
Abstract
Objective
As competition climbing becomes increasingly popular, younger climbers are entering the sport, and some are among the top-level athletes. This early start combined with intensive training methods can lead to radiographic changes in the fingers and even osteoarthrosis. Since 1994, we have been observing an increasing number of nontraumatic epiphyseal fractures in young athletes.
Methods
Twenty-four cases of young climbers with nontraumatic epiphyseal fractures of the finger middle joints are presented.
Results
The average age of the climbers was 14.5 (±0.9) years; 23 were boys, and 1 was a girl. Eight (33%) fractures were in an early stage, whereas in 16 (67%) a longer time interval elapsed between the onset of symptoms and the presentation for evaluation. All radiographs showed an epiphyseal fracture of the dorsal base of the middle phalanx of the finger; 20 patients presented a Salter-Harris III fracture and 4 presented a Salter-Harris II epiphysiolysis. An acute injury was not evident in any of the patients. All fractures were thus fatigue fractures caused by repetitive stress.
Conclusions
Chronic finger pain in young and intensively training climbers must be carefully evaluated, and radiographic studies need to be performed. The risk of epiphyseal injuries must be minimized by eliminating intensive power training in the schedules of athletes of this age.
Introduction
The increasing popularity of sport climbing has caused younger climbers to enter it, and they have progressed to levels on par with top competitive athletes. It is no longer unusual for 16-year-old climbers to be in the finals of a World Cup or climb in grades as high as 5.14. With this high-level performance, the training becomes more and more intensive, and even maximum-power training methods are being used although the climbers are in an age group where their skeletal growth still continues. In 1997, we reported nontraumatic epiphyseal fractures (fatigue fractures) in 5 climbers (mean age 13.6 years) for the first time. 1 Chell et al 2 presented a 15-year-old climber with bilateral epiphysiolysis and no trauma. Over the following years, we observed an increasing number of cases 3 in our work with the German Junior National Team and served as a reference center for climbing injuries. In a study of radiographic changes in the fingers of young top-level climbers, only climbers who did intensive maximum finger strength training—for example, Campusboard training (feet-free climbing on an overhanging board, including double-dynamic moves)—demonstrated osteoarthrotic changes as a consequence of neglected epiphyseal fractures. 4 In this study, we describe our experience evaluating and managing a series of young climbers with epiphyseal injuries to their fingers.
Methods
Description of 24 young climbers with epiphyseal stress fractures of their fingers*
Results
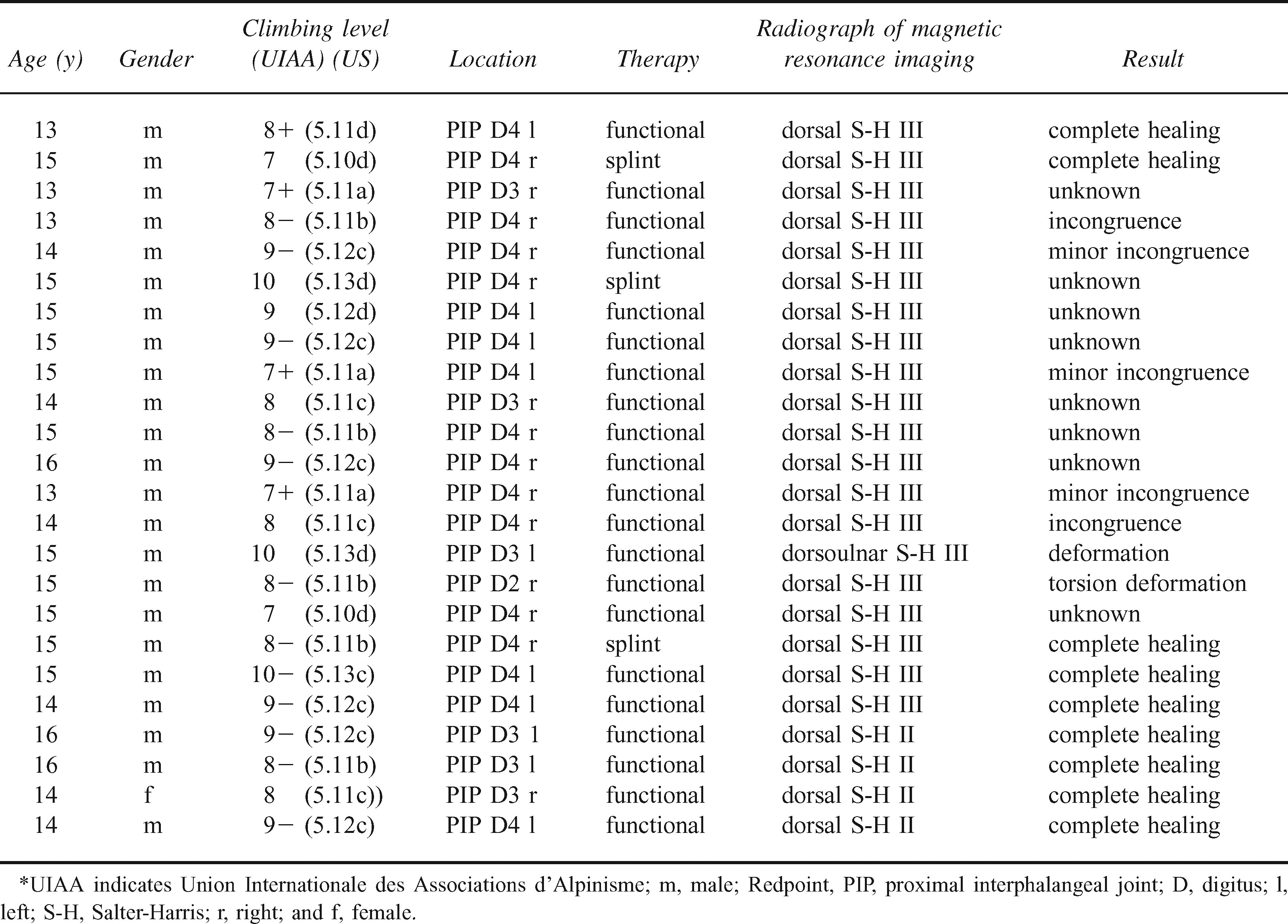
The average age of the climbers was 14.5 (±0.9) years (Table); 23 were boys, and 1 was a girl. Eight (33%) of the climbers presented with a short history of symptoms, whereas 16 (67%) contacted us after a longer interval after the onset of complaints. A single traumatic event was not evident in any patient. All patients reported a slow onset of pain in the finger middle joint in addition to swelling and sometimes complained of a reduced range of motion. Clinical examination showed swelling of the finger middle joint, tenderness on the dorsal side of the base of the middle phalanx, and in most cases a reduced range of motion of the finger middle joint (extension/flexion: 70–10–0°). All radiographs showed an epiphyseal lesion of the dorsal base of the finger middle phalanx. In 20 patients this was a Salter-Harris III fracture (Figures 1 and 2), and in 4 patients it was a suspected Salter-Harris II epiphysiolysis. The results of the additional magnetic resonance imaging in those patients with suspected Salter-Harris II epiphysiolysis demonstrated more impressive findings than did the normal radiographs (Figures 3 and 4). T1 sequences showed a complete signal eradication of the whole epiphysis, and T2 sequences demonstrated intra-articular effusion in the proximal interphalangeal joint.

Fifteen-year-old climber with a Salter-Harris III lesion.

Clinical picture of the patient in Figure 3. Note the axial deviation.
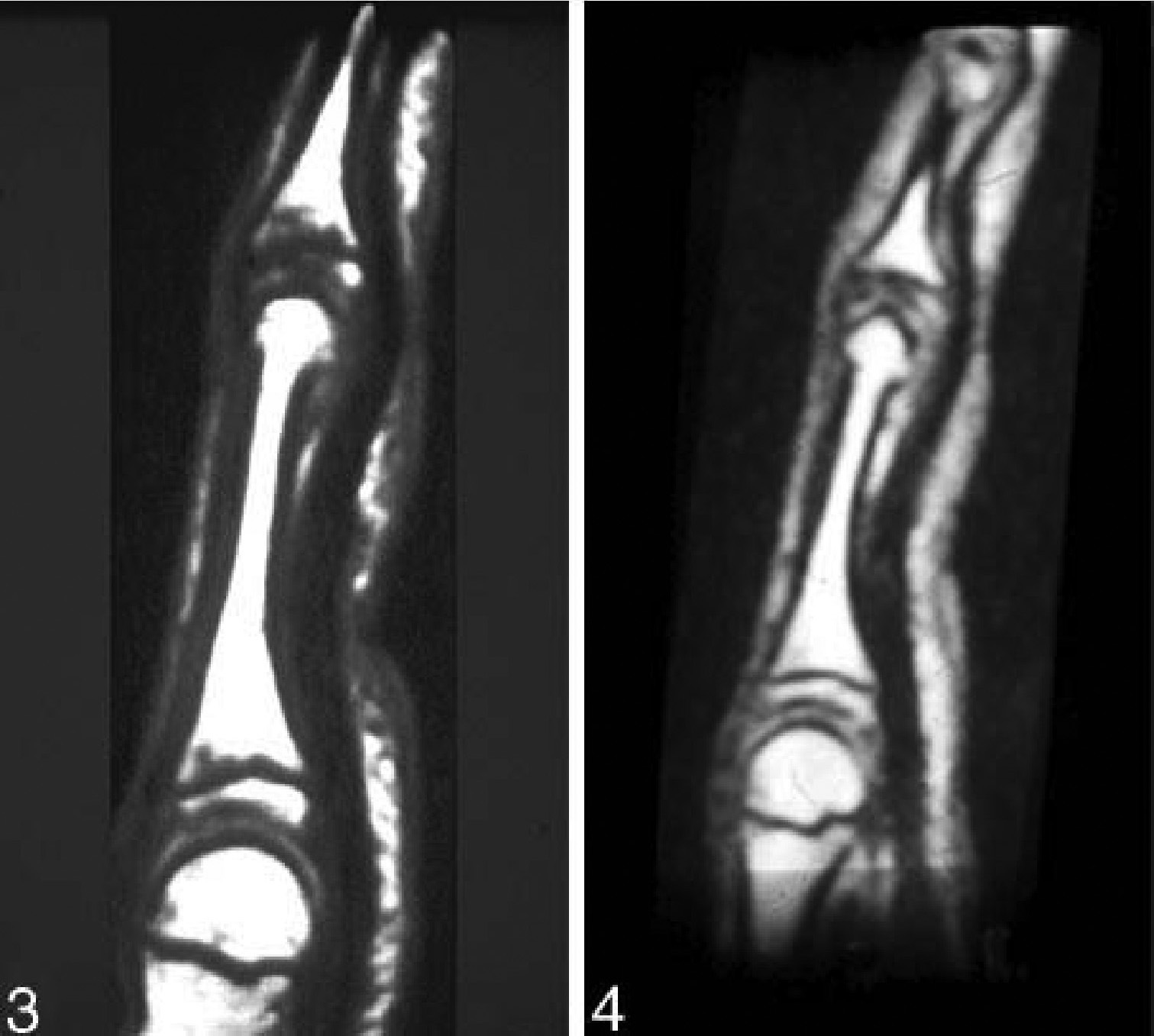
Magnetic resonance images (T1 and T2) of an early stage of epiphysiolysis. The conventional radiographs demonstrated no pathology. The T1 sequence clearly demonstrates a reduced signal of the epiphysis of the proximal interphalangeal joint in comparison with the MCP joint. The T2 image shows intra-articular effusion in the proximal interphalangeal joint.
The 8 patients with a short interval between the onset of complaints and the start of therapy showed good therapeutic results with initial splinting and a complete stop of climbing until radiographic consolidation had occurred. In most patients, a complete regeneration of the epiphysis evolved. The radiographs of the 16 patients with a longer history of symptoms before therapy demonstrated a more prominent dislocation of the epiphysis. This included minor- to middle-grade incongruence of the dorsal base of the middle phalanx—a prearthrotic deformity. We treated those patients with Salter-Harris II lesions functionally with a climbing-free interval of 3 months. In all 4 patients, the follow-up magnetic resonance imaging showed complete healing, and the signal loss in the T1 sequences was gone. Also, the follow-up radiographs showed completely normal findings. Two patients with a longer history of symptoms had very poor outcomes when they disregarded our recommendations to rest and continued to climb at a high level. This resulted in an ulnar deviation within the proximal interphalangeal joint of 15° within 12 weeks. Radiographs showed partial necrosis of the epiphysis in these patients (Figure 5).

Devastating result of 1 of the 2 climbers who continued climbing despite our advice.
Discussion
All climbers were between 13 and 16 years of age. One reason for the male predominance of these injuries might be the change in the body weight:strength ratio in this age group. Boys tend to gain more body weight than do girls. To compensate for this weight gain (which is a handicap for their climbing performance) in comparison with their strength, they tend to increase their training for more finger strength. All boys in this study were performing maximum-power training on small edges by using the crimping position. This finger position, especially combined with Campusboard training, is a method that has proven to be a high risk for finger injuries and overuse syndromes. 5 –7 Also, evidence shows that the increased testosterone output during puberty in boys weakens the mechanical stability of the epiphysis.8,9
It is interesting to note that none of the climbers reported any acute trauma. All these fractures must thus be considered as fatigue fractures caused by repetitive stress and microtrauma. A possible mechanism would be chronic microfractures of the dorsal part of the epiphysis, because the highest pressure peaks appear there, when the middle joint is in a flexed position. It appears that the epiphysis is more prone to injuries in the state of growth where it starts to close up.
In other sport disciplines, such high-impact training methods are not performed in this age group, and climbing should be no exception. In a study comparing German Junior National Climbing Team members with recreational climbers, we found radiological changes consistent with early osteoarthrosis in only 2 climbers (1 of each group). 4 Both of these climbers were using Campusboard training. In analyzing the training methods in both groups, only 3 climbers were using Campusboard training, and 2 of them had already developed epiphyseal stress fractures. 4 Although we had good results with conservative treatment in those patients who presented early, the results were worse in those with a longer interval between the onset of symptoms and the start of therapy. In such patients and in patients with further displacement of the fractured epiphysis, a surgical approach with open reduction and fixation might be required.
Conclusions
Chronic finger pain in young, intensively training climbers must be carefully evaluated, and radiographs should be performed. To minimize the risk of epiphyseal injuries, intensive, maximum-power training in these age groups should be avoided. These guidelines are already being adopted: The Medical Commission of the Union Internationale des Associations d’Alpinisme has stated that international boulder competitions have become limited to climbers above the age of 15. 10
Footnotes
Acknowledgments
The authors wish to thank Isabelle Roloff for English language support.