
Abstract
We describe a case report of a subject suffering high-altitude cerebral and pulmonary edema successfully treated with low flow rates of supplemental oxygen administered with a breathing system designed to conserve oxygen supplies at high altitude.
The 2 principal types of oxygen delivery systems used at altitude are nasal prongs and face masks with an attached reservoir bag (nonrebreathing system). Nasal prongs are typically used at night with an oxygen delivery rate of 1 L·min−1. This delivery system is wasteful because most of the gas is vented into the atmosphere. Nonrebreathing systems, which are frequently used for climbing at extreme altitude (eg, Poisk, St Petersburg, Russia), are based on a reservoir bag. They deliver oxygen more efficiently because fresh gas is stored during expiration in a flexible reservoir for subsequent use. Oxygen is still wasted in the dead space, but the main problem is dilution of oxygen with ambient air. As ventilation increases above the flow rate of supplied oxygen, the inhaled-oxygen concentrations fall.
These problems have been largely overcome in a novel partial rebreathing circuit based on principles designed by Fisher and colleagues.
1
The Fisher circuit contains a reservoir where ambient air and oxygen from a cylinder mix in a fixed proportion. Oxygen in the respiratory dead space is expired into the reservoir bag for gas exchange in the next breath. Because oxygen-enriched air is supplied throughout inspiration, a lower oxygen flow rate can be used. This system has been shown to deliver oxygen more efficiently than can either the Poisk circuit or nasal prongs.
2
The only other high-efficiency circuit available has recently been introduced by Summit Oxygen Limited (Epping, UK;
A previously fit 63-year-old man became unwell on the evening of his second day at 4850 m in the Bolivian Andes. He was drowsy, responded appropriately to questions, and had a mild headache. He had marked periodic breathing and was centrally cyanosed. His pulse rate was regular at 80 beats/min and blood pressure was 135/85 mm Hg. He had mild ataxia demonstrated by a heel-to-toe walking test, but there were no other neurological signs. While sitting, his jugular venous pulse was raised to 2 cm above the sternal angle. Chest auscultation revealed fine bilateral basal crepitations but no peripheral edema. Pulse oximetry showed an arterial oxygen saturation of 62% (Ohmeda 3740, Datex Instrumentarium, Helsinki, Finland). A diagnosis was made of high-altitude cerebral edema with incipient high-altitude pulmonary edema. Because it was evening and descent was considered dangerous, we decided to give oxygen.
The patient was placed semirecumbent and connected to the Fisher circuit with a close-fitting mask (Mallinkrodt, USA). He was initially allowed to breath air for 10 minutes when baseline assessments were made (Figure 1a). Ambient air entry was then reduced for 15 minutes. This caused a small amount of rebreathing, leading to an increase in end-tidal P
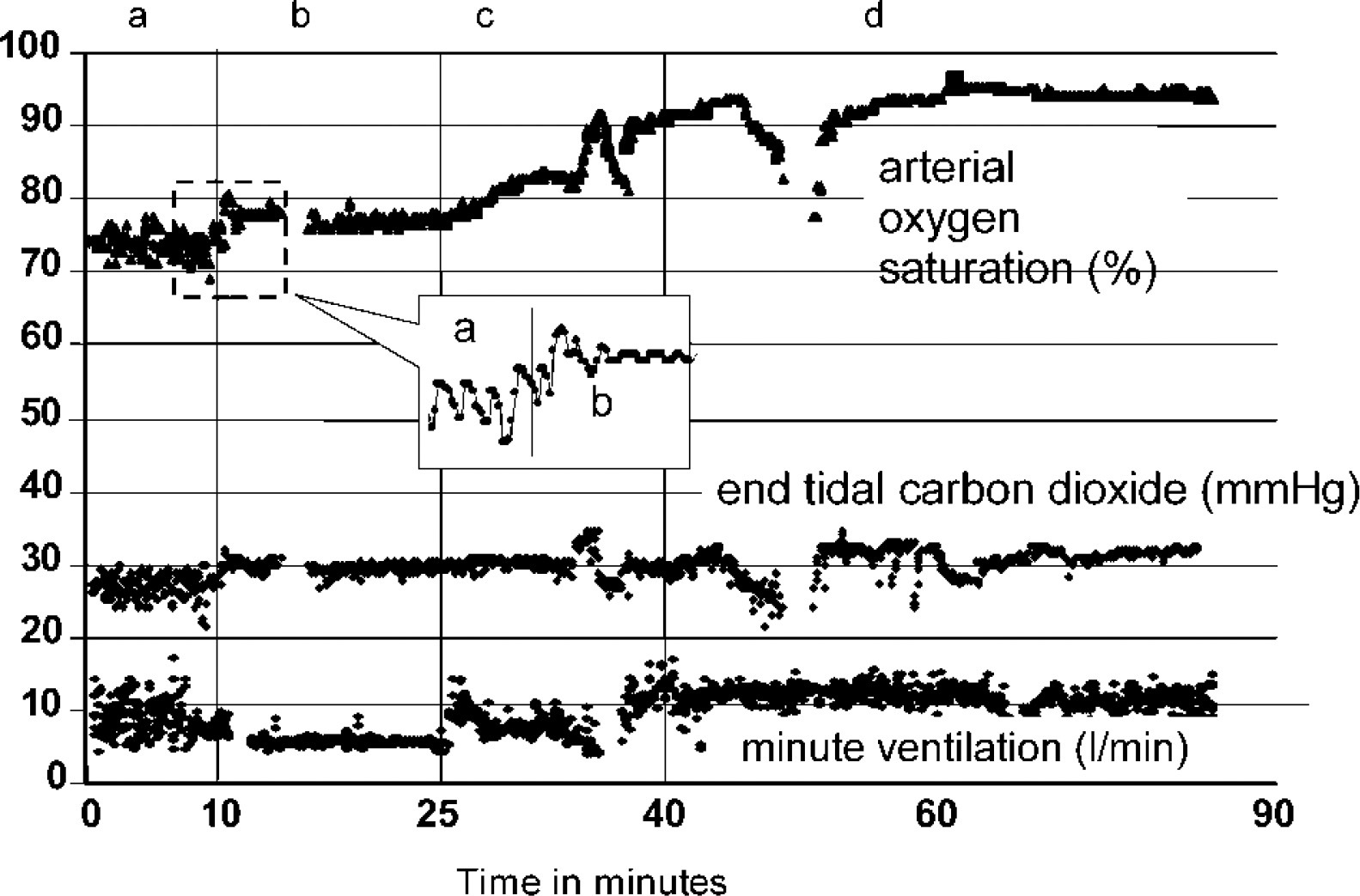
Changes in parameters in the patient with acute mountain sickness while under treatment with the Fisher circuit.
Details of the Fisher circuit are shown in Figure 2. It contains 3 one-way valves in a triangular configuration. The crossover limb valve (C) has an opening pressure slightly greater than that produced by the retraction spring on the bellows (capacity approximately 1000 mL). During inhalation, the bellows collapse first and then gas is drawn from the reservoir bag (capacity approximately 1500 mL). During exhalation, the bellows expand with a mixture of ambient air and oxygen delivered from a cylinder. Gas flow into the bellows is controlled by varying the resistance of the ambient air tube and the flow of oxygen so that the total amount entering is slightly less than needed. Exhaled gas passes into the reservoir bag before venting. Inhaled-gas requirements above those needed for normal ventilation are supplied from the bellows. Gas therefore enters the lungs sequentially: the fresh gas from the bellows enters first, followed by the gas from the reservoir bag, which contains some exhaled carbon dioxide. The mechanics of this circuit allow efficient delivery of oxygen, thereby conserving oxygen supplies.
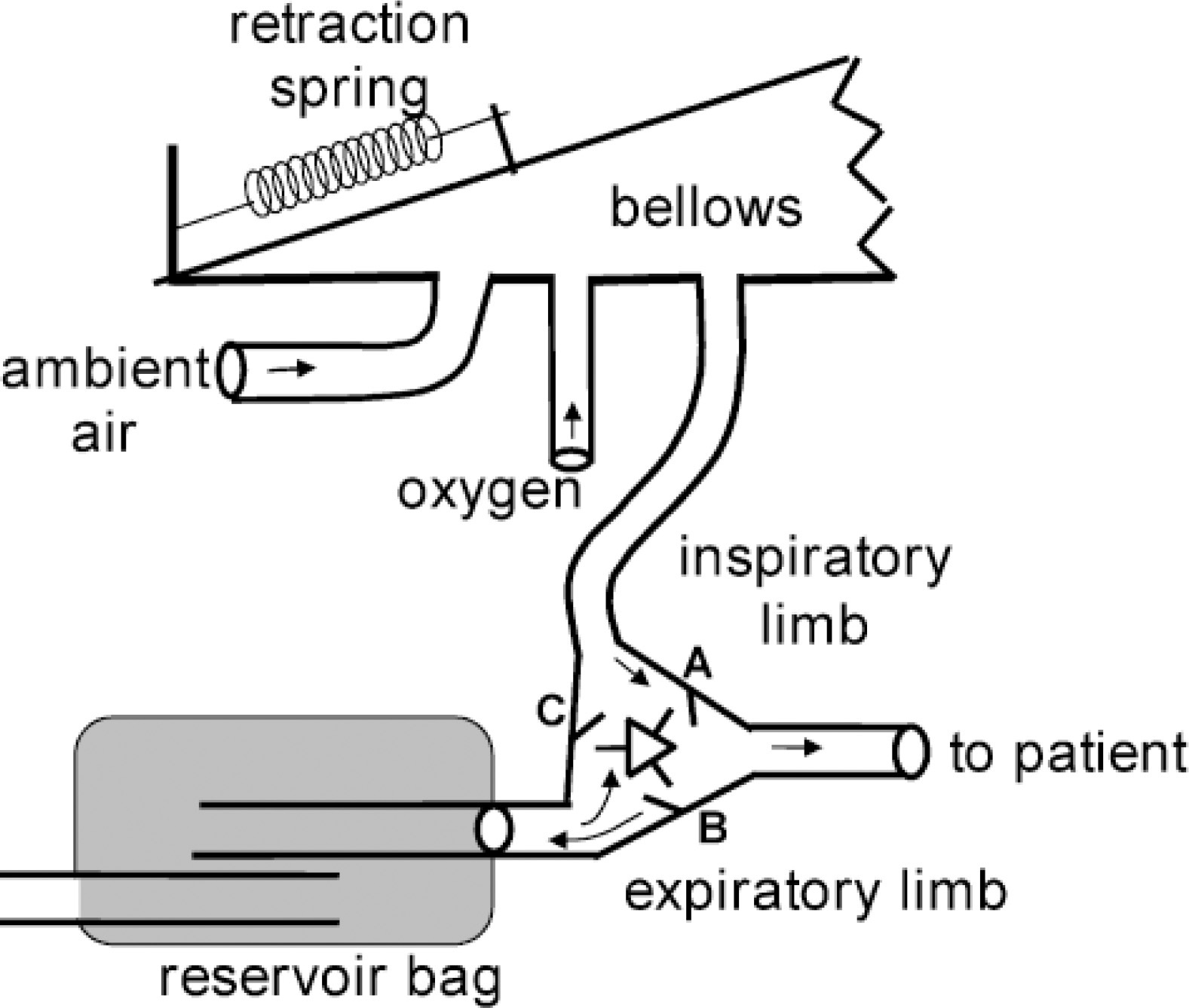
The Fisher high-altitude breathing circuit (components not to scale).
The Fisher circuit provides oxygen and then previously exhaled gas in sequence during inhalation. We suggest that the increased efficiency of oxygen delivery results from 3 mechanisms related to sequential gas delivery. First, the oxygen is mixed with ambient air at a fixed ratio of approximately 3:1, resulting in 40% oxygen being delivered. Second, previously exhaled gas is inhaled, which has a higher oxygen concentration than in ambient air. Third, because the previously exhaled gas in effect washes out the fresh oxygen from the anatomical dead space, all the oxygen delivered into the circuit is directed to the alveoli. In contrast, when oxygen is delivered throughout inspiration, as with the Poisk and nasal prongs, the oxygen delivered at the end of inspiration is sequestered in the anatomical dead space and exhaled at the beginning of the next breath without engaging in gas exchange.
The total volume of delivered oxygen and entrained air provides for alveolar ventilation and carbon dioxide elimination. When we initially treated the patient, we provided the fresh gas from atmospheric air alone. We raised the patient's P
We have shown the Fisher circuit to be useful in an emergency situation as means of providing effective oxygen supplementation with flows of only 1.2 L·min−1. Although control treatment was not possible because of ethical considerations, we would not expect such marked improvement in oxygen saturations with standard circuits.
Footnotes
Acknowledgments
The use of the breathing circuit for treating the subject with high-altitude pulmonary edema and high-altitude cerebral edema was conducted according to the United Kingdom General Medical Council's ethical guidance on experimental treatments. The expedition was supported by a grant from the Mount Everest Foundation.
Funding
This work was supported with a grant from the Mount Everest Foundation and was presented in February 2003 at the International Hypoxia Symposium, Banff, Canada.
1
J.A.F. and R.B.S. are copatentees of the circuit. They are not receiving any payments for the invention. Other authors have no conflicts of interest.