
Abstract
Objective
To quantify awareness of acute mountain sickness (AMS) in a sample of visitors to a North American ski resort and to identify strategies and interest for increasing knowledge of AMS in that population.
Methods
One hundred and thirty visitors to Big Sky Ski Resort, Montana, were surveyed. Demographic data were obtained. Respondents were asked about their current knowledge of AMS and then answered questions designed to quantify their depth of knowledge of the subject. Correct answers were correlated with demographic data. Respondents also answered questions indicating their interest in further education about altitude illness and their preferred modality for obtaining this information.
Results
In general, most respondents were young, 18 to 30 years (62.3%), and male (62.5%). Seventy-six percent had at least some college education and more than 5 years of skiing/snowboarding experience. Only 55% of respondents had some knowledge of AMS, but only 30% had knowledge of AMS symptoms using the Lake Louise Scoring System. About 30% knew the lowest altitude this illness can occur. There was a correlation between educational background and improved knowledge of altitude illness. Half of the respondents desired further information about AMS, and the Internet was the preferred source of information.
Conclusions
This study suggests that a large population of skiers in North America may be relatively naive to the dangers of AMS. The majority of the respondents were interested in learning more about altitude illness, and the Internet was the most attractive source of information.
Introduction
Altitude illness refers to a constellation of symptoms such as headache, nausea, dizziness, and insomnia brought on by rapid ascent to elevations typically above 2000 m (6562 feet). At altitudes of 2000 m to 2500 m (6562–8202 feet) the incidence of acute mountain sickness (AMS) has been reported at 25%. 1 This rate increases precipitously the higher and faster a person ascends. The reported incidence of AMS at 4550 m (14 927 feet) in people not previously exposed to altitude within the previous 3 months is 58%. 2
Many ski resorts in the western United States (US) have skiable terrain exceeding 3300 m in altitude, and millions of skiers travel from across the world to ski at these elevations. In the 2006–2007 ski season, there were more than 55 million skier visits in the United States, and more than 20 million of those visits were to resorts in the Rocky Mountains. 3 This number has been increasing yearly since 1979, putting many skiers each season at risk for developing AMS.
In 2002, Glazer et al 4 surveyed trekkers in Nepal to quantify awareness of AMS. In general, trekkers with more years of experience and who traveled to higher altitudes had better AMS awareness. Currently, no study has examined altitude awareness in visitors to US ski resorts. This study was designed to identify altitude awareness in visitors to a western US ski resort. A secondary goal of this study was to broaden experience with the survey instrument used on the trekkers in Nepal.
Methods
Our prior survey initially used for trekkers in Nepal 4 was modified to be applicable to visitors to US ski areas. Big Sky Resort in Big Sky, MT, was chosen as a site because it is easily accessible through most major domestic airlines, and its base elevation of 2286 m (7500 feet) and the peak tram elevation of 3403 m (11 166 feet) offer risk for developing AMS.
A convenience sample of visitors was approached in the base lodge at the resort during January 2006. Visitors were invited to participate in the study. Researchers were scripted to describe the study as “an anonymous survey of awareness of acute mountain sickness.” Participants were excluded if they declined to complete the survey, if they could not read English, or if they were younger than 18 years old. Eligible individuals were provided a written survey instrument (see the Appendix available at
Demographic data such as age, nationality, residence, educational status, level of experience, and number of visit days per year were obtained. Knowledge of the maximum altitude the respondents attained or would attain at their visit to Big Sky Resort was examined. Respondents were asked a variety of questions (9 total) designed to identify their understanding of the basic concepts of AMS (Appendix questions 14, 16, 18–20, 24–27). A correct answer to the symptoms question (#18) required selection of headache plus at least 2 other qualifying symptoms (maximum score = 7) as defined by the Lake Louise Scoring System. 5 Participants were also asked questions about the lowest altitude at which AMS can occur (3000 m) and what factors contribute to this illness. A correct answer to the latter question required the respondent to mention either gaining altitude too quickly or sleeping at a high altitude. Answers were correlated with demographic data.
In addition, respondents were asked to estimate the percentage of skiers in the United States affected by AMS. This was compared with their estimate of skiers affected yearly by avalanches. A clinical vignette was included to identify potential respondent actions in an AMS scenario. Finally, respondents answered questions indicating their interest in further education about altitude illness and their preferred modality for obtaining this information.
This study was granted an exemption by the Maine Medical Center Institutional Review Board committee as the survey did not include any identifying data. The requirement for obtaining informed consent was waived.
Analysis
Results were collated and analyzed by SPSS software. Deidentified data were summarized using means and proportions. The data were analyzed to assess the proportion of respondents who had knowledge of altitude and altitude sickness. All survey responses were entered into an Excel data base and then imported to an SPSS program for analysis (version 12.0 for Windows). P values were calculated using a χ2 test to compare the demographic data and altitude awareness scores. Nominal regression analysis was also performed using multiple demographic parameters. Results with P < .05 were considered significant.
Results
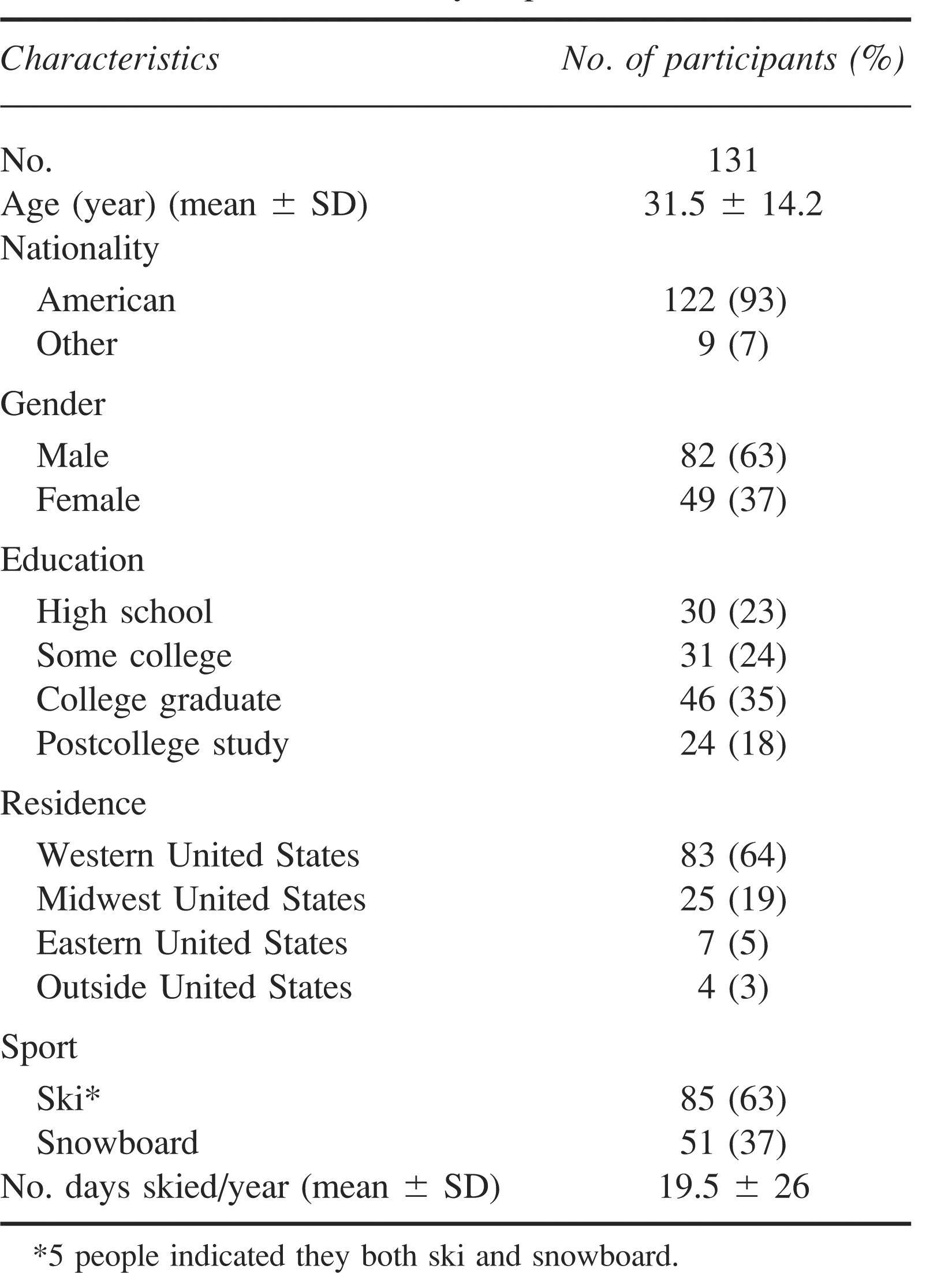
One hundred and thirty visitors responded to the survey for a response rate of 92% (130/142). The Table presents the baseline characteristics of the respondents. The average age was 31.5 years (SD ± 14.2 years). Almost two thirds of respondents (63%) were male. Seventy-six percent reported at least some college education and more than 5 years of skiing or snowboarding experience. More than half (56%) claimed to ski at least 10 days per year and 64% (n = 83) lived primarily in the western United States. Nineteen percent (n = 25) were visiting from the Midwest and 5% (n = 7) lived in the East. Only 3% (n = 4) of responders lived outside of the United States.
Characteristics of survey respondents
Respondents had limited knowledge of their current level of altitude. Only 40% (n = 53) knew approximately the maximum altitude to be achieved during their visit. Very few, 14% (n = 18), had ever traveled to altitudes above 4267 m (14 000 feet). Overall, respondents had a poor understanding of altitude illness. Just more than half, 55% (n = 71), claimed they were aware of AMS, but only 8% (n = 10) reported ever having experienced symptoms. Less than half, 48% (n = 63), were aware that gaining altitude too quickly or sleeping at high altitudes are the contributing factors in developing altitude illness. Interestingly, 66% (n = 86) and 69% (n = 90) were aware that AMS can be prevented and treated, respectively. Yet, when given an AMS scenario, only 56% (n = 73) of respondents correctly assessed the situation. Fourteen respondents (11%) correctly identified either acetazolamide or dexamethasone as pharmaceutical treatment options for a person with AMS.
As was described in the previous study by Glazer et al, we attempted to identify differences between highly knowledgeable respondents and those respondents who had little knowledge. Respondents with a higher number of correct responses to the 9 AMS concepts questions tended to have more education than respondents with a lower number of correct responses (P < .05). Age, gender, sport, having more than 10 years of experience, or number of days skied per year did not predict more correct answers. Nominal regression analysis on skiers having more than 10 years of experience, however, did show a statistically significant higher number of accurate responses (P < .05).
Respondents’ assessment of AMS risk was also poor. Whereas the average estimate was 12% (SD ± 16.7), which was lower than the actual risk of around 25%,1,6,7 the range of estimates was large (0.1%–90%). Participants’ estimation of the percentage of resort skiers dying in an avalanche was even more inaccurate at 3% (SD ± 5.3) (range 0.01%–32%) given an estimated real risk of 1 in 14.5 million.3,8
When asked whether they would like to learn more about AMS, 50% (n = 65) responded they would be interested in more information. The overwhelming majority of respondents identified the Internet as the modality of choice for obtaining this desired information.
Discussion
The nature of recreational skiing provides ideal conditions for putting athletes at risk for developing AMS. Skiers commonly travel from home altitudes below 1000 m (3280 feet) to lodging altitudes of 2000 m to 3000 m (6560–9842 feet) and then exercise at altitudes higher than 3500 m (11 482 feet) without acclimatization. Though many studies have demonstrated that AMS can be easily treated, AMS prevention should be the primary approach to managing this condition. Prevention, however, relies on awareness. No previous studies have attempted to measure awareness levels among recreational skiers.
Additionally, highly publicized altitude accidents in rarefied environments such as Mt Everest may serve to underemphasize the risk of AMS at lower elevations. Glazer et al showed that, on average, trekkers ascending to altitudes higher than 4600 m (15 091 feet) were naive to the dangers of AMS. Our study confirmed that the majority of recreational skiers surveyed had little knowledge of the risk of AMS. On average respondents greatly overemphasized (10 000 fold) their risk of dying in an avalanche, suggesting that sensational news accounts may contaminate skiers’ assessment of risk.
The pathophysiology of AMS is not well understood, and currently risk models are based on empiric observations. Major predictors of increased risk seem to be having residence at or near sea level or having a personal history of previously developing AMS, 1 whereas other conditions such as poor physical fitness, cardiovascular disease, and chronic pulmonary disease do not seem to confer any increased risk. 9 Higher physical fitness levels have no effect on preventing AMS. 10 These issues may lead to a false sense of safety for already naive recreational skiers who are healthy and physically fit. Such skiers may falsely assume their risk is lower than the majority of other skiers.
This study, based on a small sample of visitors to a North American ski resort, suggests that a large population of people at risk for AMS is relatively unaware of the danger. Generally, many respondents did not know their current altitude, the specific symptoms of AMS, and at what altitude these symptoms can occur. This was true despite our sample's generally high level of education. Certainly many skiers at the Big Sky ski resort achieve altitudes sufficient to cause AMS, and poor altitude awareness places these visitors at increased risk for developing AMS. Respondents in this study completed the survey at an altitude where previous studies have shown an incidence of AMS at about 25%, but only 8% actually reported experiencing AMS symptoms. This would either suggest a lack of true understanding of the symptoms and predisposing factors associated with AMS or may be due to the high percentage of visitors from the West who may already be acclimatized to altitude. It is unlikely that this represents a lower incidence of AMS at this altitude. This study was not designed to identify the incidence of AMS at the Big Sky ski resort, and it is not known what the true incidence of AMS was at this ski resort during the month the survey was conducted.
A secondary objective of our study was to increase experience with the altitude awareness survey. Given the consistency between responses in the prior survey and our survey, this suggests the validity of this survey instrument at determining awareness of AMS. Although this survey was not as comprehensive as the previous survey, the core AMS knowledge questions remained the same. In each study, both trekkers and visitors to a ski resort were generally naive to AMS, and there were similar correlations between years of experience and increased AMS knowledge. Neither study demonstrated that age or gender had a significant impact on the altitude awareness score.
Some respondents did not indicate a desire to learn more about AMS. Given the generally poor knowledge of AMS, it appears that some people are uninformed and may not realize that they should become better educated. In addition, since at least one third of respondents did not realize that AMS could be prevented, a large population of visitors would benefit from further knowledge regardless of whether they realize it. This fact, combined with the importance prevention has upon AMS incidence, suggests that the outdoor community may be able to decrease the morbidity of AMS through educational measures. Information could easily be distributed on the Internet, which was the modality of choice among our respondents. Having this information available on a ski resort's website could enable preemptive planning and increase awareness of the risks of AMS among skiers before their exposure.
This study is limited by the fact that only visitors to one resort were surveyed. The results may not be representative of the average visitor to other ski resorts. A larger, multicentered study could provide a better understanding of whether this population of respondents represents the average North American alpine athlete. It is also possible that awareness could be higher in resorts with educational programs about AMS.
Future studies aimed at outcomes of reducing the morbidity of AMS would also be helpful. Imray et al 11 showed that education about AMS in adolescents was helpful in self-monitoring for AMS and identifying when treatment should occur. These data suggest that the general population may benefit greatly from widespread educational interventions. The pervasiveness and ease of Internet access provides an ideal modality for education. Simple modules could educate recreational skiers about AMS and improve prevention.
Footnotes
Acknowledgments
We would like to acknowledge Dr Jeffery Daniels, Medical Director of the Medical Clinic of Big Sky, Big Sky, MT, for his support and assistance with this project.