
Abstract
Introduction
Lightweight shelters made of water- and windproof polyester are frequently used by mountain rescue, but information on physical and psychological stress during their use is scarce.
Methods
A prospective observational study was conducted with 48 experienced rescuers who performed cardiopulmonary resuscitation training on a manikin in a shelter in alpine terrain. The objective parameters of air temperature, moisture, and concentrations of carbon dioxide and oxygen were measured inside the shelter. The subjective experience of the rescuers regarding stress, moisture, noise, air draft, convenience, spatial confinement, brightness, room temperature, and air quality was assessed using a questionnaire.
Results
During 15 min of cardiopulmonary resuscitation, the median temperature in the shelter rose by >15°C (Δt, 15.9°C; interquartile range, 14.3–16.5°C; P=0.018). Carbon dioxide concentrations increased to 0.97 vol% maximum. Bag valve mask ventilation was established with and without the use of supplemental oxygen, which showed significantly different oxygen shelter concentrations (21.1 vol% with oxygen, 20.6 vol% without oxygen; P<0.001). Most participants rated the physical comfort and spatial conditions inside the shelter as convenient.
Conclusions
In this study, the use of shelters in alpine terrain improved physical comfort while carrying out a rescue. Most participants gave high ratings for the working conditions in the shelter.
Keywords
Introduction
Extreme environmental conditions such as low temperature, wind, and precipitation may hamper emergency treatment of patients in remote settings and high altitude regions and increase the risk of hypothermia. Furthermore, hostile environmental conditions aggravate rescue and complicate treatment.
1
Heat loss in trauma patients is associated with increased mortality.
2
A cold environment causes clotting disorders and accelerates the progress of circulatory shock.
3
Peripheral vasoconstriction also renders venous access difficult. Furthermore, low temperature alters the viscosity of intravenous fluids and the flexibility of venous lines, tubes, and plastic materials.
4
In addition to extreme environmental conditions, other factors contribute to physical stress in rescue personnel and Emergency Medical Services (EMS) personnel during missions.
5
In wilderness and mountain medicine, psychological stress is assumed to be particularly high during cardiopulmonary resuscitation (CPR) at high altitude.5,6 In case of a wilderness emergency, a lightweight 6- to 8-person shelter can be rapidly erected over the patient, providing sufficient space to work and to keep the patient and rescuers out of the elements. Shelters are made of wind- and waterproof polyurethane-coated polyester and provide protection from heavy winds and rain during emergency operations. This may mitigate the effects of adverse weather conditions on the quality of patient treatment
Methods
Study Design, Endpoints, and Locations
We performed a prospective observational study on the use of shelters in mountain rescue under working conditions in alpine terrain. Participants were experienced rescuers from the Austrian Mountain Rescue Service and Austrian Police Special Forces unit who performed their annual training. Inclusion criteria were volunteers >18 and <80 y of age. Exclusion criteria were missing informed consent and premature termination of study participation.
We evaluated the subjective assessment of physical comfort and working conditions in the shelter. In addition, participants were asked for their subjective assessment of whether working conditions in the shelter could have a positive impact on CPR efficiency compared with experience with previous outdoor CPR. Because shelters have only been used routinely in mountain rescue operations in Tyrol for about 8 y, most participants also could provide a comparison with the time before shelters were available. The difference between the environmental conditions outside and the ambient conditions inside the shelter was directly accessible to all participants. Participation in the study was voluntary and occurred between obligatory tasks during a period of official training. Written informed consent was obtained from all participants prior to the investigations. The participation rate (number of participants in the study divided by the total number of participants in the training multiplied by 100) was 22.9%. Both use of a shelter and Basic Life Support were among the familiar tasks in use. The study was conducted in accordance with the principles of the Declaration of Helsinki concerning the conduct, evaluation, and documentation of the data. 7 The institutional ethics committee did not consider ethics approval necessary for this observational study.
The primary endpoint was the participants’ subjective assessments of working conditions in the shelter. The secondary endpoint focused on objective environmental parameters in the shelter, including temperature and oxygen (O2) and carbon dioxide (CO2) concentrations.
The subjective assessments of rescuers who performed CPR on a manikin in an emergency scenario with simulated cardiac arrest were evaluated. Investigations were made at three locations during annual training of local mountain rescue forces and special police forces. Measurements were performed under comparable environmental conditions (air temperature, –10.0 to 3.9°C; relative humidity, 66–70%; sky cover, 1/8–4/8; wind, NE–E, <20 km/h, no precipitation) in 3 locations of the alpine region, namely 1) Schmirn (1407 m above sea level), 2) Jamtal (2165 m above sea level), and 3) Lucknerhaus by Kals (1918 m above sea level), Tyrol, Austria.
Participants and Investigation Materials
A total of 48 participants were enrolled in teams of 4 persons per test run (16 members of the Mountain Rescue Service and 8 members of the special police forces in the cohort using supplemental oxygen, and 24 members of the Mountain Rescue Service in the cohort without supplemental oxygen). Written informed consent for participation and publication was obtained prior to the study. Sequence of participation and assignment to the teams were determined by the arrival of the participants.
The emergency scenario was conducted by all teams following the same protocol. All team members were aware of performing CPR on a manikin in an experimental setting, but they were not informed about the specific sequence and duration of investigations. After a 10-min ascent, the team came across with the patient (Resusci Anne Simulator, LAERDAL Medical AS, Stavanger, Norway) lying in a supine position on a flat snow surface. While 1 rescuer checked the vital functions of the patient, the 3 other rescuers started concurrently to erect the shelter (6- to 8-person Rab group shelter; Rab Mountain Equipment, Somercotes, Derbyshire, UK) over the casualty. This brand is commonly used by Mountain Rescue and Helicopter Emergency Medical Services in Tyrol, Austria (Figure 1a). In the emergency scenario, the shelter was pulled over the rescuers with the patient in the center. Two ski poles were used to put it up. The shelter was not fixed directly to the ground but was pressed to the ground by the feet of the rescuers inside the shelter. With 5 people (4 rescuers and 1 observer in addition to the manikin) in the shelter, change of position between the rescuers during the resuscitation cycles was no problem. In practice, even without ski poles, a shelter can be easily erected with 4 or more rescuers arranged in a square. After cardiac arrest was diagnosed, 2 rescuers immediately started CPR and were replaced by the 2 other rescuers in 2-min intervals (Figure 1b). CPR consisted of 30 chest compressions followed by 2 ventilations using the double-C hold technique for bag-mask ventilation. 8 The use of supplemental O2 was practiced in only half the applications (n=24). In locations 1 and 2, O2 was supplied at a flow rate of 15 L/min during CPR. In location 3, CPR was performed without oxygen. Without direct sunlight, visibility inside the shelter was limited. Therefore, all the participants used their own headlamps. Two investigators conducted the measurements, one sitting inside the shelter and the other one observing from the outside. After 15 min of CPR, the scenario was stopped.
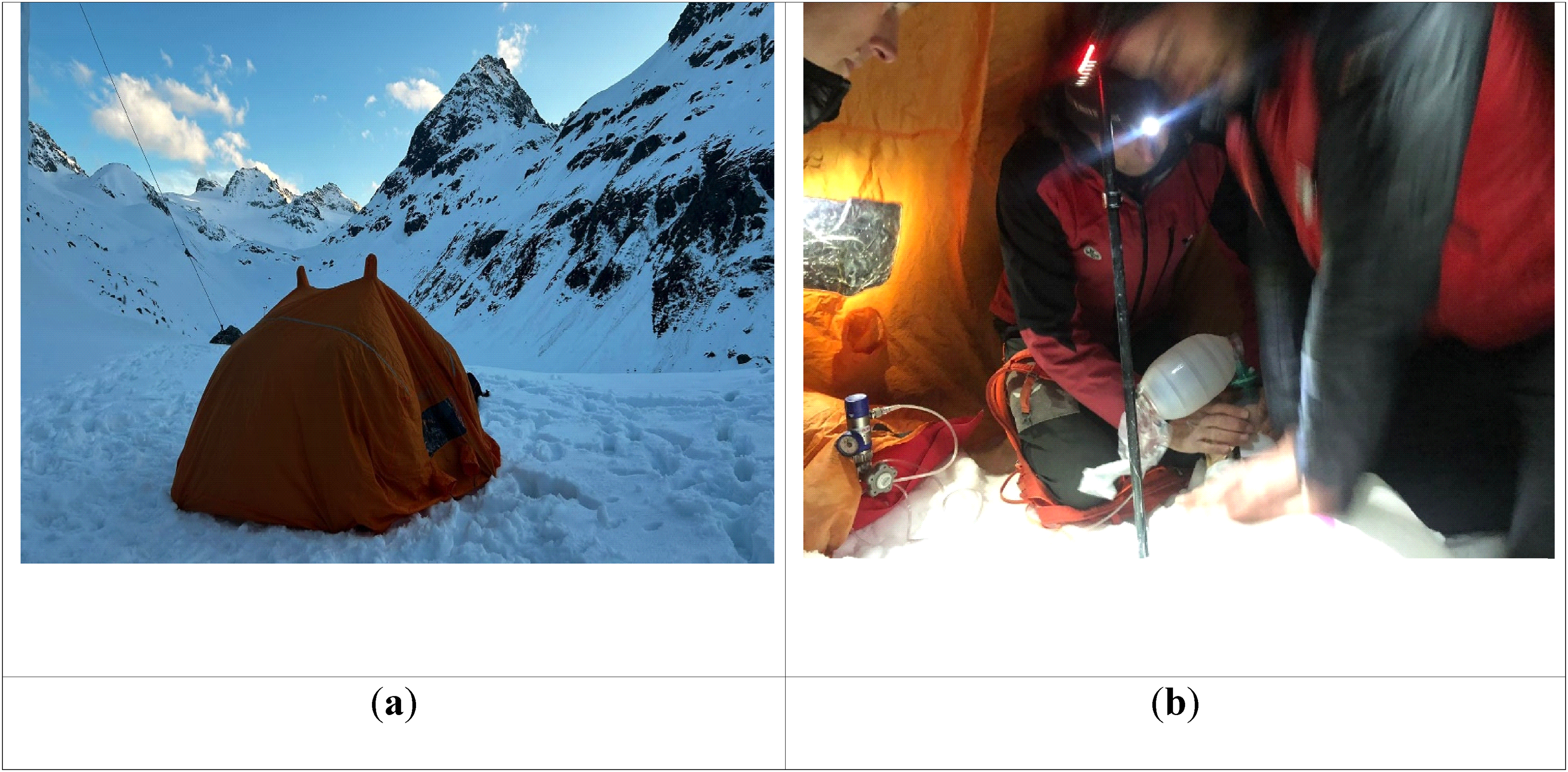
Use of a shelter for mountain rescue in alpine terrain. a, Outside view of the shelter in snow landscape (Jamtal, Tyrol). b, Participants performing chest compressions and bag-valve mask ventilation using the double-C hold technique.
Objective Environmental Parameters in the Shelter
The environmental parameters of air temperature, moisture, and concentrations of CO2 and O2 were measured continuously. The temperature probe was mounted centrally on the inner ski pole with rubber bands. Measurements were taken at ∼50 cm from the manikin's head and ∼80 cm above ground. Temperature and humidity were measured simultaneously using a portable monitor (Testo, 175 H1, 79822 Titisee-Neustadt, Germany). Changes in CO2 and O2 concentrations inside the shelter were measured using a mobile gas detector (Dräger X-am 8000; Dräger Safety AG & Co. KGaA, Lübeck, Germany). The gas detector was placed on the manikin's feet ∼20 cm above ground.
Subjective Assessment of Working Conditions in the Shelter
After 15 min of CPR, the individual satisfaction with use of the shelter was assessed by a questionnaire (see online Supplemental Material). A 5-item Likert-type scale was established to assess stress, moisture, noise, air draft, convenience, spatial confinement, and brightness using scores between 1 (very little) and 5 (very much). For the assessment of air quality and presumed impact on CPR quality, the scores were between 1 (worse) and 5 (perfect), and for assessment of temperature, the scores were between 1 (very cold) and 5 (hot). Participants were not allowed to concur with each other during the study period. In total, 12 test runs were performed, and 48 questionnaires were completed.
Statistical Analyses
Data analysis was performed using SPSS version 28 (IBM Corp, Armonk, NY). Normal distribution of values was assessed by Kolmogorov-Smirnov test. In the case of a normal distribution, a comparison of means and standard deviations was obtained by t test. Median and interquartile range (IQR) as a measure of statistical dispersion were reported for nonnormally distributed data to indicate central tendency. P values <0.05 were deemed significant.
Results
A total of 48 volunteers participated; most were male (91.6%) and between 30 and 60 (62.5%) y of age. All participants completed the study.
Objective Environmental Parameters in the Shelter
During 15 min of CPR, the median temperature rose by more than 15°C (Δt, 15.9 [IQR, 14.3–16.5] °C; P=0.018). The median temperature inside the shelter was 10.9 [IQR, 9.3–14.1] °C) compared with the median temperature outside of −1.2°C (IQR, −7.7 to −0.8°C) (Figure 2).
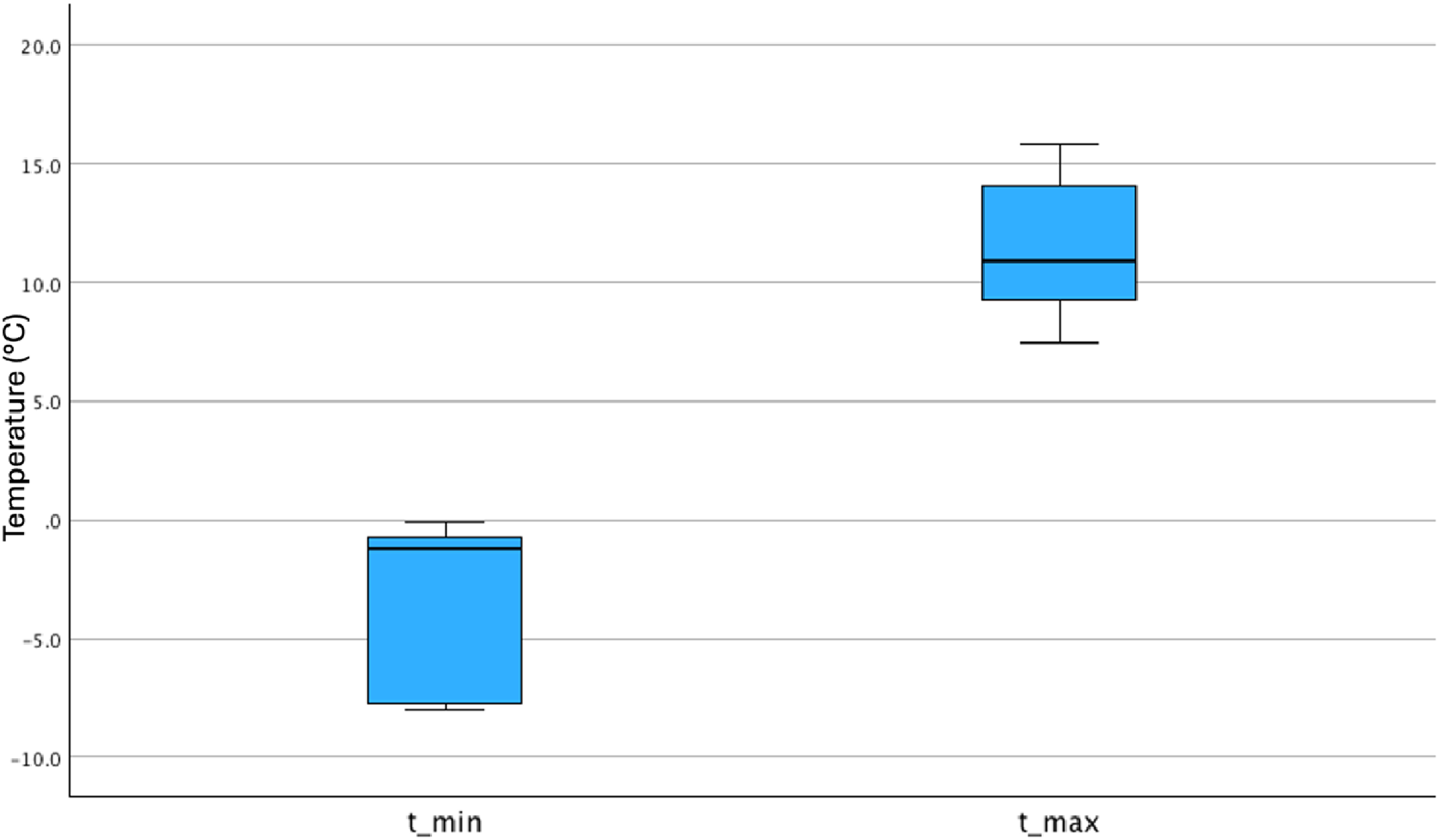
Visualizing range and distribution of median temperature between start (outside the shelter) and after 15 min of cardiopulmonary resuscitation (inside the shelter) with a box plot. Box plot of median temperature and interquartile range in degree Celsius with t_min indicating the temperature measured outside the shelter at the start of the investigation and t_max indicating the maximum temperature measured in the shelter after 15 min of resuscitation.
Relative humidity rose to a median of 93.5% (IQR, 83.4–95.3%). During the investigation interval, CO2 concentrations in the shelter ranged from 0.05 to 0.97 vol% maximum (median, 0.33 vol%). In the subgroup (n=24) using O2 for bag-mask ventilation, the O2 concentration in the shelter was significantly higher compared with the subgroup (n=24) not using O2 for bag-mask ventilation (21.1 [IQR, 20.4–21.8] vol% vs 20.6 [IQR, 20.1–21.4] vol%; P<0.001). Minimum oxygen concentration in the shelter without additional oxygen supply was 19.9 vol%, whereas the maximum value was 22.6 vol% when O2 was used during bag-mask ventilation.
Subjective Assessment of Working Conditions in the Shelter
According to the participants’ own assessments, the median duration of the CPR performance was correctly estimated to be 15 (IQR, 11–16) min.
Overall assessment of working conditions in the shelter was rated positively. Thirty participants (62.5%) rated the convenience inside the shelter as intermediate to very much, and 18 participants (37.5%) rated the convenience inside the shelter as little to very little. High stress was reported only by 1 participant. Four (8.3%) participants complained of moisture inside the shelter. Nine participants (18.7%) complained of low temperature or a disturbing air draft in the shelter, whereas 18 participants (37.5%) rated the temperature inside the shelter as warm (Figure 3). Thirty-six participants (75.0%) rated the noise inside the shelter as low to very low, and they rated the overall quality of air as intermediate to very good. Fourteen participants (29.2%) complained of spatial confinement (Figure 3).
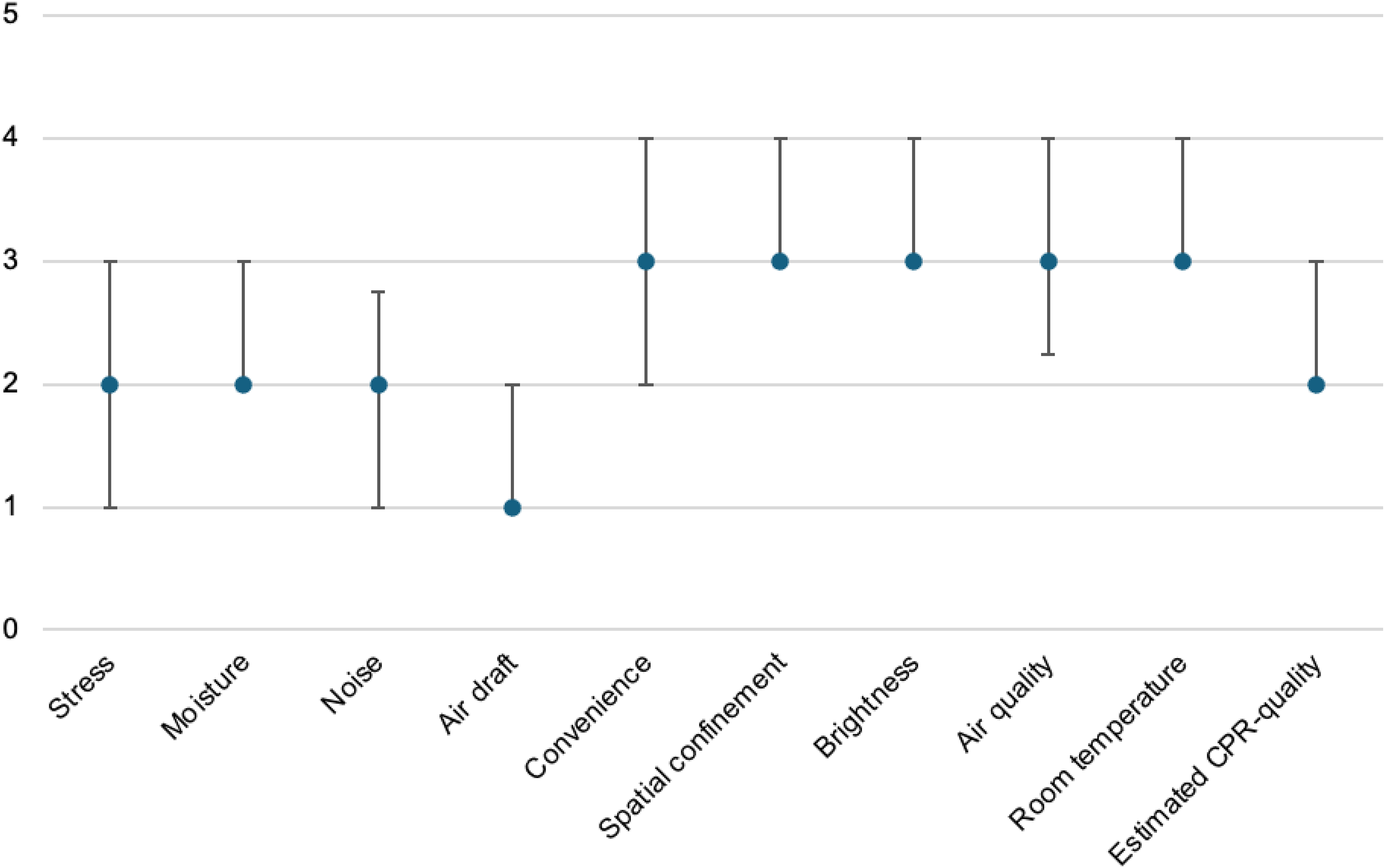
Subjective assessment of working conditions in the shelter from questionnaire responses expressed as median and interquartile range (IQR). Median and IQR of questionnaire responses of 48 users regarding moisture, noise, air draft, convenience, spatial confinement, brightness (1=very little; 2=little; 3=intermediate; 4=much; 5=very much), room temperature (1=very cold; 2=cold; 3=pleasant; 4=warm; 5=hot), and air quality and estimated cardiopulmonary resuscitation (CPR) quality compared with CPR without using a shelter (1=worse; 2=bad; 3=intermediate; 4=good; 5=perfect).
Discussion
In this study it was shown that the use of shelters during CPR in alpine terrains may increase physical comfort and convenience by provision of warmth and by protection against rain, wind, and uncontrolled air leakage. A significant rise in temperature in the shelter was observed during 15 min of CPR in all test runs. This supports the findings of Brugger et al, who reported that shelters in wilderness and mountain rescue may effectively promote hypothermia prevention. 9 Temperature loss from thermal conduction through contact with the ground must not be underestimated. In addition, thermal convection from cold air combined with brisk winds and wet clothing can accelerate heat loss from the body. Hypothermia prevention is crucial in severely injured and seriously ill patients. 2 The limited blood clotting caused by hypothermia and associated acidosis can massively increase blood loss in the event of injuries. 3 Reducing the hypothermic component of the so-called lethal triad in trauma patients improves potential outcomes. 10 However, regarding prehospital resuscitation of cardiac arrest in a nontrauma patient, mild to moderate hypothermia may even be beneficial. Moderate hypothermia in patients with cardiac arrest actually can improve resuscitation outcomes. 11 One reason is that the oxygen requirement decreases by ∼7% for every degree Celsius lower in body temperature. 12 In any case, severe hypothermia leading to cardiovascular instability and cardiac arrest must be prevented. Although a shelter cannot provide effective rewarming, at least it has the potential to minimize heat loss.
Physical stress in rescuers during missions at high altitude is known to be extremely high. 5 Presumably, the ambient heat provided by a shelter can reduce physical stress and may have a beneficial effect on performance. This is especially evident in operations at high altitude, where CPR is very strenuous. 13
Oxygen and carbon dioxide are environmental parameters that can change during measurements in confined spaces with limited fresh air supply inside the shelter. A low oxygen concentration inside the shelter could impair perception and cognitive processes. 14 An oxygen-rich environment from the use of supplemental oxygen potentially can be harmful for defibrillation. Although the risk of significant burns to the patient in oxygen-enriched environment from self-adhesive pads causing sparks between the pads and the skin may be regarded as low, it cannot completely be ruled out. 15 We observed that despite the O2 consumption of 5 people, there was still sufficient O2 in the air of the shelter even when CPR was performed without additional O2 supply. In the case of additional O2 supply (median, 225 L O2), the peak measurement did not exceed 22.6 vol%. This is also important because the slightly increased O2 concentration in the shelter would not have jeopardized the safety of defibrillation attempts from automated external defibrillators.16,17
In contrast to O2 concentrations, the CO2 concentrations increased in the air of the shelter during a 15-min stay of 5 persons. Although the manikin was metabolically inert, an unconscious patient would have contributed to a limited extent to O2 consumption and CO2 exhalation. In our study, the observer in the shelter definitely contributed more to O2 consumption and CO2 exhalation than what could have been expected from an unconscious patient. CO2 is known to be a potent vasodilator that can increase the flow and volume of cerebral blood. 18 However, CO2 concentrations exceeding 5 vol% that could have impaired neuronal function were not observed during the 15-min stay in the shelter. 19 The increased CO2 concentrations inside the shelter during our investigations were not of clinical significance.
In our study, the lightweight shelter has proven to be a valuable piece of rescue equipment in mountain medicine, facilitating emergency medical care of casualties in alpine terrains. Although the single layer of polyurethane-coated polyester has no insulation properties, with 5 persons in the group shelter, the temperature increased rapidly. Thermal sensation is known to change with humidity, but despite the high relative humidity of a median of 93.5% inside the shelter, the subjective and objective assessments of temperature in the shelter were comparable. 20 In the shelter, the occupants were kept out of the elements and benefited physically from each other's warmth. Subjective perceptions of time are known to change in an altered sensory environment, but during a 15-min stay in the shelter, the subjective perception of time did not change noticeably. 21 According to the participants’ own assessments, the median duration of their CPR performance was correctly estimated to be 15 min.
If the stay in the shelter is extended, additional insulating materials on the ground are necessary (eg, rope, rucksack, insulation foils, etc) to minimize conductive losses into the ground. Although not within the primary scope of this study, we suggest a further benefit of using a shelter is to provide a more private environment for rescue. We also expect the use of shelters to be beneficial in prevention of hypothermia in homeless people living in urban areas during the cold season. 22 Furthermore, shelters are valuable in the aftermath of natural disasters. 23
Limitations
There are some limitations that might have influenced interpretation of our findings. We cannot exclude selection bias because the sample size is small and most participants were male. We did not analyze what made contacts choose not to participate in this study. Taking in to account that only the time between the compulsory training units could be used for participation in the study, the rate was reasonably high. We did not investigate prolonged stays in the shelter. Although CO2 concentrations were within acceptable room air concentrations during the 15-min observation, we cannot completely exclude measurement inaccuracies. 24 However, lifting the edge of the shelter could rapidly improve air quality and decrease in CO2 concentrations.
Extreme environmental conditions such as storm and heavy rain may have altered user satisfaction significantly. It is the authors’ opinion that future studies should objectively evaluate the impact of shelters during common scenarios of rescue. Regarding CPR scenarios, the impact on the quality of CPR by assessment of hands-off intervals and compression depths should be examined. Furthermore, CPR in outdoor conditions and CPR inside a shelter should be evaluated in a direct comparison at high altitude.
Conclusion
The use of shelters in alpine terrain may increase physical comfort and convenience while carrying out rescue operations. The rapid increase in temperature inside the shelter by reduced thermal convection and by thermal radiation from the rescuers minimized the risk of hypothermia. An additional insulating mat under the patient would diminish heat loss to the ground through thermal conduction. Shelters appear to be a valuable rescue tool for organized Emergency Medical Services.
Supplemental Material
sj-doc-1-wem-10.1177_10806032241300132 - Supplemental material for Shelters in Alpine Rescue: Can They Create a Comfortable Zone at the Deployment Site?
Supplemental material, sj-doc-1-wem-10.1177_10806032241300132 for Shelters in Alpine Rescue: Can They Create a Comfortable Zone at the Deployment Site? by Willi Troeger, Manuel Winkler, Markus Isser and Wolfgang Lederer in Wilderness & Environmental Medicine
Footnotes
Acknowledgments
We thank the Austrian Mountain Service and Special Police Force for their cooperation and voluntary participation.
Author Contribution(s)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Accessibility Statement
Data further supporting the findings of this study are available from the corresponding author on reasonable request.
Supplemental Material
Supplementary material associated with this article can be found in the online version at https://doi.org/10.1177/10806032241300132.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.