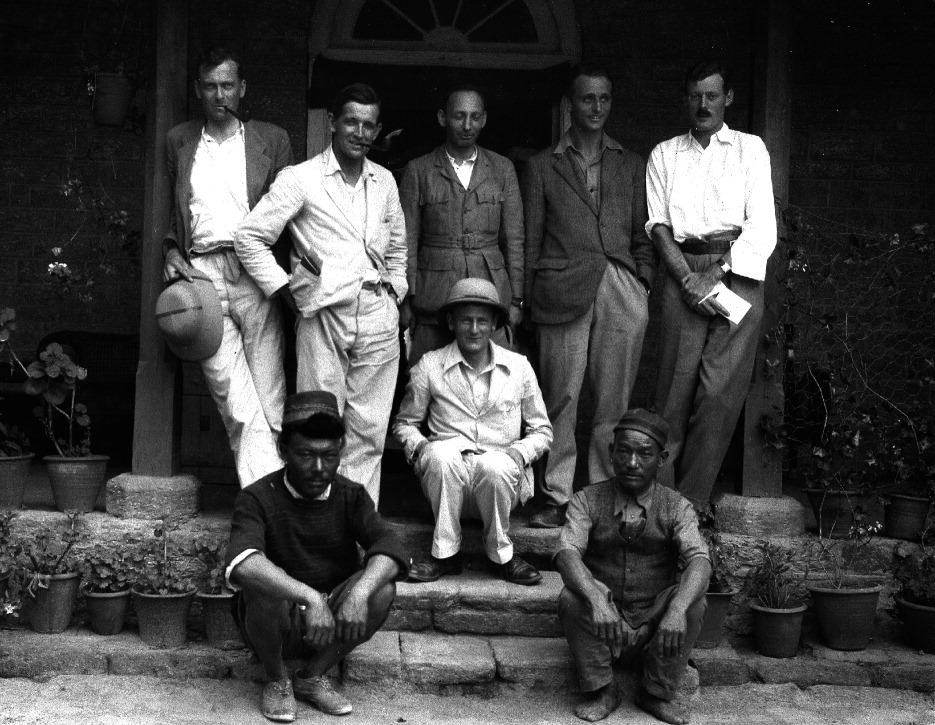
1931 Kamet expedition team members: (Front) Nima Tendrup and Achung. (Back) Greene, Holdsworth, Beauman, Shipton, Birnie, Smythe (seated in center).
The 1931 Kamet climb was not without a considerable amount of medical drama. During the march back to civilization, Frank Smythe developed an agonizing toothache. After several days of suffering, he asked Greene to extract the tooth. In Greene's autobiography, Moments of Being,
5
he wrote: I gave Frank a shot (of morphine) and left him to carve a dental prop out of a juniper root. When I returned I found him unduly cheerful: to give himself Dutch courage he had consumed more than half a bottle of rum. I extracted the tooth, and Frank, after one screamed expletive, passed into oblivion. We carried him to his tent at about six in the evening and he slept quietly until I retired to my tent at about nine o'clock. At about two in the morning I was awakened by a curious noise and, emerging in pyjamas only in a temperature well below zero Fahrenheit I found that Frank's head was protruding from the flap of his tent, his neck supported by one of the ties … When I rescued him from this predicament he stopped breathing. I gave him artificial respiration but every time I rested for a moment he stopped again. After 2 h, spontaneous breathing returned. Luckily the hard exercise involved prevented me from freezing solid.
Firth and Pattinson 6 provide an analysis of this life-threatening event. However, given Greene's description, citing an exact cause is unrealistic. Nevertheless, we do know that alcohol in large doses is a potent sedative and is capable of exacerbating breathing disorders during sleep through impairment of the chemical drive of respiration. 7 It is thus possible that “heavy sedation and subsequent airway obstruction, compounded by disruption of chemical drive by alcohol and possibly, the residual effects of morphine, may have all contributed to [Smythe's] breathing difficulties.” 6
One can only speculate upon the contribution of altitude-induced nocturnal periodic breathing to a medical phenomenon such as this. However, it is not inconceivable that this may have exacerbated the situation somewhat if Smythe was in fact already experiencing cyclic episodes of central apnea during sleep.
The next time Greene was called upon to perform dental extractions in the field was during the march across Tibet on the 1933 British Mount Everest expedition. Greene's involvement with this expedition will be discussed in some detail later. However, it is worth recalling that, for dental anesthesia, Greene used only a “sup of whiskey” for the local porters and villagers. 8 Fortunately, Ruttledge reported that these hardy Tibetans were “sublimely indifferent to the absence of an anaesthetic.” 8 It is not known whether Greene's previous experience on Kamet had influenced his parsimonious approach to pain control on subsequent occasions at altitude!
Greene wrote a chapter on the “Medical Aspects of High Climbing” in Smythe's 1932 expedition book, Kamet Conquered,
3
and also contributed a short article to the journal Nature titled “Oxygen and Everest.”
9
These allowed Greene to discuss a number of medical and physiological issues. In particular, Greene touched upon a matter much discussed but little understood at the time—namely, the balance between high altitude acclimatization and altitude-related deterioration. Although there was virtually no data available at the time to strongly support opinions on this issue, Greene was a keen observer and had a reasonable amount of anecdotal evidence to draw upon. He rightly recognized that there is a balance between acclimatization and deterioration, and optimal climbing performance was to be had by achieving that balance through shrewd timing of movements high on the mountain. Greene concluded: It is probable that many … factors may enter into the problem. I hope that by stimulating controversy I may be instrumental in bringing some to light. The importance of the subject to climbers is great. I have pointed out elsewhere that the question of the climbing of Everest depends upon the opposing factors of acclimatization and deterioration.
3
Everest 1933
Shortly after the Kamet team returned to Great Britain in 1931, preparations were afoot for another expedition to Everest in 1933, and Raymond was chosen to participate as climber and chief medical officer. Hugh Ruttledge was to lead this venture, and the team of 14 included 4 of the Kamet team: Smythe, Birnie, Shipton, and Greene. Although Raymond was working long hours as a general practitioner in Oxford, he was able to find time to do physiological work, albeit with considerable risks, in preparation for the expedition. “He consulted leading physiologists Haldane, Douglas, and Priestley, and spent many hours in a low-pressure chamber at Oxford, suffering agonizing earache and some days of deafness when a careless technician “crashed” him from a simulated 20 000 feet (approximately 6100 m) to earth (sea level) in a few seconds.” 1 (Greene also describes this incident on pages 148–149 in Moments of Being 5 ).
Despite this difficulty, he was able to conclude that a climber's ascent should average on the order of 1000 feet (approximately 300 m) per day, 5 with acclimatization “stops” as necessary at various camps as one ascends. This thinking, or versions of it, has been the basis of recommendations for conservative ascent profiles in the mountaineering world ever since—particularly as a means of avoiding altitude-related illness.
Greene also found time to improve the design and function of the supplementary oxygen kit for climbing at extreme altitudes on Everest. The original oxygen kit for Everest, first used in 1922 (frame and charged cylinders), had weighed approximately 15 kg (33 pounds). The engineering skill of George Mallory's climbing partner on Everest, Andrew “Sandy” Irvine, had reduced this to about 10 kg (22 pounds) by 1924. However, by 1932, it had been decided that the oxygen kit needed to be lighter still and should weigh no more than 6.2 kg (13.6 pounds). Building on Irvine's earlier work, Greene carried out further alterations for the 1933 attempt. By removing the carrying frame and limiting each apparatus to just one bottle of oxygen (each bottle holding 500 L of compressed gas and weighing 4.9 kg (10.8 pounds) when full), the device now weighed just 5.8 kg (12.75 pounds). At the 2 to 2.5 L/min flow rate used with the 1933 apparatus, 10 one 500 L bottle would last approximately 4 hours. So, while the 1933 oxygen kit was certainly lighter than its predecessors, it must be remembered that the 1924 version was designed to be used with 2 or 3 cylinders of gas carried on the frame—with each cylinder having a capacity of 535 L of compressed oxygen. Thus, the 1933 apparatus saved weight, but only at the distinct expense of supplemental oxygen availability.
The combination of poor weather and the expedition's bias against supplementary oxygen meant that opportunities to use the device were limited during the 1933 attempt. In fact, the apparatus never received a proper trial on the mountain. Somewhat surprisingly, it had been decided prior to the expedition that oxygen should be used only if attempts to reach the summit without it had failed. At the end of the “unoxygenated” attempts, the weather deteriorated and the condition of the snow had become dangerous. The party retreated to Base Camp to await better conditions, leaving most of the oxygen apparatus at Camp IV. Unfortunately, the better conditions never came. 10
The 1933 Everest expedition also provided Greene with an opportunity for physiological field research. During the 1924 attempt on the mountain, Howard Somervell had “attempted to obtain samples of alveolar air from members of the climbing party at elevations as high as 23,000 feet [approximately 7000 m]. Unfortunately, he collected his samples in rubber bags and there was long delay before the analyses could be done. That a great deal of CO2 had diffused out through the rubber in the interval is evident not only from the extremely small concentration of CO2 found in the samples but also from the abnormally low respiratory quotients that he records.” 11
Given the less-than-satisfactory results of Somervell's study, Greene thought that it would be worthwhile to once again attempt to obtain alveolar air samples on Everest (in 1933). He believed that by using a somewhat different technique, the results might prove more acceptable than those of his predecessor. Despite Greene's best-laid sea-level plans, this experiment was difficult to execute. In the end, Greene “was only able to obtain a few samples of alveolar air, all from myself whilst at rest, but I believe that these afford a reasonably satisfactory index of the composition of the alveolar air in an acclimatized person at the altitude of approximately 23,000 feet [approximately 7000 m].” 11
The methodology for this collection in 1933 was an improvement over that used in 1924. Air samples were collected in evacuated glass tubes that were “sealed in a flame on the spot” and transported back to the United Kingdom for analysis. This novel field technique for collection and transport of alveolar air samples was a definite leap forward, methodologically speaking. It was still a method successfully used by medical scientists decades later as, for example, during the well-known 1960–1961 Silver Hut physiological research program in the Himalayas. Greene's findings at 23 000 feet (approximately 7000 m, with a barometric pressure of 339 millimeters mercury [mm Hg]) showed a resting alveolar CO2 concentration of 19.3 mm Hg and a resting alveolar oxygen concentration of 38.8 mm Hg (with a respiratory quotient of 0.83). These results suggest Greene's gas collection techniques and study methodology were sound, given today's accepted values for alveolar partial pressure of oxygen (PO2) and partial pressure of carbon dioxide (PCO2) at this altitude. Evidence for this can be seen, for instance, on the well-known Rahn-Otis diagram included in West's history of high altitude physiology and medicine, High Life. 12
Greene's contributions to the 1933 Everest attempt were actually far more wide-ranging than just helping to design an improved supplementary oxygen circuit or collecting alveolar air samples. As scientist, climber, and senior medical officer, he was also involved in a number of other important events during the expedition. During the approach march across the Tibetan plateau, a Tibetan porter, Lobsang Tsering, suffered a fractured clavicle after falling off of his pony. Hugh Ruttledge related that “It was decided to give Lobsang an anaesthetic and set the bone at once. Greene is an expert anaesthetist, and no difficulty was expected. But anaesthetics, it seems, can play queer tricks at over 14,000 ft. [approximately 4260 m].” 8
Greene no doubt recalled his prior experience with post-anesthesia ventilatory depression in Frank Smythe in 1931 and, therefore, gave Lobsang a very small dose of inhaled anesthetic vapor. He later recorded: In camp I gave [Lobsang] a mere breath of chloroform while Willy reduced the fracture. Suddenly heart and lungs stopped acting simultaneously. I filled a syringe with Coramine [a theophylline derivative no longer in common use], struck for the heart and began external cardiac massage while Willy applied artificial respiration [this was most likely not cardiopulmonary resuscitation, or CPR, as we know it today, as chest compressions were not formally described until 1960,
13
with “modern” CPR techniques following some years later]. Lobsang's heart began to beat again and respiration returned.
5
This sudden cardiopulmonary arrest may well have been induced by chloroform. Cardiac arrhythmia under chloroform anesthesia has been well-documented.14,15 Importantly, it should also be realized that “using the open drop technique, Greene had no way of precisely assessing the inspired concentration of anaesthetic.” 6 While we realize it is impossible to establish the primary physiological “event” in this case of cardiopulmonary arrest, Greene summed up his clinical impressions by saying “Within an hour [Lobsang] was smoking a cigarette. I don't know which part of our treatment worked but I've had a weakness for Coramine ever since.” 5
Greene's thoughts had apparently also turned to ventilatory stimulation of a prophylactic nature during preparations for Everest. In 1932, at the suggestion of the famous respiratory physiologist John Scott Haldane, Greene had undertaken a series of experiments in order to examine whether ammonium chloride increased the work capacity at low barometric pressures. 16 These studies, conducted in a hypobaric chamber at Oxford University, were positive, and Greene followed this up with field observation on Everest the following year. With logic that foreshadowed the use of acetazolamide to prophylax or treat mountain sickness decades later, Greene wrote that, with the administration of ammonium chloride, “… one increases the ventilation of the lungs by increasing the acidity of the blood passing through the respiratory centre in the brain.” 8 Although the trials with ammonium chloride on Everest in 1933 were less than satisfactory because of the inability of many climbers to tolerate the substance, it was also used with mixed results on other pre-World War II (WWII) Himalayan mountaineering expeditions. Perhaps the most notable subsequent use of ammonium chloride (during this era) was on the ill-fated 1939 American K2 attempt. 17
As Greene was along on the 1933 expedition as a climber as well as a physician, it comes as no surprise that adventures of the alpine variety also presented themselves during the course of this attempt on Everest. In mid-May, as the expedition was starting to make progress on the upper part of the mountain, a lengthy storm struck the team. In advanced base camp (Camp III) on the East Rongbuk Glacier, some of the climbers who camped at this relatively low altitude considered themselves in a protected position from the onslaught of the weather. Unfortunately, they were mistaken. In Greene's tongue-in-cheek style, he wrote: We lay in the comfortable arctic tent like pips in a gigantic cantaloupe. In the evening the hurricane returned … At two o'clock there was a resounding crash and the side of the tent fell in. Longland, who had very virtuously insisted on sleeping in his own leaky Meade tent to leave more room for the rest of us, slept on undisturbed. The remaining four of us sat up and looked at one another with a wild surmise. We knew that if we could not erect the tent again it was the end of us. In such cold and in such a gale survival would have been impossible. With no word spoken, Wager and I climbed out into the night. … The wind was so strong that we could hardly stand. Knee-high for me, shoulder-high for the shorter Wager, a thick layer of driven snow raced horizontally, so that only his head was visible, apparently decapitated. All the guys of the tent had given way, but after an hour they were replaced and the tent was secure though lop-sided.
5
As the 1933 team pushed the route higher, other altitude-related problems arose. After Camp V was established at 25 700 feet (approximately 7830 m) on the North Ridge, Greene, Harris, Boustead, and Birnie had planned to continue on the following day to set up Camp VI. Unfortunately, Greene had climbed to altitude considerably faster than the others and suffered from the effects of his rapid ascent. Forced to descend with a group of porters to the North Col (Camp IV), the ailing Greene was unable to keep up and was soon left behind. Many years later, he vividly related an account of the descent, hinting at the dangers of exhaustion at extreme altitude and just how easy it can be to sit and rest at high altitude only to never get up again: The going was easy to a trained mountaineer, scrambling over rocks about as easy as the Crib Goch ridge on Snowdon, interspersed with patches of snow. But I was a sick man. In every patch of snow I fell over and rested a while. At last in a very comfortable spot, sheltered from the howling wind, I decided that I had had enough. I was warm and comfortable and the view was superb. If I stayed where I was I would fall comfortably asleep. I had no wife or children for whom I could feel responsible: my parents had five other children and, though I knew they would mourn, they would lose only a small proportion of their offspring. I decided to stay … [and then although] I do not recall any [conscious] effort, suddenly I was struggling downwards again, falling again in every patch of snow, but rising at once when breath returned. Then below me were the tents of Camp IV bright green against the snow.
5
Like Norton in 1924, the 1933 Everest expedition stalled at an altitude of about 28 200 feet (approximately 8600 m). Despite subsequent expeditions to Everest in 1936 and 1938, none managed to go higher. None of the pre-WWII attempts made serious use of supplementary oxygen after 1924, which begs the question as to whether full-on oxygen-aided attempts during these years might have fared better. Even a romantic purist such as Frank Smythe (member of the 1933, 1936, and 1938 attempts) recognized that “Those who tread its [Everest's] last 1,000 feet [approximately 300 m] tread the physical limits of the world.”
8
Oxygen advocate George Ingle Finch, one of the leading climbers of the 1922 effort on Everest, was incensed by the non-use of gas on the mountain after the 1933 failure:
18
This wretched state of indecision about oxygen must be ended, and in good time, too, if the next expedition is to succeed. Either oxygen should be taken and used full blast in the attack above 25 000 feet [approximately 7600 m] or even above 23 000 feet [approximately 7000 m], or it should be utterly tabooed on moral or material grounds, or indeed for any other reason that the wit of man can conceive. And if the prospective Everest committee cannot bring itself to decide one way or the other then sack the lot!
Not until the early 1950s did Everest expeditions make an effort to seriously and systematically integrate supplemental oxygen into their climbing strategies.
Later Medical Career and Other Pursuits
In 1937, Raymond Greene moved from family medicine to the emerging specialty of endocrinology and became a Clinical Assistant at the Westminster Hospital. After the Second World War, he joined the staff of several other London-area hospitals, but his name became primarily associated with the New End Hospital, Hampstead, where, with Sir Geoffrey Keynes, he developed a thyroid clinic that achieved world renown. Greene later wrote what could be termed a “popular science” text titled Human Hormones.
19
In his typical style, that usually displayed more than just a hint of facetiousness—or, as one anonymous writer termed it, “a wry sense of friendly irony,” he captured the essence of a medical specialty in its formative stages: Endocrinology as a branch of medicine has had a troublesome career. A mere half-century ago it was not quite respectable. Too many smart-alicks within and without the medical profession were, with great perspicacity but little knowledge, beginning to climb on to the band wagon … The failure of orthodox doctors was largely due to the fact that endocrinology was a new science. Not much was known by the most learned. The less learned fell back on speculation and romance: “the glands of destiny”, “we are governed by our glands”, “I don't know what is wrong – it must be something glandular”, were phrases commonly heard. It was a quack's paradise, but so obviously so that in many hospitals physicians interested in endocrinology were looked upon askance.
19
Notable, too, was his appointment as a Hunterian Professor of the Royal College of Surgeons of England, especially so as a physician. He had made a distinct mark on the burgeoning field of endocrinology over the years, as both a practitioner and a medical scientist. A search of PubMed lists over 70 endocrine-related publications that contain his name. A later accomplishment came in the form of the Chairmanship of Heinemann Medical Books.
Raymond Greene's medical interests in his later career were not limited to endocrinology, however. After his personal involvement in high altitude medicine in the 1930s, he continued to maintain a strong interest in environmentally oriented medical problems. During the early years of the Second World War, it became obvious there was a great need for scientifically based investigations in the area of environmental physiology and medicine. Stimulated by the practical problems he faced with cold injury in the Himalayas, Greene's investigations produced an article in a 1943 issue of the Journal of Pathology and Bacteriology titled “The Immediate Vascular Changes in True Frostbite.” 20 In addition, during WWII Greene had significant contact with the British military, in particular the mountain troops and the Special Operations Executive (SOE). A significant post-war honor that came his way as a result of his association with the SOE was Chevalier of the Legion of Honor presented by French leader Charles de Gaulle.
Never one to let increasing medical specialization limit his widespread interests, Greene produced a paper later in his career entitled “Mental Performance in Chronic Anoxia” for the British Medical Journal.
21
This article, in a style laced with wit that had become Greene's own, largely concerned itself with the hypoxia of high altitude and the psychological stress that can be manifest in many individuals under such circumstances. Greene did not miss an opportunity, however, to bring his observations into the clinical realm. Using patients with chronic cardiopulmonary disease as an example, he anecdotally captured the problem in an elegant fashion that cut straight to the heart of the matter: My own impression is that in the chronic anoxia of cardiac failure and advanced pulmonary disease one sees an accentuation of a previous mental abnormality rather than the creation of a new one. The man one has known for years as a well-balanced, placid, good-tempered, co-operative patient retains these characteristics in a state of chronic anoxia due to illness. One feels that one of the effects of the illness is to strip the veneer off a man and expose the quality of his mind naked to the world. I think that the same thing happens in alcoholic intoxication and in the chronic anoxia of great altitudes.
21
Conclusions
Raymond Greene's contribution to mountaineering and medicine was wide-ranging and considerable. It can be argued that, in the arena of high altitude mountaineering, his combination of enthusiasm and intelligence was particularly invaluable. Not only was he able to be of direct help to those around him in the realm of medicine and mountaineering, but he was also able to make a difference in the wider world of contemporary medical thought through his writings. In addition, Greene's influence has been keenly felt by those who have subsequently followed in his footsteps.