
Abstract
Although eyes are not frequently injured in the mountains, they are exposed to many adverse factors from the environment. This article, intended for first responders, paramedics, physicians, and mountaineers, is the consensus opinion of the International Commission for Mountain Emergency Medicine (ICAR-MEDCOM). Its aim is to give practical advice on the management of eye problems in mountainous and remote areas. Snow blindness and minor injuries, such as conjunctival and corneal foreign bodies, could immobilize a person and put him or her at risk of other injuries. Blunt or penetrating trauma can result in the loss of sight in the eye; this may be preventable if the injury is managed properly. In almost all cases of severe eye trauma, protecting the eye and arranging an immediate evacuation are necessary. The most common eye problems, however, are due to ultraviolet light and high altitude. People wearing contact lenses and with previous history of eye diseases are more vulnerable. Any sight-threatening eye problem or unexplained visual loss at high altitude necessitates descent. Wearing appropriate eye protection, such as sunglasses with sidepieces and goggles with polarized or photochromic lenses, could prevent most of the common eye problems in mountaineering.
Keywords
Introduction
In the mountain or wilderness environment, even minor injuries or visual disturbance could immobilize a person or make him dependent on other members of his party. This could precipitate other problems, such as a slow descent and unplanned bivouacs, thus putting the whole party at risk. This article focuses on the most common eye problems seen in the mountains. It is aimed at first responders, paramedics, physicians, and mountaineers and gives practical advice on the prevention and safe management of these problems, particularly when timely specialist help is not available. The paper is the consensus opinion of the International Commission for Mountain Emergency Medicine (ICAR-MEDCOM).
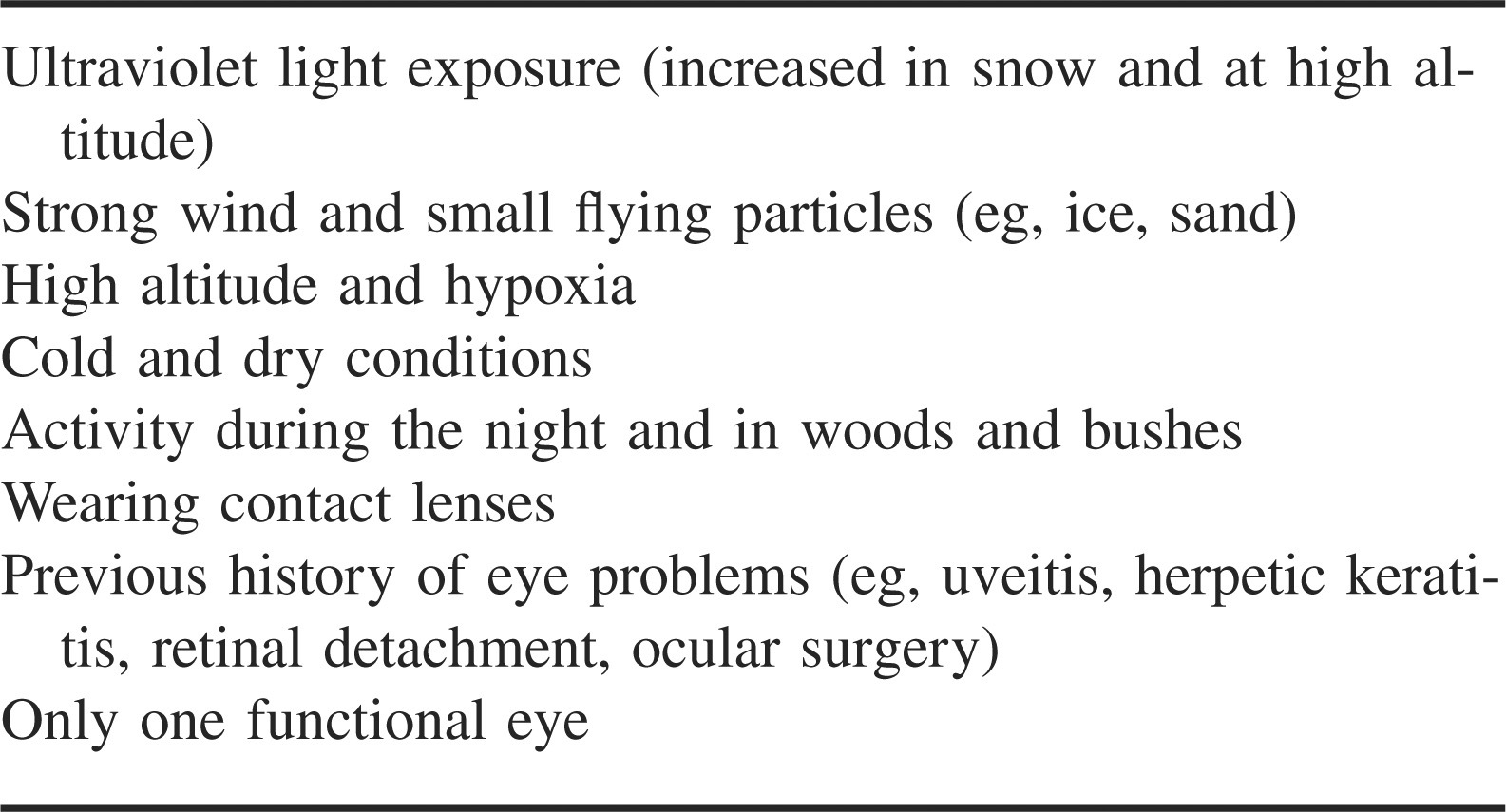
Although the eye surface area is less than 0.1% of the total body surface and therefore infrequently injured, eye injuries related to outdoor and sport activities in the mountains and wilderness areas do occur and induce marked anxiety, particularly in the nonspecialist. Fortunately, most are minor eye injuries. 1 However, unrecognized or poorly treated injuries can lead to permanent and severe visual impairment. In addition, many noxious factors in the environment are magnified in the mountains and expose mountaineers and local inhabitants to an increased risk of eye problems. These factors are listed in Table 1. Wearing contact lenses or undergoing corneal refractive surgery is appealing to a person venturing into the wilderness but requires careful planning if the benefit gained is not to be lost.
Risk factors for eye problems in the wilderness setting
Specific Eye Conditions in Mountain and Remote Areas
Butler has written an excellent chapter on eye problems in the wilderness setting; it serves as a review of the subject. 2 A wider range of eye conditions is presented, as well as photographs and a practical diagnostic approach.
Ultraviolet Light Problems
Ultraviolet (UV) light is a nonionizing solar radiation with a shorter wavelength than visible light. The shorter its wavelength, the more damaging it is to tissues. 3 Fortunately, the earth's atmosphere absorbs all of the shortest wavelengths (UV-C; 180–280 nm) and almost all of the midrange wavelengths (UV-B; 280–314 nm), thus leaving the less damaging longer UV wavelengths at the earth's surface (UV-A; 315–400 nm). The quantity of UV light increases with increasing altitude (at a rate of 4% for each 300-m ascent), low latitude, and in highly reflective environments. For example, the reflection of UV light increases 2 times from the surface of water and 8 times from snow when compared with the reflection from a field of grass. 4 The combination of altitude and snow at 2000 m results in a doubling of the quantity of UV light compared with sea level. Damage to almost all eye tissues (lids, cornea, conjunctiva, and lens) could occur, with the observed pathology being determined by the intensity, wavelength, and chronicity of exposure and the UV absorbance of the tissue. 5
Acute exposure to UV light damages the conjunctiva and cornea, causing snow blindness. Symptoms range from mild irritation and a foreign body sensation to severe pain, light sensitivity (photophobia), lid spasm, and watering. The discomfort starts 4 to 10 hours after exposure and abates 12 to 48 hours later, although sometimes in severe cases it can last several days. The eye is vulnerable to opportunistic infection. 6
Long-term exposure to UV light is associated with conjunctival degenerations (pinguecula and pterygia). 7 The incidence of cataract is higher in populations that have a higher cumulative exposure to UV light. 5 Recent data have suggested that short-wavelength visible (blue) light has a damaging effect on the region of greatest visual acuity (macula) and is a risk factor for macular degeneration.8,9 However, other studies have not confirmed the association, leaving the optimum protective glasses open to debate.10,11
High-Altitude Eye Problems
Disturbance in visual function can result from the hypoxia of altitude and the effects of cold. Hypoxia can cause corneal swelling (edema). 12 In normal eyes, this usually causes no visual disturbance, although after corneal refractive surgery, refractive changes can occur (see below). The increased evaporation of tears at high altitude, especially in windy conditions and when supplementary oxygen is used, can cause dry eyes. This is exacerbated by contact lens wear and makes the eyes gritty and uncomfortable. Lid spasm, light sensitivity, and watering can also occur.
High altitude and hypoxia also affect the retina. Retinal hemorrhage is common but usually asymptomatic. However, if the macula is involved, severe visual difficulties can occur. 13 The cause of retinal hemorrhage and its relationship to other attitude illnesses, particularly acute mountain sickness, is unclear. A single case report of bilateral retinal detachment in a trekker with multiple pre-existing risk factors has been described. 14
In addition, transient monocular blindness (amaurosis fugax) and binocular brain cortex (cortical) blindness have been described. Both seem to resolve spontaneously and are thought to be the result of vascular spasm (ischemia) of the central retinal artery and cerebral blood vessels supplying the visual cortex, respectively. 15
Although rare, freezing of the eyelids and corneas may occur at high altitude or during a blizzard. The condition hampers navigation and is painful but rarely causes permanent damage. More commonly, fogging of glasses can be a real problem, especially when supplementary oxygen is used.
Contact Lens Problems
Contact lenses may successfully be used in the mountains and at high altitude. 16 However, the wearer must be cautious and pay particular attention to cleaning the lenses and avoiding eye infections. Maintaining fastidious hygiene is challenging. Contact lens wearers often note that their eyes become dry and irritated because of the factors mentioned above. This discomfort may be solved with more frequent use of lubricating (rewetting) drops, although this may not always be practical. Even those contact lenses with a high oxygen permeability decrease the oxygen delivery to the cornea. Extended-wear contact lenses are associated with an increased risk of corneal infection and do not allow the cornea any time to recover from contact lens–induced hypoxia. When this is combined with the hypoxia of high altitude, there is a higher risk of visual problems from corneal edema and infection. Therefore, the overnight use of extended-wear contact lenses should be discouraged; daily disposable contact lenses require the least care and are less likely to cause problems. It is imperative that contact lenses be removed at the first sign of discomfort, because continued use risks severe corneal infections and permanent visual loss. UV light–absorbing contact lenses protect the cornea and deeper eye structures. However, the conjunctiva and eyelids are not protected. Contact lenses in a case filled with liquid solution, as well as cleaning solutions and lubricating drops, can freeze in cold weather.
Eye Problems Associated with History of Eye Disease or Surgery
Mader and Tabin have extensively reviewed the literature on mountaineers with pre-existing eye problems venturing to altitude, and the reader is referred to their paper for greater detail. 16 However, it should be stressed that if someone takes regular eye drops for a condition, such as glaucoma, she should remember to take a plentiful supply while away and check with her ophthalmologist regarding storage of medication.
Persons who have had corneal refractive surgery and then go to altitude or into a cold, dry environment, such as the polar regions, may develop blurred vision as a consequence of a refractive change. The problem can occur with most of the common surgical techniques but seems more prevalent when a patient has had a radial keratotomy, an older technique in which radial cuts are made in the cornea. The hypoxia-induced corneal edema makes the person become relatively far sighted; this is of nuisance value at moderate altitude, making map reading difficult, but at extreme altitude can lead to near blindness with severe consequences. Unfortunately the degree of refractive change cannot be predicted. 17 Patients who have had a radial keratotomy could take one pair of “off-the-peg” +3.00D reading glasses to use if required. After bilateral laser in-situ keratomileusis, an opposite (myopic) temporary refractive shift has been reported in 2 climbers going to altitude (6959 m) and a patient who trekked to the North Pole.18,19 These patients were in the “postoperative” period (<4 months since surgery), and it is unclear whether the refractive changes would occur after the surgery was fully matured (>6 months). The change was thought to be due to hypoxia in the case of altitude and a drying of the cornea at the North Pole. Vitreo-retinal surgery after a retinal detachment, for example, frequently involves leaving gas in the globe. This is an absolute contraindication to ascending to altitude as expansion of the gas bubble can threaten irreversible loss of vision. However, this is usually only relevant in the postoperative period.
Eye injuries
Minor injuries of the eye, such as corneal erosions and small corneal surface or conjunctival foreign bodies, can be caused by particles blown into the eye by a strong wind, during hammering, or during ice axe placement. Contact lens use can also lead to corneal erosion. Most small corneal erosions will heal after 24 to 36 hours, as will those left after the extraction of a small foreign body. However, corneal erosions can, rarely, become infected and create an ulcer, so proper recognition and treatment are necessary.
Blunt or penetrating eye trauma with globe rupture may not always be obvious, especially with a small, high-velocity foreign body, but does threaten loss of vision and even the eye itself.
Symptoms and Examination
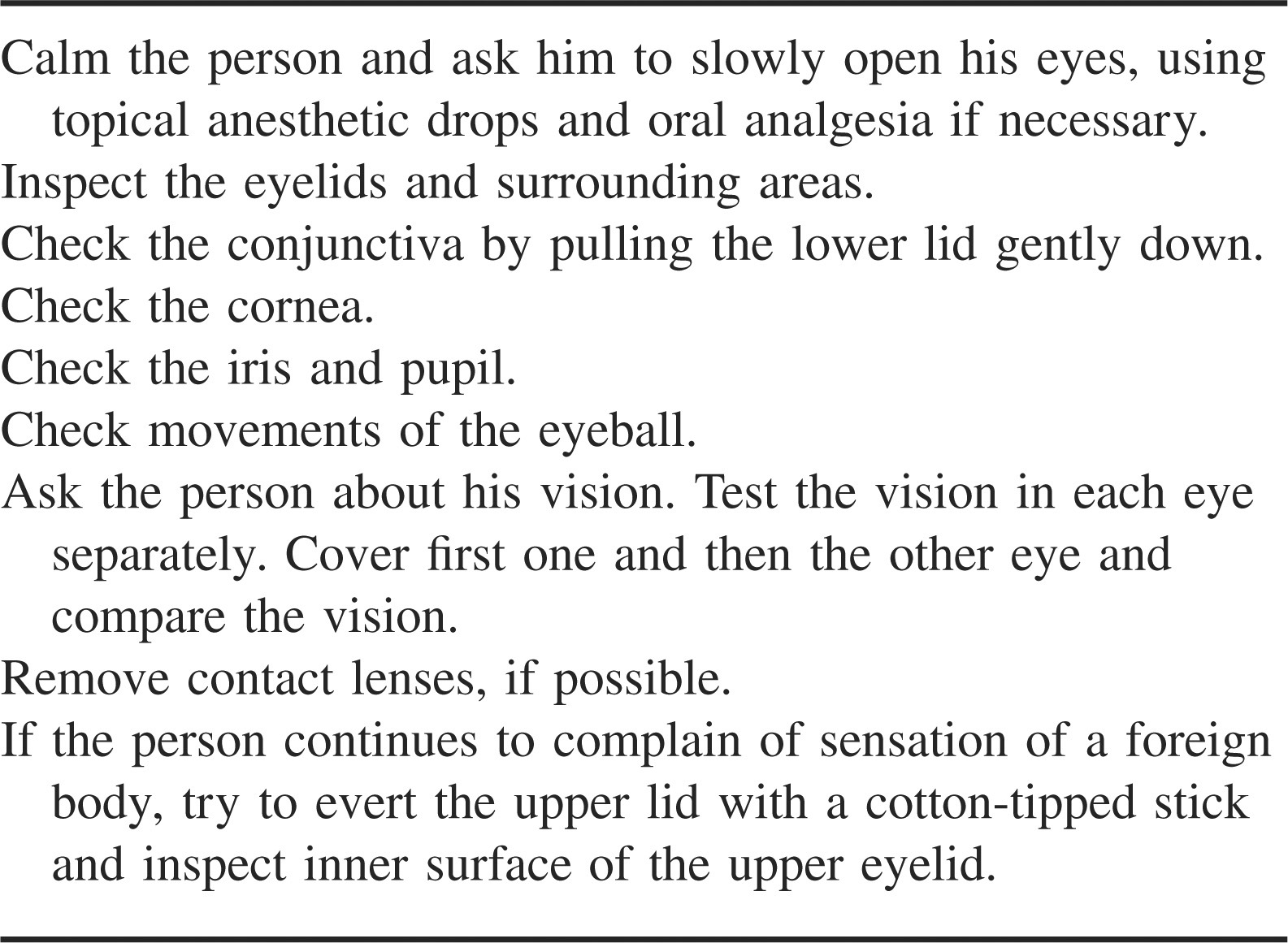
A complaint of blurred vision, eye irritation, or injury should result in a careful inspection. Both eyes are inspected and compared. A penlight and fluorescein drops, which show defects in the corneal surface, will be helpful for the examination. Recent exposure to potential trauma, such as drilling and hammering rock, should be sought. A practical procedure for eye examination is shown in Table 2.
Procedure for a practical eye examination in the wilderness setting
Pain, “red eye” (in which the cornea changes from white to pink/red), light sensitivity, and lid spasm are the most common symptoms of eye trauma and/or infection. An erosion or corneal/conjunctival foreign body is suspected if a person complains of discomfort or pain in the eye after exposure to a strong wind. The sensation of “something in the eye” does not necessarily mean that a conjunctival or corneal foreign body is present. Definitive diagnosis requires the visualization of the foreign body, but sometimes this can be difficult. A common position for a foreign body to be missed is under the upper lid; laypersons going to remote areas should learn the technique for everting the lid. Eyelid trauma should be examined carefully to exclude the presence of a penetrating injury of the eye globe or orbit.
An eye suffering from severe blunt or penetrating trauma usually has pain and poor vision compared with the uninjured eye. If a penetrating injury is suspected, the eye should be examined carefully without manipulation. If the eye is obviously ruptured, the examination should be discontinued.
Presence of blood behind the cornea that obscures the pupil (hyphema) or a large conjunctival hemorrhage with conjunctival edema indicates severe blunt trauma. A very soft eye (hypotony) is likely to be ruptured. Signs of an occult rupture include a large subconjunctival hemorrhage with conjunctival oedema, dark uveal tissue at the corneal margin (limbus), and an irregularly shaped pupil. In the absence of trauma, blood under the “white of the eye” without pain and without changes to the cornea or iris in an eye with normal vision is not a serious sign.
Treatment
General considerations
Symptomatic eyes are usually most comfortable if the eyelids are gently closed. The addition of sunglasses or goggles can also help. In most cases, applying a soft dressing as a pad or patch is to be discouraged, because the pad creates a natural culture medium and can cause abrasions if not applied with sufficient pressure to hold the eyelids shut. Patching does not improve healing nor reduce pain, and it prevents binocular vision. 20 An exception may be a large (>3.3 × 3.3 mm) corneal abrasion, in which a properly applied pad, splinting the eyelid, could be considered if symptoms are severe. In such cases, the patch should be applied for as short a time as possible and topical antibiotics instilled. Topical eye anesthetics delay corneal healing, but a single application for purpose of diagnosis and examination is useful. Repetitive applications should only be used in extreme situations to control disabling symptoms. In such cases, systemic painkillers (analgesics) tend to help. An urgent evacuation is necessary when the eye has been penetrated or ruptured, when blunt trauma has decreased the vision, or when a severe lid laceration is present.
Snow blindness
The person should be reassured and asked to close both eyes and rest in a dark place until the discomfort regresses. Nonsteroid anti-inflammatory eye drops, such as diclofenac 0.1% and antibiotic ointment, can be used to soothe the eye and prevent infection. Analgesics, such as paracetamol (acetaminophen), may also be necessary. Cooling through the closed eyelids may reduce discomfort, and, of course, it is obligatory to wear sunglasses afterwards to prevent a recurrence.
Corneal erosions, with or without small foreign bodies
A foreign body should be washed out with clean water and movements of the eyeball. If unsuccessful, the foreign body could be removed by gently lifting it off the eye with a cotton-tipped swab or piece of gauze. Topical anesthetic drops make this procedure more comfortable and the patient more cooperative. The routine use of antibiotic drops or ointment, such as bacitracin, tobramycin, and ciprofloxacin, after the removal of a foreign body is not required in the clinic setting. 21 However, in the wilderness environment where hygiene is less optimal and the management of a severe infection more challenging, using a prophylactic topical antibiotic is still recommended by some experienced eye specialists. Certainly, erosions secondary to contact lenses should have a topical wide-spectrum antibiotic applied. 22 If infection has gained a foothold, perhaps because of delayed treatment, a topical antibiotic applied hourly for 24 to 48 hours is indicated. In these cases a patch should never be applied. Erosions at very high altitude are treated likewise. Systemic analgesics and/or nonsteroid anti-inflammatory eye drops can be used if the discomfort persists.23,24 The latter, though expensive, may reduce the need for sedative oral analgesia and thus allow the person to remain mobile. 25 Sunglasses should be worn afterwards. If eye discomfort persists after 24 hours, suspect infection or a missed foreign body.
Suspected or obvious penetration of the eye and severe blunt trauma or globe rupture
A penetrating injury should be suspected whenever ocular trauma occurs. If after careful examination a penetrating injury is still suspected, treat the eye as if the injury is present. Do not use any topical preparations or remove a foreign body that has ruptured the eye unless very extenuating circumstances dictate otherwise. Close the eye carefully; place a soft dressing over it without applying pressure and use a protective shield or goggles to prevent any inadvertent pressure during the evacuation. Paracetamol (acetaminophen) tablets may not be strong enough to relieve the pain, so stronger analgesics can be given if appropriate. Systemic antibiotics, such as ciprofloxacin by mouth, should be started as soon as possible and an immediate evacuation arranged, using a helicopter if available. Ideally, an eye specialist in hospital should treat a lid laceration that penetrates the full thickness of the lid or involves the lid margin. Other lid lacerations can be managed as uncomplicated surface wounds, but it is important to check that the eyelids can completely close so as to avoid corneal drying.
High-altitude eye problems
Reduced vision at high altitude can present a serious risk to the patient and have consequences to the rest of the party. Descent is recommended. In the presence of high-altitude illness, follow the International Mountaineering and Climbing Federation (UIAA) guidelines. 26 Descent is not required if asymptomatic retinal hemorrhages are discovered in an otherwise well individual. However, other risk factors, such as pre-existing monocular vision or the presence of other high-altitude illness, may prompt descent.
If a contact lens wearer develops any eye symptom, the lens should be removed and lubricating drops applied. Antibiotic eye drops or ointment should be applied immediately if symptoms continue. If, despite antibiotics, the eye does not rapidly improve over 48 hours, descent and a different topical antibiotic should be considered.
Prevention of eye problems
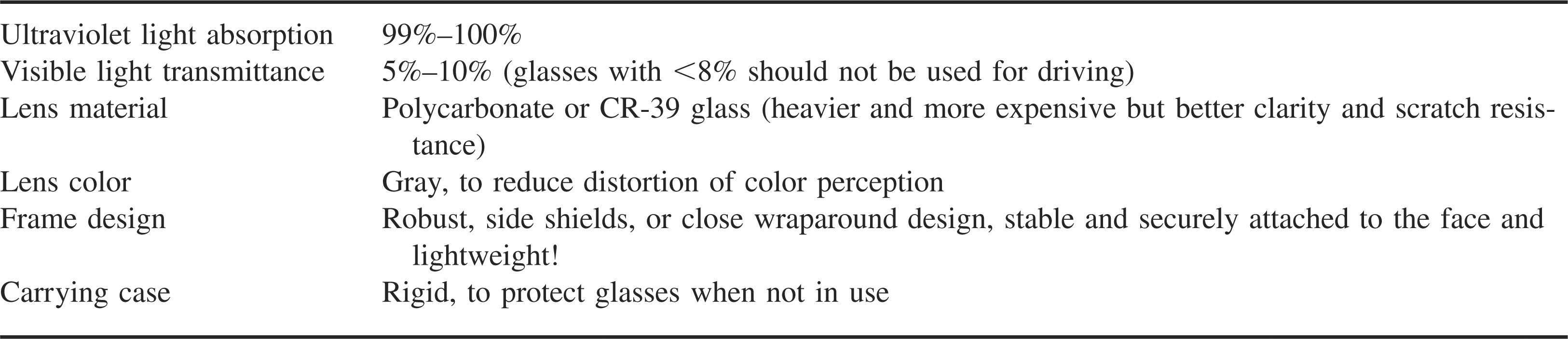
Protective glasses of polycarbonate with side shields or adequate eye protection in the form of goggles should be worn whenever there is a risk of eye trauma. It is obligatory for all persons in snowy and mountainous conditions to wear high-quality sunglasses that absorb all UV light. 27 Table 3, adapted from the suggestions of Butler, describes their desirable attributes. 2 Hats with a shield also reduce UV light exposure and increase comfort levels. Children's eyes are particularly sensitive to UV light. Ski goggles are often more practical and comfortable at high altitude or in windy conditions. Fogging can be problematic, particularly when supplementary oxygen is used; ventilated goggles can effectively reduce this. Working near helicopters, where the turbulent air is often filled with foreign bodies, is a risky environment. Goggles are particularly recommended for rescue personnel.
Desirable characteristics of sunglasses for use in the mountains 2
Contact lens wearers should carefully plan their mountaineering and be prepared to deal with the problems described above. They must be cautious and pay particular attention to cleaning lenses and avoiding eye infections. To avoid dry or irritated eyes, lubricating drops should be used frequently, although this may not always be practical. The use of extended-wear contact lenses should be avoided, especially at high altitude. Contact lenses in a case filled with liquid solution, such as cleaning solutions and lubricating drops, should be kept warm inside a sleeping bag. Nonprescription protective sunglasses or ski goggles will be required, as well as backup refractive glasses and sunglasses, whenever the person is in a mountain or wilderness area. Antibiotic eye drops or ointment should also be carried.
People going to very high altitude (>3500 m, or 11 483 ft) or into remote areas who have a previous history of eye disease, such as uveitis and herpetic keratitis, should consult their eye specialist and take appropriate prescribed medication with them in case they suffer a recurrence of the disease. Having the correct medications and knowledge to use them can avoid many problems. Persons with previous retinal detachment surgery should consult their eye surgeon as to when they can return to altitude. In addition, Morris et al 14 advise that all high myopes (people who need thick lenses equivalent to −6.00 dioptres to see distant objects) going to very high altitude undergo a full prophylactic retinal examination for risk factors of detachment. Though they describe a single case of retinal detachment in such a setting, more studies are required to quantify the risk before accepting this recommendation.
Footnotes
Acknowledgments
The authors thank Dan Morris for his suggestions during the preparation of the manuscript.
The recommendations presented in this paper have been discussed and were officially approved at the annual International Commission for Mountain Emergency Medicine (ICAR MEDCOM) meeting in Pontresina, Switzerland (2007), by the following members of the International Commission for Mountain Emergency Medicine: Giancelso Agazzi (I), Borislav Aleraj (HR), Jan Beaufort (CZ), Jeff Boyd (CA), Hermann Brugger (President) (I), Florian Demetz (I), Tigran Elezovic (BIH), John Ellerton (GB), Fidel Elsensohn (Vice President) (A), Gianluca Marconi (I), Martin Ivanov (BG), Pavel Jonek (PL), Peter Mair (A), Mario Milani (I), Werner Mährlein (D), Maria-Antonia Nerin (E), Marie Nordgren (Sweden), Peter Paal (I), Gula Przemyslaw (PL), Oliver Reisten (CH), Peter Rheinberger (FL), Erik Sandstrom (Sweden), Theoharis Sinifakoulis (GR), Sven Skaiaa (N), Inigo Soteras (E), Michael Swangard (CA), Günther Sumann (A), Dario Svajda (HR), Steve Teale (SCO), Oleg Tcholakov (BG), Iztok Tomazin (SLO), Vlahov Vitan (BG), Nicole Vogt (FL), David Watson (CA), Gregoire Zen-Ruffinen (CH), Eveline Winterberger (CH), Ken Zafren (USA). This article reflects the consensus of opinion of ICAR-MEDCOM, which is fully responsible for the content. The authors have no conflict of interest, nor have they received any financial or material support from pharmaceutical companies whose products were mentioned in this paper.