
Abstract
Introduction
The aim of this study was to evaluate different grip positions as a contributing factor for primary periphyseal stress injuries of the finger phalanges in climbing.
Methods
Ultrasound imaging of the proximal interphalangeal joint was performed on 37 asymptomatic adolescent climbers. Longitudinal images were obtained of middle and ring fingers of both hands in different grip positions (open, half-open, and crimp), unloaded and loaded. The translation between the dorsal head of the proximal phalanx and the shaft of the middle phalanx was measured in an unloaded and loaded situation for all grip positions. The resulting difference was determined as the palmar shift.
Results
The mean age of the study population was 13 y. Results showed a palmar shift of 0.57 mm in a loaded crimp grip position compared to 0.13 mm in an open position and 0.20 mm in a half-open grip position. With a P value of <0.001, this shift was significantly higher in a crimp grip position compared to open or half-open grip positions.
Conclusions
This leads to an increase in joint incongruity and much higher peak forces on the dorsal aspect of the epiphyseal-physeal-metaphyseal complex, which is particularly vulnerable during the adolescent growth spurt. Thus, climbing and training behavior should be adapted accordingly during this phase by avoiding the crimp grip position until epiphyseal fusion.
Introduction
In recent years, sport climbing has become increasingly popular not only on a recreational but also on a competitive level. 1 In 2021 the sport had its Olympic debut in Tokyo and has officially been confirmed by the International Olympic Committee as part of the Olympic program for Paris 2024 and Los Angeles 2028.2,3 With an average age of 25 y (range=18–37) among the Olympic participants, most of these top-level athletes are still rather young and started climbing at an early age.3,4 Training and performing at such a high level naturally increases the risk of injury, with epiphyseal stress fractures of the finger phalanges being the most common injury among adolescent climbers. 5 -7 The use of small holds in difficult climbs leads to very high loads on the finger joints compared to those experienced in other elite sports. 8 Depending on the size and shape of the climbing hold, different grip positions can be used, which are vastly classified into open, half-open, and crimp grip positions (Figure 1). The crimp grip position is thought to play a major role in climbing-specific finger injuries due to the forced maximum flexion (>90°) of the proximal interphalangeal (PIP) joint and has repeatedly been described as the main injury mechanism for pulley ruptures. 9 -11 This may also be true for epiphyseal injuries, with the PIP joint being the most common target site for this type of injury.12,13 However, the biomechanics of the crimp grip position have not yet been studied in detail in adolescent climbers with open growth plates.
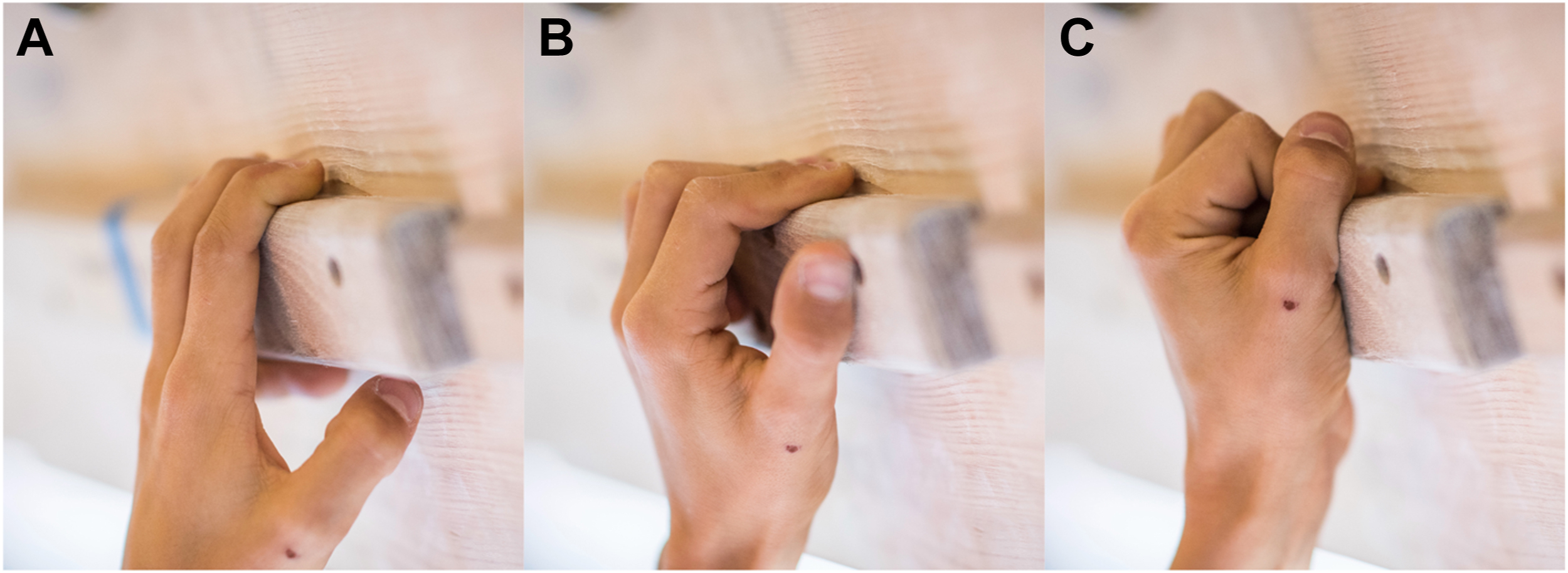
A, Open grip position with fully extended (0–30°) PIP joint and partially flexed DIP joint. B, Half-open grip position with partially flexed (60–90°) PIP joint and extended DIP joint. C, Crimp grip position with fully flexed (>90°) PIP joint and hyperextended DIP joint. DIP, distal interphalangeal; PIP, proximal interphalangeal.
The aim of the present study was to determine and understand the effect of different grip positions on a potential palmar shift of the middle phalanx in relation to the proximal phalanx. As previously suggested by the senior author of this paper, 14 we assume that this palmar shift results in a joint incongruity, which leads to a peak load on the dorsal part of the epiphyseal-physeal-metaphyseal (EPM) complex.
Methods
Study Population
All participants of the annual national Testing Day held by Swiss Climbing were recruited for this study. Included were healthy athletes between 11 and 18 y of age. Written parental consent was obtained from all participants. Exclusion criteria were lack of written consent or acute injuries causing pain during the examination.
Study Design
Ultrasound imaging of the dorsal aspect of the PIP joint was performed on the middle and ring fingers of both hands since this is the most common target site for epiphyseal injuries. 12 A GE LOGIQ e system ultrasound machine was used with the transducer (L8-18i-RS) being placed in a longitudinal direction on the dorsal aspect of the joint with the support of a three-dimensional (3D) printed positioning device. Imaging was performed on each finger using open, half-open, and crimp grips in an unloaded and loaded position (Figure 2). For the loaded positions, participants were asked to pull on a 20-mm campus edge with most of their body weight still on the ground. The amount of loading was neither measured nor standardized. All subjects underwent imaging once by the same author. The distance between the dorsal aspect of the head of the proximal phalanx and the dorsal corticalis of the shaft of the middle phalanx was measured in unloaded and loaded positions for each grip position. To determine the palmar shift, the difference between the unloaded and loaded measurements was obtained (Figure 3). The measurements were independently taken twice by 2 different authors of this paper to minimize the effect of measurement error.
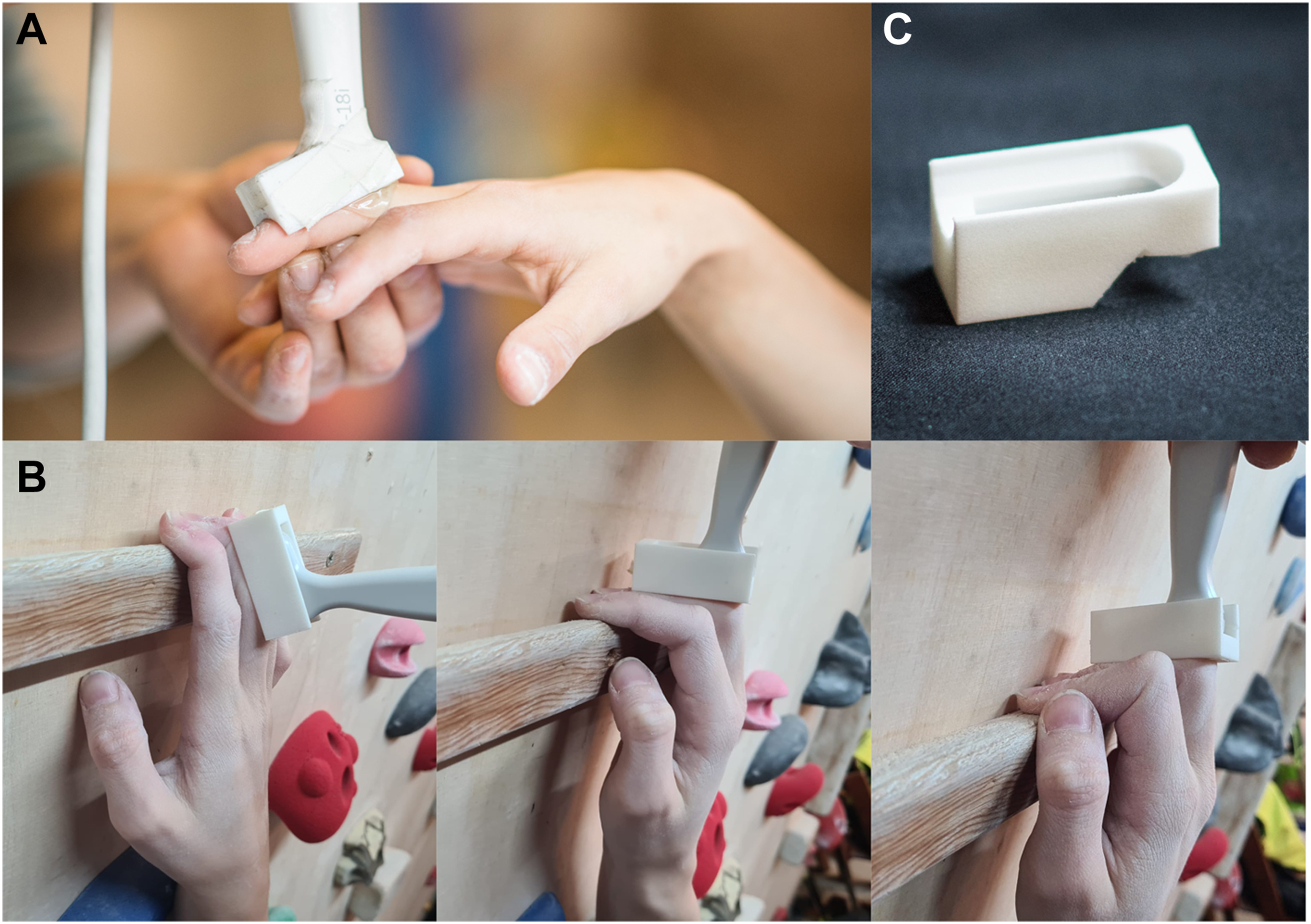
A, Probe placement for longitudinal ultrasound imaging of the PIP joint of the middle finger in an unloaded open-hand grip position. B, Probe placement for longitudinal ultrasound imaging of the PIP joint of the middle finger in loaded open-hand, half-open, and crimp grip positions. C, 3D printed positioning device. 3D, three-dimensional; PIP, proximal interphalangeal.

A, Ultrasound imaging of the palmar shift in a crimp grip position. B, Ultrasound imaging of the palmar shift in an open-hand grip position.
Statistical Analysis
A statistical analysis of the palmar shift was performed using paired sample t-tests (P<0.001) for grip position (open, half-open, and crimp), side (right and left), and digit (Dig III and IV). Measurement consistency between examiners was assessed using intraclass correlation based on a two-way random effects model assessing the absolute agreement of a single-measure approach. Intraclass correlation coefficient values were classified as poor (≤0.2), fair (0.21–0.4), moderate (0.41–0.6), good (0.61–0.8), and very good (>0.8). 15
Ethical Approval
Approval for this study was granted by the Cantonal Ethics Committee of Zurich, Stampfenbachstrasse 121/Postfach, 8090 Zurich (BASEC-Nr. 2017-00893).
Results
A total of 42 athletes were recruited, out of whom 5 athletes had to be excluded due to injury. Imaging was performed on the remaining 37 subjects (22 females, 15 males), resulting in 888 images of 148 different joints. The age of the participants was 13.3 y (range=11–16, SD=1.6). In 5 patients, the epiphyseal growth plate was already fused, the youngest being a 13-y-old female. The average palmar shift between middle and proximal phalanx in a loaded crimp grip position was 0.57 mm compared to 0.20 mm in a half-open position and 0.13 mm in an open grip position for both examiners (Figure 4). With a P value of <0.001, this shift was significantly higher in a crimp grip position compared to open or half-open grip positions. In the open or half-open grip position, no significant difference was found between loaded and unloaded positions. Comparison between middle and ring fingers as well as right and left hand showed no significant difference in palmar shift. Intraclass correlation between examiners was classified as good (intraclass correlation coefficient=0.77).
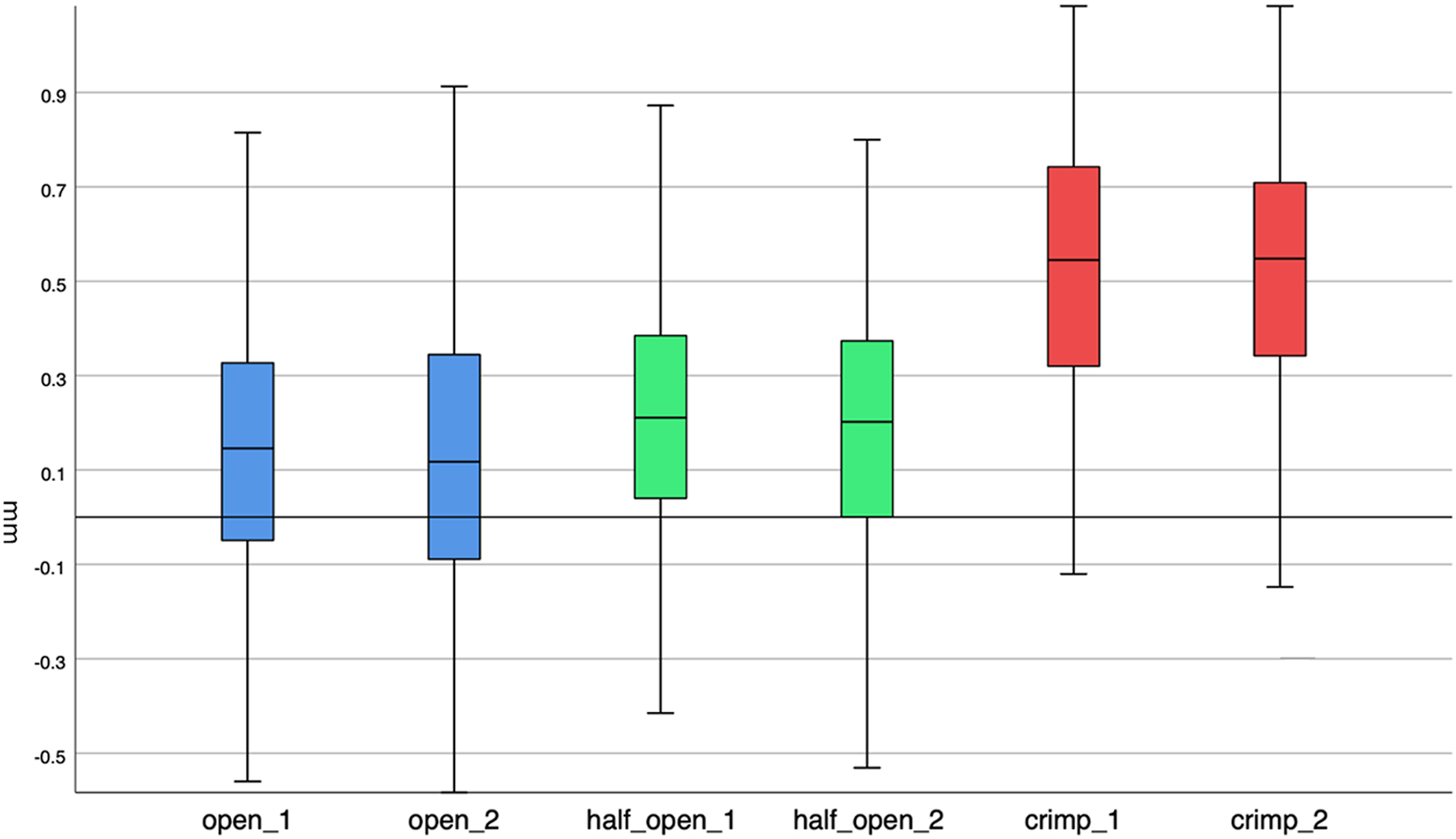
Palmar shift in different grip positions for both examiners (1 and 2).
Discussion
Pathomechanism
The dorsal aspect of the EPM complex is a common target for injuries in adolescent climbers. 13 The majority of reported epiphyseal injuries occurred without a single traumatic event and are therefore considered a stress reaction caused by repetitive overload and microtrauma.12,13,16,17 In an attempt for a more standard use of terminology, these types of injuries are now referred to as primary periphyseal stress injuries (PPSIs). 18 High compressive forces on the dorsal aspect of the PIP joint have been found using the crimp grip position, 7 which has been described by various authors as a risk factor for PPSI.2,12,13,16 Our results show that the average palmar shift is 3 times higher in a loaded crimp grip position compared to an open or a half-open position. This translation inevitably leads to joint decentralization, and based on a theoretical 3D calculation, the primary contact area (78 mm2) is reduced to less than a third (23 mm2). As previously suggested by the literature, 7 using this grip position in climbing leads to much higher peak forces on the dorsal part of the EPM complex (Figure 5). Due to high activity of the epiphyseal growth plate during the adolescent growth spurt, this part of the joint is particularly vulnerable and therefore prone to injury during heavy loading. 19 All subjects in our study with closed growth plates were females, although there was an even distribution of age in both sexes. This finding is in accordance with the literature indicating that cessation of growth occurs earlier in females due to the difference in estrogen levels during adolescence. 20 However, this distribution is hardly representative in such a small study population, and overall, there were more female subjects included in the study, which leads to a sex bias.
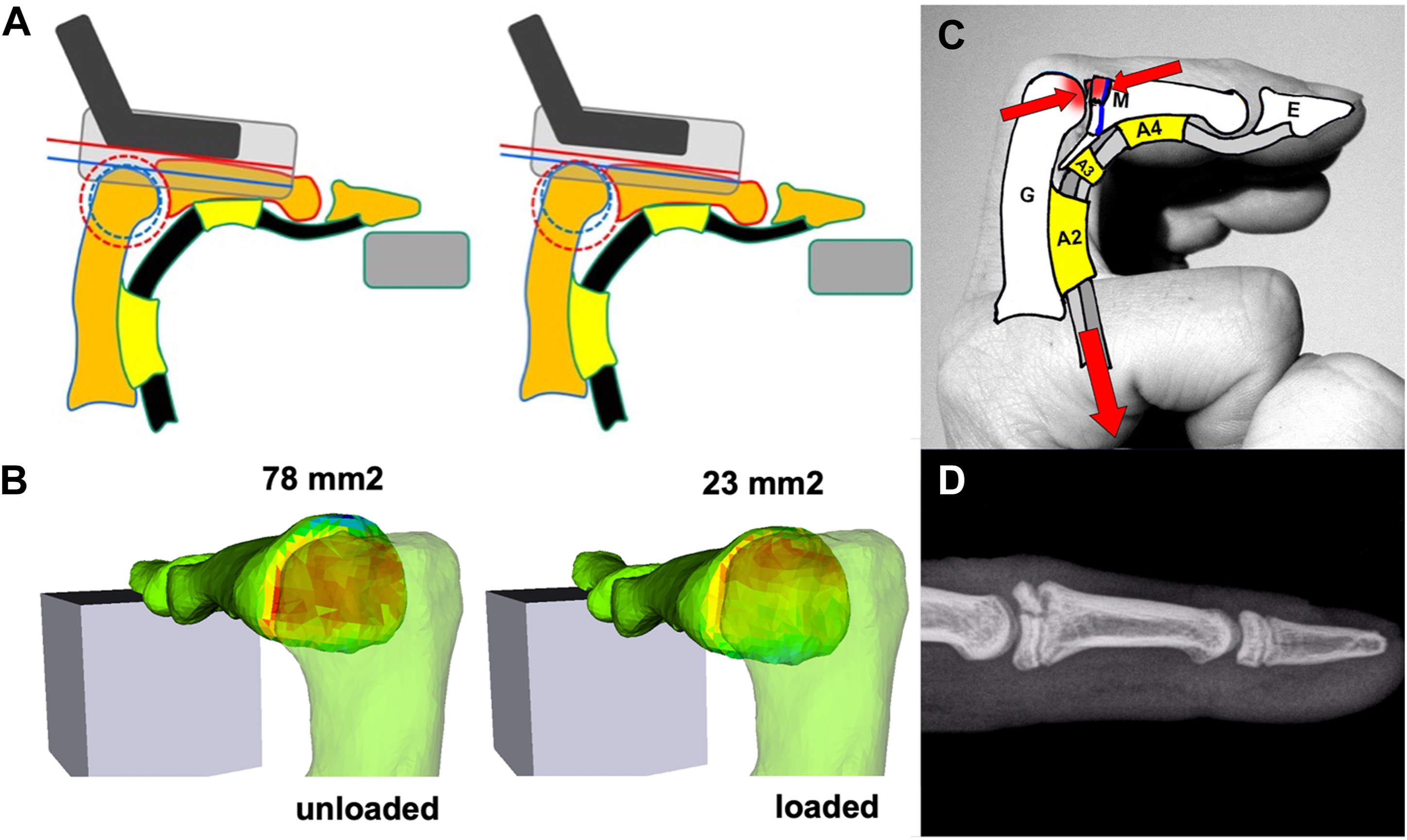
Palmar shift: difference between the unloaded and loaded measurements, resulting in decentralization of joint (A) and reduction of the joint contact area (B). C, Kinematics of the crimp grip position leading to peak forces on the dorsal part of the epiphysis, which may end up in an epiphyseal stress fracture (D).
Clinical Implication
To prevent this type of injury, climbing and training habits should be adjusted accordingly by avoiding the crimp grip position during the adolescent growth spurt, ideally until epiphyseal fusion. In accordance with the literature, a multitude of PPSIs were provoked during bouldering competitions, 7 and it has been recommended repeatedly to limit competitive bouldering to adult athletes. 21 With bouldering being included in the Olympic Games, athletes tend to compete in this discipline from an early age, and such a limitation seems highly unlikely. Since our study showed no concerns with using open or half-open grip positions, a more feasible approach would be through adjustments in route setting, as previously suggested by various authors.4,7 Particularly, the use of appropriate holds, which do not necessarily require a crimp grip position, could help in the primary prevention of PPSI. Systematic training in open or half-open grip positions using body weight or less could be a safe way to improve finger strength and induce tissue adaption, which could potentially decrease the risk of finger injuries in the long term. However, specific finger strength exercises in adolescent climbers need to be assessed carefully with respect to the fitness level and biological age of the individual. Regarding secondary prevention, atraumatic finger pain around the PIP joint in youth climbers needs to be taken seriously, and an evaluation by an experienced physician is recommended at an early stage. 12 Although not suitable for the diagnosis of PPSI, ultrasound imaging could be used as an easily applicable tool in high-level athletes to monitor the process of epiphyseal fusion in the finger joints. It should be noted however that even after epiphyseal fusion, the crimp grip position remains a risk factor for other finger injuries, 8 and systematic finger strength training should be implemented gradually over a longer period to allow for tissue adaptions and therefore avoid injuries.
Biomechanics
From a biomechanical point of view, our results support the idea that the PIP joint cannot be considered as a hinge joint. Research suggests that there is a physiological incongruity of the articular surfaces allowing for 3D movements with several degrees of freedom. 22 According to our findings, the applied load to the distal phalanges results in a palmar shift, increasing this incongruity. Another article found that during full flexion of the PIP, there was a dorsal shift of the area of contact, 23 which correlates with an increased load on the dorsal EPM complex we found during crimp grip position. Unfortunately, our methodology does not allow an exact quantification of the acting forces on the joint, partially because we did not take into consideration the plasticity of the cartilage. However, this could be an interesting topic for further exploration in future research projects.
Limitations
Several limitations of the study should be noted. First, there is high observer variability in performing ultrasound imaging as well as in measuring the palmar shift. Second, our loaded measurements were performed with most of the athlete’s body weight still on the ground; therefore, we cannot issue a general statement about the safety of different grip positions at full body weight. Additionally, loaded measurements were not standardized and therefore vary across study participants. Lastly, due to the small study population, further research effort in a larger study population is required.
Conclusions
The crimp grip position showed a significantly higher palmar shift of the middle phalanx compared to that with half-open and open grip positions. Therefore, the crimp grip leads to more joint incongruity and higher loading of the dorsal aspect of the EPM complex, posing a risk for PPSI. No difference in palmar shift was found in open compared to half-open grip positions, concluding that these grip positions should be preferred in adolescent climbers. These findings do not suffice to give out a general recommendation for finger training in adolescents. To evaluate the safety of certain grip positions in climbing during epiphyseal growth, more studies need to be performed using full body weight and preferably different shapes and sizes of holds.
Footnotes
Previous Presentation
The preliminary results of this study have been orally presented at the 4th International Rock Climbing Research Congress by IRCRA in Chamonix (France).
Acknowledgments
The authors thank Tobias Götschi for statistical advisory and Alannah Yip for proofreading the manuscript as well as the Swiss Alpine Club for providing the opportunity to acquire the data.
Author Contributions: study concept and design (AS); data acquisition (NB, AS); data analysis (NB, A-GS); drafting (NB) and critical revision of the manuscript (AS, A-GS); and approval of final manuscript (NB, A-GS, AS).
Financial/Material Support: None.
Disclosures: None.