
Abstract
A 24-year-old male snowboarder was buried in an avalanche for 20 h and rescued on the next day at a depth of 2.3 m below the snow surface. A large air pocket was noted in front of his mouth and nose. He was responsive but moved restlessly and uncoordinatedly. The epitympanic temperature was 22.5 °C. He was bradycardic (35/min), and a right bundle branch block with Osborn waves was noted. Rewarming (1 °C/h) was initiated with continuous hemodialysis; core temperature raised to 29.8 °C within 4 h. At 30 °C he became conscious. With rewarming, the heart rate increased to 90 beats per minute and the ECG changes disappeared; nonfreezing cold injuries were noted. On the next day, his pulmonary function deteriorated—fluid overload of 9 L since admission was diagnosed. With spontaneous diuresis, the situation improved. On Day 4, the neurologist reported subtle polyneuropathy in both legs secondary to hypothermia, without tendency to regress. This case occurred more than 20 years ago but has not been reported yet. To this day, this is the third-longest critical avalanche burial ever reported. We discuss the circumstances of this accident, the clinical course, and how treatment has changed since 2000.
Case Report
On a cold winter day in January 2000, a 24-year-old male was snowboarding in a ski resort in the Western Austrian Alps with 2 friends. Heavy snowfall had been reported for the past 3 d and continued until the following day. The temperature was −10° C at 2000 m above sea level. The avalanche warning level was 4 (high) on the 5-point scale. At 14:45, the 24-year-old and one of his friends decided to descend from the summit station of the skiing area in deep powder snow off-piste; the third friend stayed on the groomed ski slope. At 17:55, the 2 friends who had planned to descend off-piste had still not reached their friend at the valley station; he reported them missing at the emergency dispatch center. Later, it was ascertained that the 2 snowboarders had been buried completely in deep powder snow by a spontaneous slab avalanche. Night had already fallen when the search and rescue mission started. During the night, 80 cm of snow fell, and the visibility was poor. The avalanche warning level was still 4. The search and rescue operation was difficult and was stopped at 23:30 because the risk to the rescue team was considered too high. On the following day, at 07:30, the search and rescue mission resumed. Three hours later, the 2 missing snowboarders were found. The first one was located at 10:50 by an avalanche dog and pronounced dead immediately after extrication. His airway was completely blocked by the snow. The postmortem examination indicated asphyxiation as the cause of death, which had likely occurred 15 to 30 min after burial. The same avalanche dog located the second victim at 11:00. He had been buried for 20 h at a depth of 2.3 m below the snow surface in a lateral position, with both legs bent. The victim wore large ski goggles that had slipped over his mouth and nose during the fall and formed a small air pocket. An air connection was noted with a large air pocket around a rock close to the ground (Figures 1 and 2).
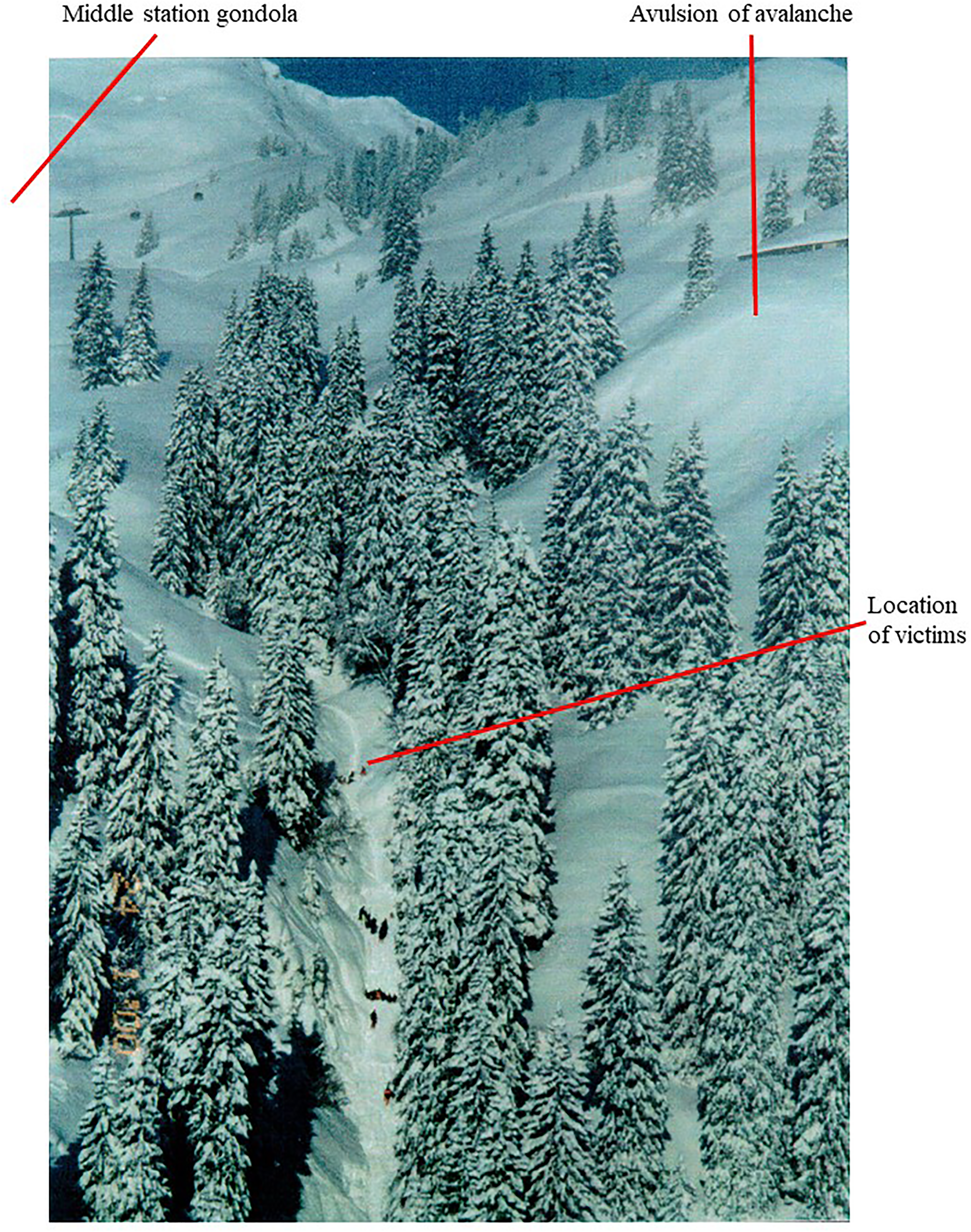
This image shows the avulsion of the avalanche, the middle station, where the avalanche victims started their descent and the location of the victim.
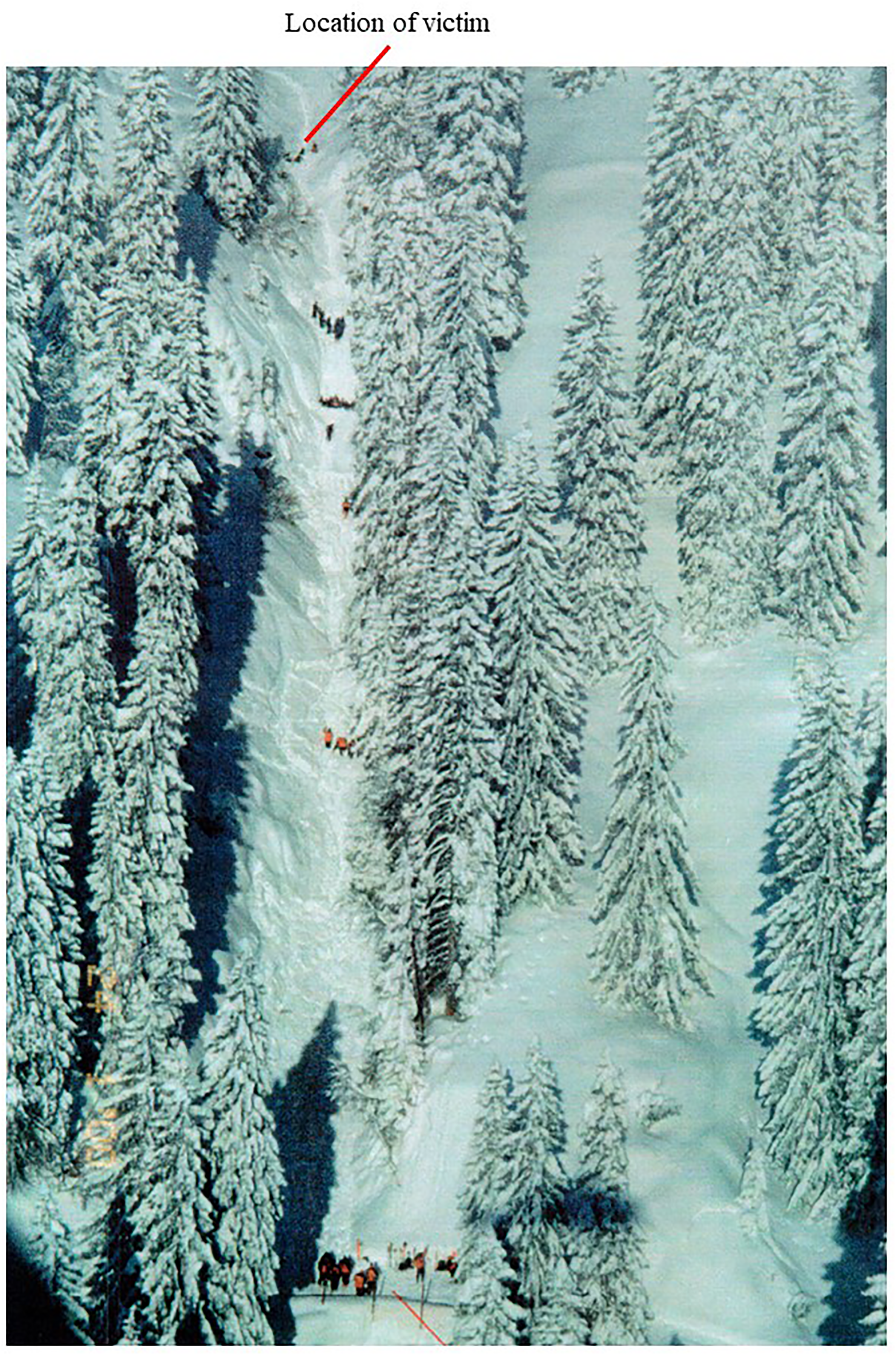
This historic image shows the location where the victim was located and the position of the rescuers.
At extrication, the victim was responsive but moved restlessly and uncoordinatedly. He did not show any obvious sensory or motor deficits. The epitympanic temperature was 22.5 °C. The patient was warmed with chemical heat packs on the trunk and firmly placed into a rescue bag. Thereafter, he was evacuated by helicopter hoist directly from the burial site and flown to the next tertiary-care-level hospital. During extrication, transport, and in-hospital rewarming, moving the patient was kept to a minimum.
Upon arrival at the hospital at 12:00, the patient was still responsive and restless but was not responding adequately. The temperature, measured with an indwelling urinary catheter, was 24.1 °C. The electrocardiogram (ECG) showed sinus bradycardia, an Osborn wave, and multiple broad-complex extrasystoles. The initial systolic blood pressure was low, between 80 to 95 mm Hg, which—in combination with the negative base excess (BE) and the fact that the patient had not had any fluid intake for more than 24 h—was interpreted as a sign of exsiccosis and treated with 9 L of crystalloid fluid. Any movement of the patient resulted in cardiac arrhythmias—mainly broad-complex extrasystoles and a few narrow-complex extrasystoles in the otherwise bradycardic sinus rhythm. The patient did not present any injuries.
The patient was admitted to the intensive care unit (ICU). An arterial line was inserted into the right radial artery, and a central venous catheter was inserted into the right jugular vein. The first arterial blood gas analysis on ambient air showed paO2 146 mm Hg, paCO2 56 mm Hg, pH 7.22, and base excess −3.8. No information on potassium or lactate levels was available. Upon admission to the ICU, the ECG showed a profound bradycardic sinus rhythm (35/min) with a right bundle branch block and paroxysmal broad-complex and narrow-complex extrasystoles, as well as Osborn waves. The CVP during the state of hypothermia was reported to be 16 mm Hg, although it is not clearly differentiated whether this reading was seen before or during the fluid administration. Rewarming was initiated with continuous hemodialysis with a rewarming speed of 1 °C/h. Core body temperature was raised to 29.8 °C within 4 h. Continuous hemodialysis was stopped, and the patient rewarmed spontaneously. With rewarming, the heart rate had increased to 90 beats/min, and the ECG changes had disappeared, now showing a normofrequent sinus rhythm without any sign of ectopy and no Osborn waves. On controls, the ECG, which was already normalizing during rewarming, was unremarkable, and the systemic blood pressure, as well as the CVP, regained physiological values.
With continuous rewarming and a core temperature above 30 °C, the patient's awareness improved gradually. He started to open his eyes when addressed, responded to simple questions, and started to move all 4 extremities consciously. Bolus sedation with Midazolam and Morphine was carried out for less than 24 h to treat agitation and was stopped as agitation improved the day after admission to the ICU.
Upon ICU admission, both legs showed nonfreezing cold injuries. The right leg recovered quickly, the left slower. Until 5 h after the ICU admission, edema of soles and toes on both sides increased; they remained cyanotic. The right hand, where the arterial line was inserted, showed discoloration. Therefore, the arterial line was removed and inserted into the femoral artery. Thereafter, the perfusion of the right hand improved rapidly.
On the day after ICU admission, the patient was fully orientated to person, place, and time. He reported on his experience of being buried. He felt tired, and his thought process seemed slowed down. From Day 2 after admission, the patient developed almost 39 °C fever, which was treated pharmacologically and with physical cooling.
The patient survived the avalanche accident and the subsequent ICU stay without tracheal intubation and mechanical ventilation. However, on the day after the rescue, the patient's pulmonary function deteriorated. In the blood gas analysis on ambient air, PaO2 dropped to 61 mm Hg and PaCO2 was 23 mm Hg, with persistent hyperventilation. Noninvasive continuous positive airway pressure (CPAP) and high-flow oxygen were used to treat the hypoxia. The chest x-ray showed incipient infiltrations in the left middle lobe suggestive of pulmonary infection and the image of a bilateral interstitial pulmonary edema. The thoracic computed tomography (CT)-scan showed bilateral overhydration and extensive, small, confluent alveolar infiltrations on the left. The overhydration was secondary to fluid management of 9 L within the first 18 h after admission because of supposed initial exsiccosis. The parenteral fluid administration was stopped 18 h after the admission, and the patient spontaneously increased diuresis. Oxygenation improved rapidly and persistently, and the radiological signs had disappeared by Day 3.
On Day 4, before discharge from the ICU, the attending neurologist examined the patient and confirmed a full cerebral recovery. The clinical presentation of the nonfreezing cold injuries had improved: the discoloration and edema of the feet had diminished, and there were no signs of necrosis. The patient was discharged from ICU after 4 d with only a subtle polyneuropathy remaining in both legs, manifesting in paresthesia without any weakness, secondary to nonfreezing cold injury, without tendency to regress.
Discussion
We present a case of critical avalanche burial with one of the longest burial times ever recorded. Three features of this case are particularly interesting and will be discussed below.
LONG BURIAL TIME
The burial time was exceptionally long. Only 2 persons have survived a longer avalanche burial in an open area, 1 with a burial duration of 43 h 45 min (1972, Italy, female, age unknown), the other with 25 h 30 min (1960, Canada, male, 59-year-old).1–3 Reasons for a good outcome after long avalanche burial in an open area include the presence of a large or open-air pocket, no obvious major injuries, victims well insulated to avoid fast and critical cooling within hours, and no hypothermic or asphyctic cardiac arrest. A retrospective study analyzed the survival probability in avalanche victims with long burial (≥60 min) and identified several correlating parameters 4 : the median burial depth of survivors (70 cm) was significantly more superficial than for those who died (100 cm). 4 Our avalanche victim survived, despite being buried 230 cm below the snow surface, therefore contradicting this study. The same study reported that the estimated survival probability dropped from 23% after 60 min of burial duration to less than 6% after 1400 min, approximately 24 h. 4 The odds ratio of the decrease in survival was 0.93 per hour. 4 The presented case provides evidence that avalanche victims can survive long and deep burials in the presence of a large air pocket. Therefore, search and rescue teams should be encouraged to continue their operation until the avalanche victim is extricated and a proper diagnosis can be made.
PULMONARY EDEMA
On the first day after extrication, the patient developed pulmonary edema. Pulmonary edema after avalanche burial is rare but has been described before.5,6 Pulmonary edema after avalanche burial has been attributed to the negative pressure, which develops when buried victims strenuously breathe against an occluded air space; this phenomenon is known as negative-pressure pulmonary edema. 7 Avalanche burial-related pulmonary edema may also be triggered by hypoxia-induced left ventricular failure and pulmonary arterial hypertension.
In the present case, the thoracic CT scan identified bilateral overhydration and confluent alveolar infiltrations, probably due to severe and prolonged hypothermia with capillary leak and extravasation in combination with lung contusion. Another reason could also have been a delayed and slow-onset negative pressure pulmonary edema. Overhydration is explained by the large amount of fluid administered within the first 18 h of admission. Today, fluid resuscitation should be guided with continuous real-time hemodynamic monitoring, which may include clinical indices of the adequacy of tissue and organ perfusion, echocardiography, as well as hemodynamic parameters. 8 Avalanche burial-related pulmonary edema resolves within 24 h as soon as the triggers are removed and causal therapy with CPAP and negative fluid balance is commenced. Endotracheal intubation and mandatory ventilation are rarely required. After critical burial, the potential injury pattern, the current treatment guidelines, and the risk of pulmonary edema must be considered,9–11 and the target hospital must be selected accordingly.
NONFREEZING COLD INJURY
The patient suffered nonfreezing cold injuries. Nonfreezing cold injury is a modern term for trench foot or immersion foot, a condition that results from a combination of exposure to moisture and constant low but above-freezing temperatures. 12 Nonfreezing cold injury seldom, if ever, results in loss of tissue unless there is also pressure necrosis or infection. 12 In an avalanche, depending on the environmental temperature and with some distance to the surface, snow temperature is only slightly below 0 °C. In this case, the patient was buried more than 2 m below the snow. Discoloration of the skin of both legs, which was at first considered third-degree frostbite, was noted at hospital admission. The patient never developed signs of freezing cold injuries (ie, frostbite, blisters, or necrosis) but suffered from dysesthesia until discharge. With exposure over several hours or days to an environment with a temperature around 0 °C, nonfreezing cold injuries have been described.12,13 Neurological sequelae tend to last months or even years. 12 In our case, the neurological sequelae resolved completely, and the patient resumed his occupation without any restriction.
DIFFERENCES THEN AND NOW
This case happened in 2000. Compared to today, the treatment has changed in several aspects. In this specific case, the following aspects of treatment would be handled differently according to present-day guidelines
10
:
Current guidelines recommend transporting severely hypothermic avalanche victims, who present with a core temperature <30 °C, systolic blood pressure <90 mm Hg, ventricular arrhythmias, or any other cardiac instability, directly to a center offering rewarming with extracorporeal life support (ECLS).10,14 There, in case of hypothermic cardiac arrest, ECLS rewarming could be initiated with minimal delay.10,15 In 2000, this treatment had already been established, but no recommendation existed to transfer patients with core temperature <30 °C directly to a center capable of ECLS rewarming. In an ECLS center, a patient with core temperature <30 °C and spontaneous circulation should be rewarmed actively externally (eg, with warmed forced air) and minimally invasively (with warmed infusions, according to volume requirements).
15
This technique is usually effective.
15
If a patient fails to rewarm adequately, active internal rewarming should be used.
15
Active internal rewarming methods in moderate-to-severe hypothermia include intravascular rewarming catheters, continuous renal replacement therapy (CRRT), and extracorporeal membrane oxygenation (ECMO).
15
Insertion of arterial and venous catheters is managed differently today. In the present case, the cannulation of the radial artery caused hypoperfusion of the ipsilateral hand. The better option is to cannulate the femoral artery in the first place, preferably with ultrasound guidance. Secondly, the insertion of the dialysis catheter into the jugular vein using the Seldinger technique can be risky, as the guidewire may cause arrhythmias and even ventricular fibrillation when advanced into the hypothermic and highly irritable right atrium.
16
It is, therefore, advisable to insert central venous catheters into the femoral vein, preferably on the same site as the arterial catheter, to spare the second side for possible cannulation for ECLS rewarming.
Overall, if the same patient were treated today, some peculiarities in treatment would be handled differently. The outcome, very likely, would be the same.
Conclusions
We report the third-longest known case of critical avalanche burial (20 h), which happened in 2000. The lowest core temperature was 24.1 °C. The patient always maintained spontaneous circulation. He was rewarmed with continuous hemodialysis until 30 °C, followed by spontaneous rewarming. Within 24 h, the patient developed pulmonary edema, which resolved with oxygen administration, CPAP, and spontaneous diuresis. He also suffered nonfreezing cold injuries of his feet; symptoms persisted until hospital discharge. According to present guidelines, a patient in this condition should be transported to an ECLS center and rewarmed actively and minimally invasively. Fluid administration should be individually titrated to avoid overload and pulmonary edema. If a patient fails to rewarm adequately, active internal rewarming should be used. Only in a hypothermic cardiac arrest patient should ECLS rewarming be initiated.
Footnotes
Acknowledgments
We would like to thank Daniel Spiegel, Herbert Strolz, and Hermann Brugger for providing data, detailed information, and support, as well as the mountain rescue, helicopter, and hospital team who took good care of this patient.
Author Contribution(s)
HL provided all necessary data and information on the case. BW and PP conscripted the first draft of the manuscript; all authors critically adapted the following versions and were major contributors in writing the manuscript. All authors read and approved the final manuscript. BW submitted the paper as corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.