
Abstract
Objective
To measure the incidence of acute mountain sickness (AMS) in adolescents travelling to moderately high altitudes.
Methods
The study was carried out on a cohort of 63 adolescents with an average age of 15.9 years during an 8-day trip to Morocco, travelling to altitudes between 3106 m and 4167 m. The incidence of AMS was calculated using the Lake Louise questionnaire, which was completed twice daily by each participant. An episode of AMS was defined as being a score of 3 or more on the Lake Louise questionnaire in the presence of a headache. Difference in incidence between boys and girls was analyzed using 2-tailed Mann-Whitney U testing.
Results
The daily incidence of AMS among 52 participants with complete data was found to be between 3.8% and 42.3% and increased with increasing altitude. Girls had a statistically significant higher incidence of AMS (80%) compared with boys (55%) (P < .01).
Conclusions
Acute mountain sickness may occur more commonly in female adolescents than in male adolescents. Overall, however, it appears that the incidence of AMS in adolescents is similar to that found in adults in previous studies.
Introduction
Acute mountain sickness (AMS) is a well-recognized phenomenon in people travelling to high altitudes. The syndrome is characterized by symptoms of headache, nausea, or vomiting; dyspnea; fatigue; poor appetite; dizziness; and difficulty sleeping. 1 It has been observed at elevations of 2500 m or higher. Very few studies have been published that examine the incidence of AMS in adolescents. Over the last 30 years, several important studies have examined the incidence of AMS in adult travelers going to high altitudes. The incidences recorded have ranged from 25% in travelers at 2975 m2 to 68% in travelers at 5671 m. 3 Acute mountain sickness has been recorded in both adults and children, but the relative incidence in children and adolescents compared with adults remains controversial. Hackett et al found younger trekkers were more susceptible to AMS. 4 Honigman et al observed an incidence of 45% in those aged between 16 and 19 years (compared with an overall average of 25%). 2 A study of children (6–48 months), adolescents (13–18 years), and adults (more than 18 years) in Northern Chile at 4400 m reported incidences of 100%, 50%, and 27%, respectively. 5 Imray et al found that 91.7% of adolescents had Lake Louise scores consistent with AMS when travelling to 5500 m in Peru. 6
The aim of this study was to examine the incidence of AMS, using the Lake Louise questionnaire, in a group of adolescents aged 13 to 18 years travelling to elevations from 3106 m to 4167 m in Morocco. Travel to high altitude is becoming increasingly common, and it is important to understand the associated risks for young people.
Methods
Study Group
The participants in this study were 63 British schoolchildren (30 girls and 33 boys) aged between 13 and 18 years (average 15.4 years) travelling from the UK to the High Atlas Mountains in Morocco. All participants resided in the UK at elevations less than 1500 m. The participants travelled in 5 separate groups, each for a period of 8 days. Trips started in October, March, or April. Each participant was given an information sheet on the study and signed a consent form prior to taking part. At the time the study was conducted, the work was exempt from the requirement for IRB approval. None of the participants took medication for the prophylaxis of AMS such as acetazolamide.
Group Itinerary
All groups flew directly from the UK to Marrakech (428 m), where they spent 1 night. They then took a 2-hour bus journey to Aroumd (2047 m) and spent 2 nights there for acclimatization, which included a day hike (to approximately 2300 m). After this the groups trekked for a period of approximately 6 hours to a campsite at 2719 m or to the Neltner refuge (3106 m). Two of the 5 groups managed to reach the summit of Mount Jebel Toubkal (4167 m). However, for the remaining groups, snow conditions made the trek too hazardous. After trekking in the Toubkal Massif region, each group returned to Aroumd for 1 night before descending to Marrakech for a further night prior to return to the UK. Figure 1 shows the sleeping elevations over the course of the trip.
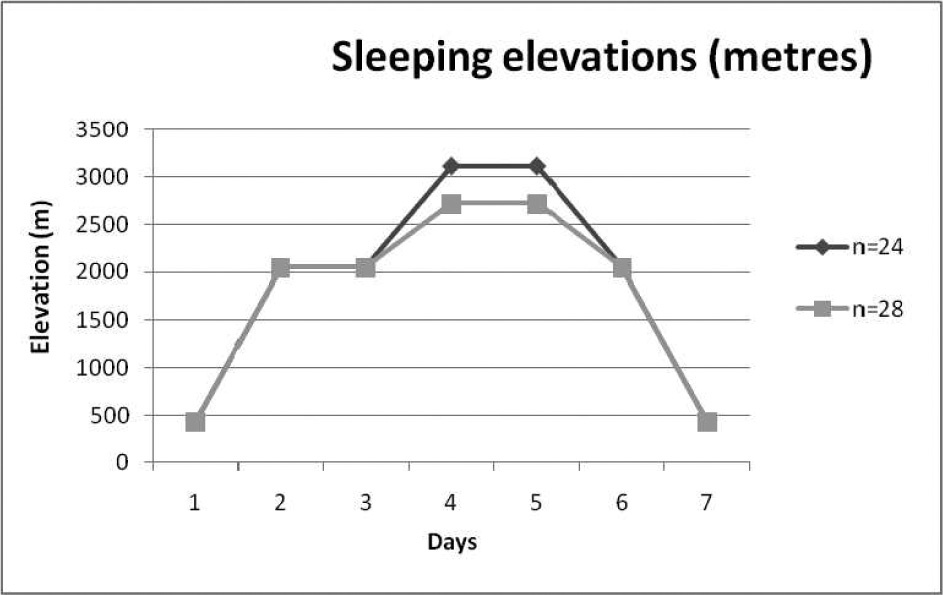
Sleeping elevations.
Acute Mountain Sickness Questionnaire
Each individual was given a Lake Louise self-reported questionnaire to be completed twice daily. The completion of this form was supervised by the adult group leaders. Two of the groups were led and supervised by one of the authors (J.D.). Groups started to record data on arrival in Marrakech. Details of age and sex were recorded on the sheets. The Lake Louise scores were measured in the morning and evening for each individual. Total scores of 3 or more, in the presence of headache, were taken to indicate the diagnosis of AMS.
Statistical Analysis
A 2-tailed Mann-Whitney U test was carried out to investigate the difference in the number of episodes of AMS during the expedition.
Results
The response rate was 82.5%, with 52 of 63 participants returning all questionnaires fully completed (30 girls and 22 boys).
In this study, 37 (71%) experienced at least 1 episode compatible with AMS over the 8-day trip. Thirty percent of participants had Lake Louise scores compatible with AMS on initial arrival in Marrakech at 428 m elevation.
The daily incidence of AMS ranged between 3.8% (on return to Marrakech) and 42.3% (which corresponded with the maximum altitude gained) (Figure 2). Twenty-four individuals in 2 groups reached the summit of Jebel Toubkal at 4167 m (17 girls and 7 boys). Of these summiteers, 70.6% of the girls and 57.1% of the boys had AMS. Sixteen participants only reached a maximum elevation of 3800 m because of difficult snow conditions, and 1 group (n = 12) only reached a maximum height of 3106 m, again because of the snow conditions.
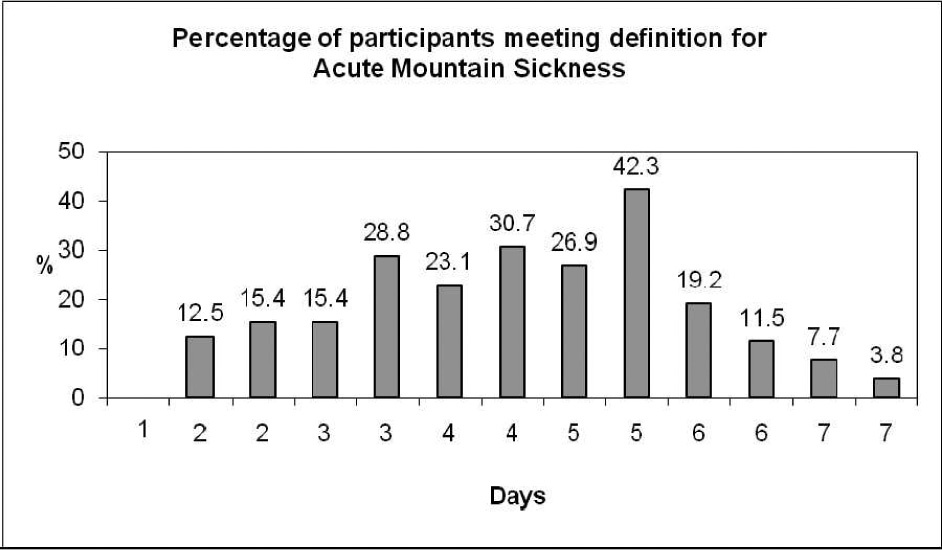
Percentage of participants meeting the definition of acute mountain sickness.
The number of episodes of AMS per participant was higher for the girls, with a median of 3 episodes per girl for the whole trip or 2 episodes excluding the first day when the group arrived in Marrakech (428 m), compared with a median of 1 episode for the boys. This was statistically significant, with P values of .008 and .016, respectively. The proportion of girls who had scores compatible with AMS on the expedition was 83% and 55% for boys. This fell to 80% for girls and 55% for boys when the first day was omitted.
The percentage incidence of AMS in the participants is shown in Figure 3.
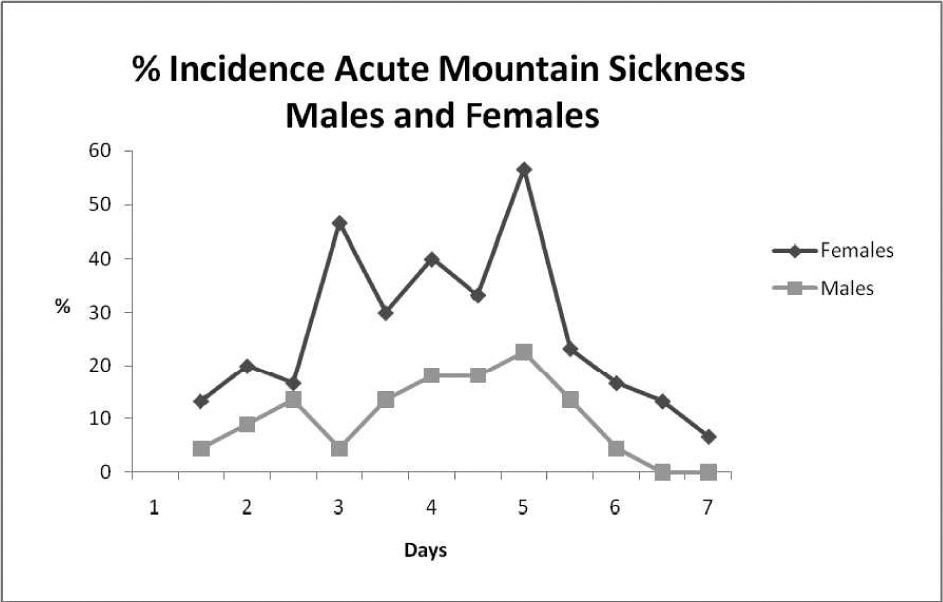
Percentage incidence of acute mountain sickness in boys and girls.
Discussion
The daily incidence of AMS, defined as a Lake Louise score of more than 3 with headache, in this sample of adolescents ranged between 3.8% and 42.3%. There was a 30% incidence of symptoms compatible with AMS on arrival in Marrakech (428 m), but at this elevation it is likely that symptoms of headache, tiredness, and nausea were related to other factors, such as the long flight, dehydration, or the effects of the heat. As expected, the incidence of AMS increased with increasing elevation, rising to a peak of 42.3% when the maximum elevation was reached. The percentage of participants with scores consistent with AMS then declined again as the participants descended, reaching 3.8% on return to Marrakech.
A large number of studies have been conducted looking at AMS rates in adults, giving rise to a variety of incidence rates. These include the study by Hackett et al, which gave an incidence of 53% at 4243 m. 4 Examining 466 climbers at various altitudes in the Alps, Maggiorini et al detected a positive correlation between altitude and incidence of AMS, 13% at 3050 m, 34% at 3650 m, and 53% at 4559 m. 7 At intermediate altitudes in the Rocky Mountains, an overall incidence of 25% was calculated. 2 It is likely that the spectrum of incidence rates found over the years may be due to the number of variables that contribute to the development of altitude sickness (eg, rate of ascent, maximum altitude reached, residence at or near sea level). In this study, the daily incidence ranged between 3.8% and 42.3%, which is comparable to that found in studies of adult populations.
Few studies have directly examined the incidence of AMS in adolescents. Imray et al found that in a group of 12 adolescents taken to an altitude of 5500 m, 91.7% recorded a Lake Louise score of greater than 3 on at least 1 day. 6 A prevalence rate of 71% can be calculated with the data from this study in Morocco. Imray et al suggest that their high prevalence rate may be the result of the small study size (only 12 participants) or because of the ascent profile that the participants undertook. The participants in their study reached higher altitudes than those taking part in this study.
In the study by Honigman et al, a higher incidence of AMS was recorded in the teenage population of their sample (45% compared with 25% in the adults). However, this age group constituted less than 1% of the total 3158 participants. 2 Hackett et al studied 278 hikers in Nepal and demonstrated a negative correlation with age. 4 Moraga et al also recorded a greater incidence in the adolescents that took part in their study (50% compared with 27% in adults). 5 In all of these studies, the sample size of adolescents was small.
Several other studies, however, have shown that AMS levels in adults and children are comparable. Theis et al examined 558 children aged 9 to 14 years at 2835 m and found an AMS incidence of 28%, a figure comparable with that found in adults at similar altitudes. 8 In 459 Iranian trekkers to 5671 m, Ziaee et al found no association between age and incidence of AMS (31 members of the study group were aged under 19 years). 9
Some studies have found a difference in the incidence of AMS between boys and girls,2,6 and others have not.3,4,7 This study at moderate elevations in Morocco showed a clear difference between the incidence in boys and girls. The reasons for apparent differences in the occurrence of AMS in this group are not clear. It may be that boys were less likely to record symptoms of AMS, or there actually may be a true sex difference in incidence.
The limitations of this study include its relatively small sample size, although it is the largest study of its kind to date. The use of a greater number of participants may have given a more reliable indicator of the incidence of AMS. The incidence of AMS may be underestimated; some participants may not have completed their questionnaires accurately because they were feeling too ill or tired, and some adolescents may be unreliable when completing self-scored questionnaires. A further difficulty encountered was that the different groups did not all follow identical ascent profiles due to poor weather conditions.
An additional problem in analyzing the results of this and other studies is that the symptoms of AMS are nonspecific and other factors may account for the symptoms experienced. For example, Theis et al looked at a group of children at sea level, where AMS symptoms were reported in 21% of the study sample. 8 In our study, 30.0% experienced symptoms similar to AMS on initial arrival in Marrakech (428 m). It is possible that confounding factors, such as change of daily routine, dehydration, and lack of sleep, may account for symptoms (eg, headache, fatigue) recorded in individuals not at altitude. These results also highlight the difficulties in measuring and diagnosing AMS. 9
Conclusions
This study has demonstrated that adolescents, like adults, are vulnerable to the effects of altitude, and these data can be added to the growing evidence on AMS to help educate travelers and their care providers in these areas. This study suggests a significant difference in the incidence of AMS between male and female adolescents. To build on the evidence from this and other studies of AMS in adolescents, further research focused on a cohort of both adults and adolescents following a similar ascent profile may allow any true difference to be identified. Larger numbers of adolescent participants would demonstrate any significant sex difference.
Footnotes
Acknowledgments
The authors gratefully acknowledge the help with statistical analysis from Professor Jonathan Benger and Dr Rosemary Greenwood. This work is attributed to the Department of Emergency Medicine, Bristol Royal Infirmary, Bristol, United Kingdom.
1
Dr Dallimore is a professional medical advisor to the expedition company.