
Abstract
Objective
It is well established that a combination of factors, including ethnicity, may influence an individual's response to cold stress. Previous work from our laboratory has demonstrated that when faced with a cold challenge, there is a similar response in heat production between Caucasian (CAU) and African American (AA) individuals that is accompanied by a differential response in core temperature. The objective of this study was to evaluate the influence of ethnicity (CAU vs AA) on the thermoregulatory response after acute cold exposure (ACE-REC, 25°C air).
Methods
Five AA males (20.8 ± 0.5 years) and 10 CAU males (25.6±4.9 years) underwent pre-experimental testing to determine V
Results
Analysis of variance for ACE-REC revealed a significant main effect for Tsk across time (P < .001), Tre across time (P < .001), and V
Conclusions
Based on these data, there is a differential response between CAU and AA across time for V
Introduction
When an individual is exposed to environmental temperature extremes, the challenge is to maintain thermoregulatory homeostasis. Humans attempt to maintain thermoregulation through the integration of different mechanisms, acting in concert with a variety of contributing factors. The primary physiological responses include an increase in metabolism (shivering thermogenesis), an alteration in the vasomotor response (peripheral vasoconstriction/vasodilation), 1 and a circulatory response (countercurrent heat mechanism). Additionally, such factors as fitness level, body composition, age, gender, and race may also influence the individual's ability to thermoregulate. 2 –7
An understanding of how different individuals thermoregulate is valuable to those who engage in outdoor activities for prolonged periods. The majority of current literature in the field focuses on the cold exposure portion, whereas little research has examined the recovery phase. Acute cold exposure (ACE) has been shown to increase the clotting response during the recovery period, making individuals more susceptible to negative cardiovascular events, 8 –10 such as heart attacks and strokes. Research in the area of cold exposure has also focused primarily on the Caucasian (CAU) male with very little research available concerning different ethnicities and how they may thermoregulate to the stressor of cold.
It has been well documented that African Americans (AA) suffer a disproportionately higher rate of cardiovascular disease. 11 Cardiovascular reactivity has also been shown to be greater among AA after a variety of stressors. 11 Further, it is unclear whether morphological or ethnic differences cause potential alterations in cold responsiveness between groups or whether the alterations are due to differences in thermosensitivity. McArdle et al suggests that the differences in thermoregulation at rest during cold stress may be due in part to the sensitivity of the thermogenic response. 12 Previous work from our laboratory has demonstrated that CAU individuals thermoregulate to cold stress by maintaining a higher metabolic rate than their AA counterparts. 1 Although numerous studies have demonstrated that certain physiological changes may ensue with cold stress, research in the area of ethnicity and how the individual may respond to this stressor is limited.6,13–18 Therefore, the impact of ethnicity (eg, AA vs CAU) on thermoregulation warrants investigation. In an effort to establish possible differences that are involved in thermoregulation, the recovery phase of acute cold exposure (ACE-REC) was explored to discern if individuals who varied on the basis of ethnicity would demonstrate a differential response after ACE. In this differential response, the return of cooled peripheral blood after ACE for 120 minutes may elicit differences between individuals based on ethnicity.
In an effort to establish possible differences involved in thermoregulation between AA and CAU males, we studied ACE-REC to evaluate whether there is a differential thermoregulatory and metabolic response after ACE in individuals of these races.
Methods
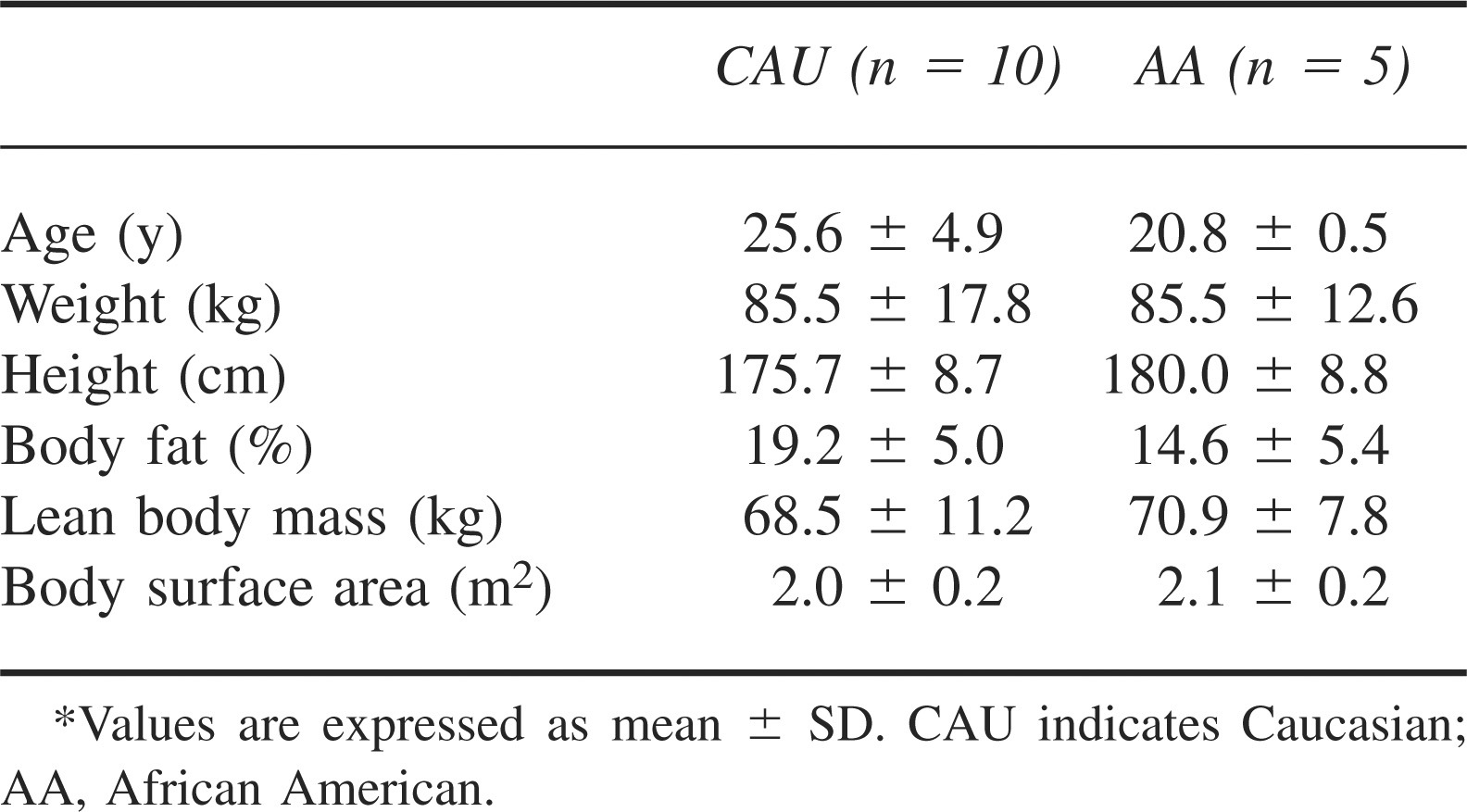
Fifteen males (5 AA, 10 CAU) participated in this study. Participant characteristics are presented in Table 1.
Study group participant characteristics*
Each participant experienced 120 minutes of exposure to 10°C air (ACE) and recovery (ACE-REC) wearing only a swimsuit for 120 minutes or until rectal temperature (Tre) was ≤35°C. The complete air exposure trial consisted of 3 periods: a 15-minute baseline (BASE) period followed by a 120-minute ACE, followed by a 120-minute recovery (ACE-REC) in 25°C air. Throughout the ACE and ACE-REC, Tre, skin temperature (Tsk), expired air, and heart rate (HR) were continuously monitored and metabolic rate (V
Baseline Period
Upon arrival to the Applied Physiology Laboratory, participants had their body weight measured. They were then instructed to insert a rectal probe (ER400-12, Respiratory Diagnostic Products Inc, Irvine, CA) 13 cm beyond the anal sphincter for the purpose of monitoring Tre. Participants were also outfitted with skin thermistors (Model #409B, Yellow Springs Instruments Inc, Yellow Springs, OH) to measure mean skin temperature. Temperature-sensing thermistors were placed on the tricep, chest, thigh, calf, and forearm and secured with Hy-tape waterproof tape (Hy-tape International, Patterson, NY) for the purpose of collecting Tsk data. Rectal temperature and Tsk thermistors were then interfaced with a data acquisition system (iNet-100HC, Omega Engineering Inc, Stamford, CT), which was interfaced with a desktop computer. Mean skin temperature was calculated using the weighted formula used by Ramanathan. 19 Rectal temperature and Tsk data were monitored continuously and recorded every minute.
After instrumentation, the participant sat quietly, with arms and legs extended and separated, in a semirecumbent position on a plastic lounge chair outside of, and next to, the environmental chamber in a 24–26°C air environment for 15 minutes. During the BASE period, expired air samples, Tre, Tsk, V
Cold Air Exposure/Recovery Period
After completing the BASE period, participants were rolled into the environmental chamber, where they were required to remain seated and quiet in the chair with limbs separated and extended while exposed to 10°C cold air for 120 minutes. Rectal temperature Tsk, V
Statistical Analysis
Statistical analysis was performed using a 2-way analysis of variance, 2 (group [CAU and AA]) × 6 (time [BASE, 0, 15, 30, 60, 90, and 120 minutes]) with repeated measures for time. An independent t test was used to analyze participant characteristics (anthropometric variables, V
Results
Fifteen volunteers (5 AA males [20.8 ± 0.5 years], 10 CAU males [25.6 ± 4.9 years]) were recruited to participate in the current study and successfully completed all experimental trials of 120 minutes of ACE followed by 120 minutes of ACE-REC. The groups did not differ statistically with respect to percent body fat (AA = 14.6 ± 5.4%, CAU = 19.2 ± 5.0%). Both groups were similar in height and weight, as well as in lean body mass and body surface area. Likewise, the groups did not differ significantly with respect to maximal oxygen consumption (AA = 37.2 ± 0.1 mL·kg−1·min−1, CAU = 44.3 ± 8.7 mL·kg−1·min−1).
Rectal Temperature
Figure 1 shows a significant difference in Tre (P = .008) between the 2 groups. Posthoc analysis demonstrated significant time × ethnicity interactions (ie, significant difference between groups across time) for Tre at 0 (CAU 36.9 ± 0.3°C, AA 36.5 ± 0.3°C), 30 (CAU 36.7 ± 0.4°C, AA 36.2 ± 0.4°C), 60 (CAU 36.6 ± 0.3°C, AA 36.1 ± 0.4°C), 90 (CAU 36.6 ± 0.4°C, AA 35.4 ± 0.4°C), and 120 (CAU 36.6 ± 0.2°C, AA 36.0 ± 0.4°C) minutes of ACE-REC, during which the AA participants demonstrated a lower Tre. Additionally, a main effect for time (ie, significant difference across time) was demonstrated (P < .001). As ACE-REC time increased, Tre decreased.
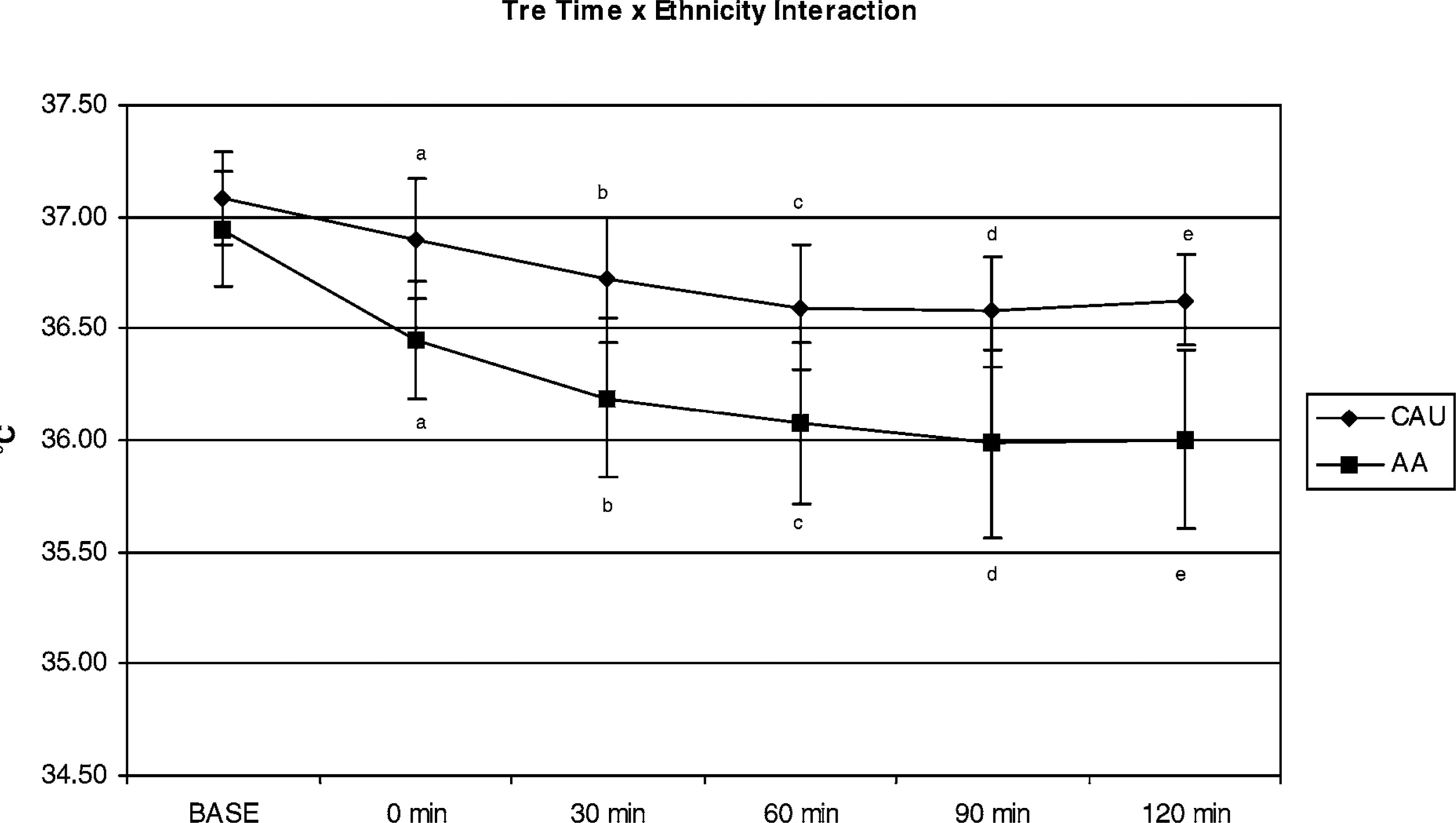
Time × ethnicity interaction for rectal temperature during recovery (P = .008). *
Mean Skin Temperature
Figure 2 shows a significant difference in Tsk (P = .042) between the 2 groups. Posthoc analysis demonstrated significant time × ethnicity interactions for Tsk at 60 (CAU 27.6 ± 0.4°C, AA 27.0 ± 0.6°C) and 90 minutes (CAU 28.2 ± 0.4°C, AA 27.5 ± 0.3°C) of ACE-REC, during which the AA participants demonstrated a lower Tsk. There was also a significant (P < .001) main effect for time for Tsk. As ACE-REC time increased, Tsk increased.
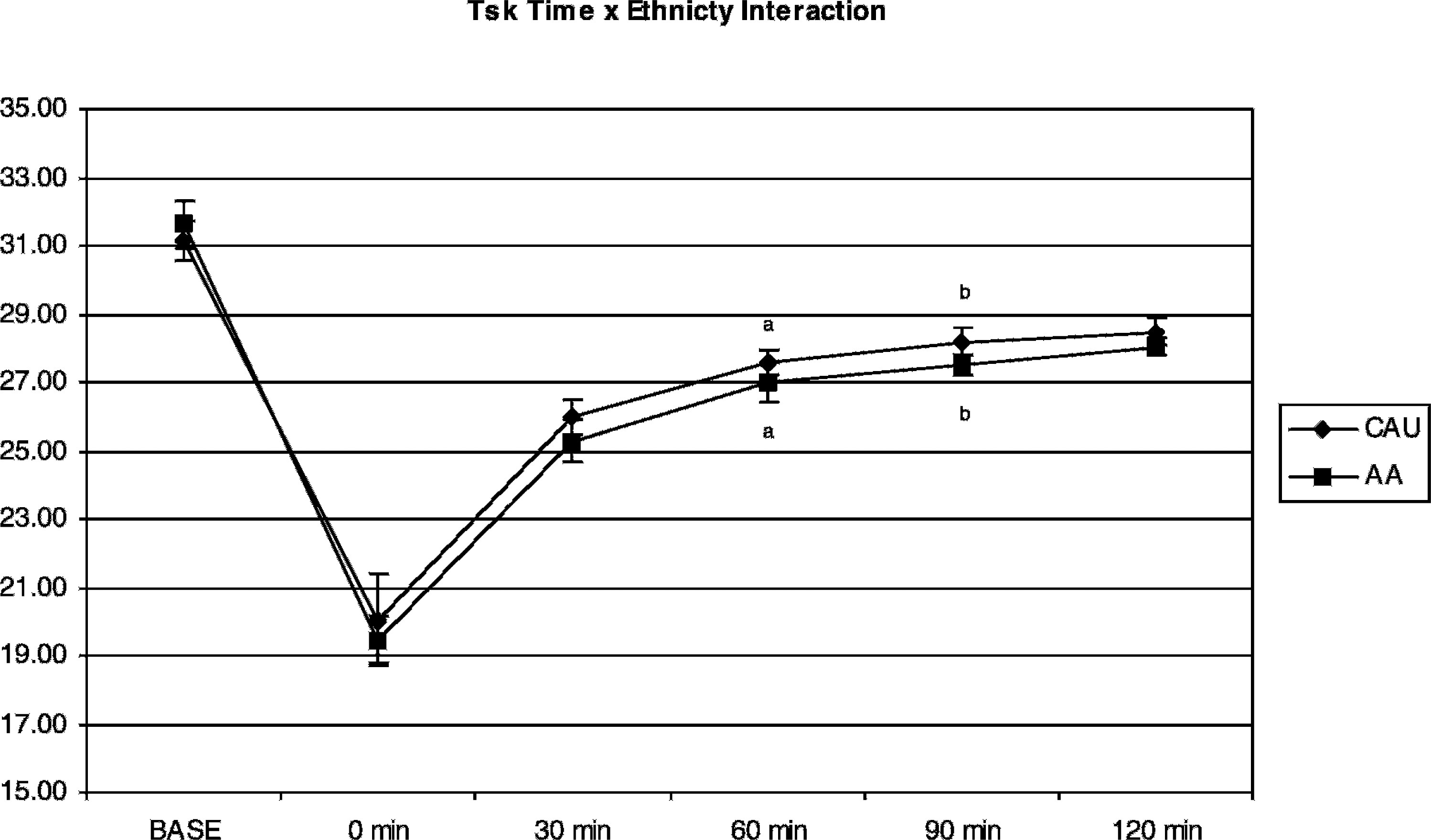
Time × ethnicity interaction for skin temperature during recovery (P = .042). *
Oxygen Consumption
Figure 3 shows a significant difference in V
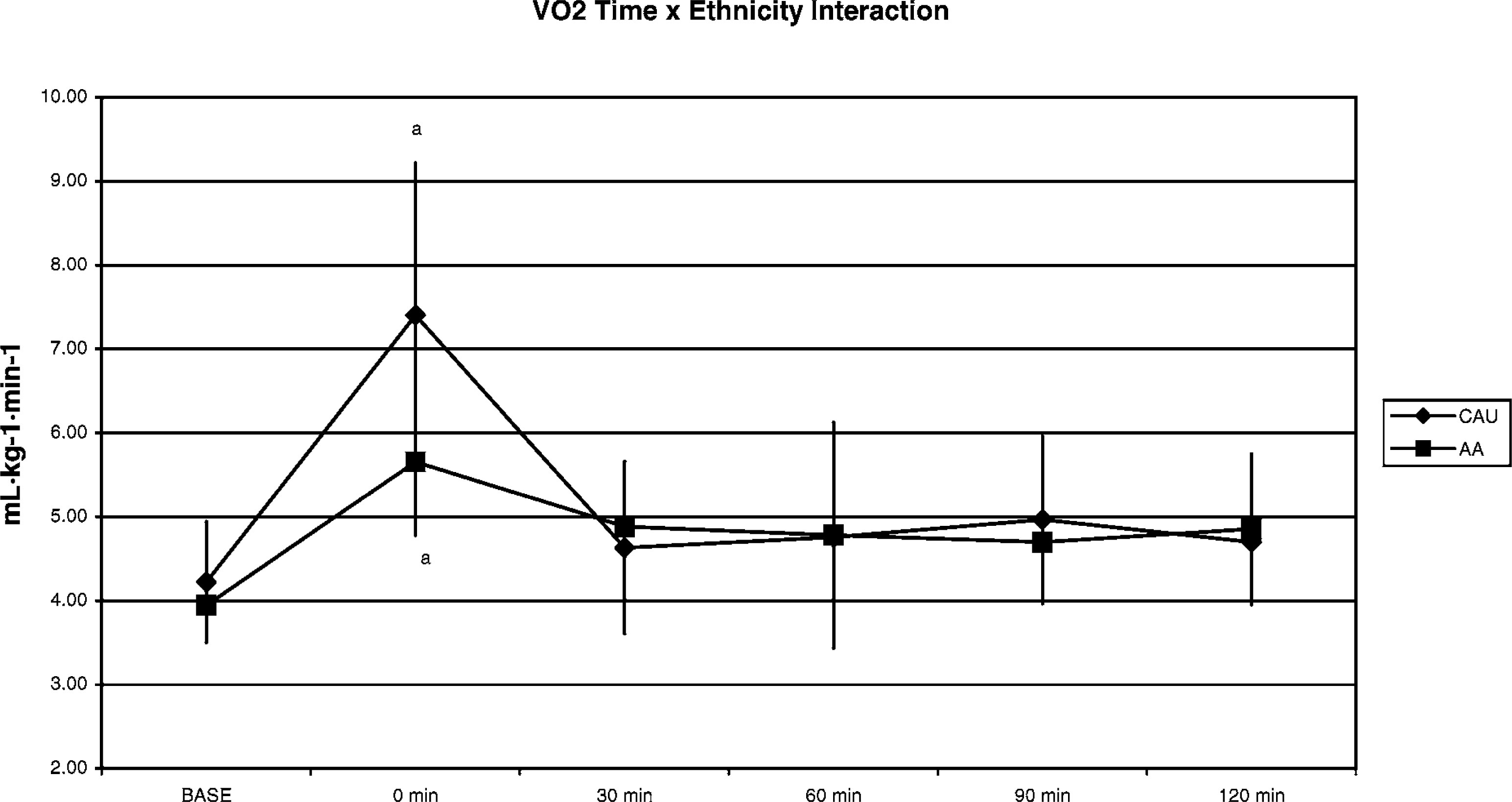
Time × ethnicity interaction for V
Discussion
The present study examined the influence of ethnicity on the thermoregulatory and metabolic responses of AA and CAU males during ACE-REC. When exposed to environmental extremes, the challenge is to maintain thermoregulatory homeostasis. Previous research has suggested that there may be a difference in the intrinsic systems responsible for thermoregulation, which may affect how individuals thermoregulate.13–14,16–18 These may include ethnic cardiovascular differences, such as higher resting blood pressure and increased total peripheral resistance among AA. 11
The response of Tre demonstrated by the participants is consistent with earlier research conducted in the field of environmental physiology.1,4,12 As the physiological stress of ACE-REC increased, Tre decreased over time. The primary physiological stress during recovery is due to the return of cold peripheral blood to the core. This phenomenon is commonly referred to as afterdrop. This response differed significantly between the groups and suggests that AA individuals maintained a significantly lower Tre than their CAU counterparts over time (Figure 1). One may speculate that the AA group may be more at risk for hypothermia.
Additional research in the area of ethnicity may focus on thermoregulation to cold exposure employing a more prolonged recovery period or perhaps a greater cold air stressor. Mean skin temperature demonstrated a main effect for time (Figure 2). This response in mean skin temperature demonstrated by the experimental participants is in agreement with the research in the area of environmental physiology, whereby Tsk (over time) is closely linked to ambient temperature.6,19–22 In addition, there was a significant time × ethnicity interaction (Figure 2), whereby the AA group demonstrated a lower Tsk at 60 and 90 minutes than did the CAU group. This is probably due to the greater heat loss, which was also demonstrated via the lower Tre. In both the Tre and Tsk responses, the initial change and the interaction may be a result of the immediate and initial measurement in the transition from the cold air (10°C) to the warmer ambient air temperature (25°C), which best perhaps represents thermoresponsiveness, or the return of the cold peripheral blood to the core.
Although peripheral vasoconstriction functions to reduce heat loss, an increase in heat production via an increase in oxygen consumption demonstrates an increase in shivering thermogenesis. As recovery from cold exposure time increased, oxygen consumption increased initially with a concomitant decline in Tsk and Tre and then reached a plateau at slightly higher values compared with the baseline.
In a cold environment, the peripheral thermoreceptors are believed to send a signal to the hypothalamus, which then activates the brain centers to increase shivering, among other thermoregulatory responses. These data therefore suggest that external stressors influence homeostasis by altering the involvement of the hypothalamus with both the sympathetic adrenal medulla and the hypothamalmic pituitary axis.
1
The present investigation demonstrated a significant time × ethnicity interaction for Tre and V
The difference in V
However, there was a difference in metabolism between the groups, whereby the CAU participants exhibited higher values then their AA counterparts. The experimental literature suggests morphological, racial differences between AA and CAU individuals. 24 However, the present investigation did not show significance for morphological characteristics. Contrary to the results of the present investigation, Hooton 24 demonstrated that AA individuals have a greater surface area in their extremities and have greater subcutaneous fat located more centrally. Both of these factors may elicit greater heat loss through the periphery and, in part, may account for these differences in thermoregulation.
Adams and Covino observed that after 55 minutes of whole body exposure, CAU and Eskimo participants had increased heat production by 22 cal·hr·m2 above control levels of 40 and 55 cal·hr·m2, respectively, whereas the AA participants, after 85 minutes of exposure, had increased heat production by only 10 cal·hr·m2. 2 Similarly, in the present investigation, the CAU volunteers had an initial increase in energy and a higher Tre compared with their AA counterparts. Further, Adams and Covino observed that after 85 minutes of exposure, the AA participants had not increased heat production to levels equal to that of either of their CAU or Eskimo counterparts. 2 In the present investigation, after the initial increase in energy expenditure, the CAU group had slightly higher energy expenditure in ACE-REC. This may again suggest that the CAU group was more responsive to the stressor through the return of peripheral cooled blood back to the core than their AA counterparts. This may be due to the central (ie, sympathetic adrenal medulla and hypothamalmic pituitary axis) and/or morphological differences that clearly warrant further investigation in the area of ACE.
The data of the current investigation suggest that although Tre differed between the AA and CAU individuals, the CAU individuals appeared to expend more energy to maintain a higher rectal temperature compared with their AA counterparts at the 0 minute time point of ACE-REC. This “hyper” metabolic heat production exhibited by the CAU group may prove to be beneficial in the maintenance of rectal temperature and ultimately temperature homeostasis over a prolonged period during recovery from cold stress. Further, as a result of the higher metabolic rate, the CAU individuals are at reduced risk for the development of hypothermia compared with AA individuals, as demonstrated by the increase in shivering thermogenesis and energy expenditure, which play a role in the maintenance of temperature homeostasis.
Limitations of the present study include the small sample size and the discrepancy between group sizes. Both of these factors resulted from difficulties in recruiting CAU and AA participants for this study. However, the related literature within this field of research often uses small sample sizes, and this limitation may indicate a possible reduced significance and adequate statistical power.
Conclusions
In conclusion, based on these data there was a differential response between CAU and AA individuals over time for V
Footnotes
Funding
This study was funded in part by the Natural Science and Engineering Research Council (Canada).