
Abstract
Objective
Maximum aerobic capacity decreases at high altitude. This study was conducted to compare the changes in maximum aerobic capacity in men and women mountaineering trainees on induction to high altitude at 4350 m by trekking.
Methods
Eight men and 8 women mountaineering trainees in a mountaineering course were selected for the study. The initial study was conducted at 2100 m (586 mm Hg) and then during 6 to 7 days of sojourn at 4350 m (435 mm Hg). Maximum oxygen consumption (V
Results
V
Conclusions
The results indicate that the decrement of maximum aerobic capacity at 4350 m was less in women than in men under similar modes of ascent.
Introduction
Physiologically, an elevation of 2500 m (8250 feet) above sea level is considered high altitude, because at this height arterial oxygen saturation (Sa
Exercise responses of men at varying altitudes have been extensively studied, but not much attention has been given to investigating the exercise response in women. The comparison between men and women at high altitude at rest has indicated some differences in physiological parameters. Cudkowicz et al 4 showed an increase in the forced expiratory volume in 1 second of female sojourners at 5200 m, whereas in males it remained unchanged. Women living at low altitude have greater ventilation relative to carbon dioxide production, that is, lower end tidal partial pressure carbon dioxide, compared with men.4,5 This greater alveolar ventilation in women compared with men at sea level suggests that women may be predisposed to a more rapid ventilatory acclimatization response at high altitude. A few studies on women's responses to maximal exercise under hypobaric hypoxic conditions reported varying results. 6 –8 Our earlier study on submaximal work performance in women mountaineers at 2100 m and 4350 m altitudes indicated that native women of moderate altitudes were more fit than their sea level counterparts and that induction to high altitude by trekking under progressive hypoxia coupled with rigorous mountaineering activity provides better acclimatization and improved physical work performance. 9 However, the effect of altitude on maximal exercise responses in men and women mountaineering training under similar regimens of ascent by trekking has not been studied. The present study sought to investigate the rate of changes of maximum exercise responses in men and women at 4350 m altitude while undergoing mountaineering training under similar regimens.
Materials and methods
Eight men and 8 women trainees were randomly selected for this study from a total of 50 trainees who came to Himalayan Mountaineering Institute (HMI), Darjeeling (2100 m), India, for a basic mountaineering course. All of them were medically fit. None of the participants had been to high altitudes within the previous 3 months. The participants gave their informed consent and were aware of their rights to withdraw from the experiments at any time. The Ethics Committee of the institute approved the experimental protocol.
Initial pretraining measurements of maximum exercise test were carried out in the medical investigation room at HMI (Darjeeling) with a room temperature of 16 °C to 20 °C. The same investigations were repeated on induction to high altitude at Chaurikhang, the base camp of HMI (4350 m), within a makeshift laboratory inside the Silver Hut, where the room temperature was maintained between 17 °C and 20 °C, with the help of bukharies (gas or kerosene heaters). This Silver Hut was used by a scientific and mountaineering expedition team in 1960 and 1961 led by Sir Edmound Hillary on Ama Dablam glacier at an altitude of 5800 m, about 15 km south of Mount Everest. Presently, it is under the management of HMI (Darjeeling) at Chaurikhang in the eastern Himalayas, the base camp of HMI. The study was conducted in 2 phases: 1) a baseline study was carried out during the first 3 days of stay at HMI (2100 m, barometric pressure 586 mm Hg), and 2) a high altitude study was conducted on days 6 and 7 at 4350 m (barometric pressure 435 mm Hg) in the Silver Hut. All the tests were conducted by the same group of observers with the same set of equipment in both sites.
At HMI (Darjeeling), the trainees underwent a rigorous training schedule of mountaineering activities [1 week] from early morning until late evening with intermittent breaks. After a week's training at Darjeeling, they set out on their journey to the base camp (4350 m elevation). The trainees were transported (160 km) by bus (day 8) from Darjeeling to Yoksom (2200 m elevation). On the next morning (day 9), all the trainees trekked for about 15 km and reached Bhakim (2750 m), where they stayed for the next day (day 10). On day 11, the participants walked to Zamlingaon (3600 m elevation) after crossing over a height of 4500 m, covering a distance of 12 km, and halted there for the next day (day 12) for acclimatization. On day 13, the trainees trekked about 14 km and reached the base camp of HMI at Chowrikhang (4350 m). The trainees trekked about 2 to 3 km/h for 5 to 6 hours each day at increasing altitude under progressive hypoxia while carrying a load of approximately 15 kg.
During days 14 to 23 (10 days), participants stayed at 4350 m in a hut made of metal sheets and fitted with bunks. They used appropriate winter clothing. They undertook intense mountaineering training that involved glacier marching, ice cutting, peak assault, back packing, repelling, and rock climbing and were engaged in snowbound field areas at higher elevations in the forenoon and nearby camp areas in the afternoon. On the penultimate day of training, they climbed a peak of about 5550 m.
The maximum and minimum ambient temperatures at the base camp during the period of study were +10 °C and −7 °C, respectively. Sunshine and partial cloudiness during the day with occasional snowfall and high-velocity wind are the characteristic features of the area. At high altitude, none of the participants exhibited any symptoms of discomfort or acute altitude sickness, and they were not taking any medication. A clinical assessment was made by a trained physician from HMI during the morning assembly every day. The trainees were free to report their ailments/discomfort and/or injuries without any fear. All of them ate well, slept well, and worked as demanded in the course syllabus. After 10 days of sojourn at 4350 m, they returned to HMI (2100 m), which involved 2 days of trekking (days 24 and 25) and a motor journey of 1 day (day 26).
Participants were allowed to sit comfortably for 10 minutes before the start of the experiment in the laboratory at both 2100 m and 4350 m. Exercise tests were performed on a calibrated cycle ergometer with a pedal rate of 60 rpm. Participants were lightly dressed and wore appropriate shoes. The room temperature was between 18 °C and 20 °C, and relative humidity was 50% to 60%.
The exercise protocol was a modification of that described by Wasserman et al.
10
After a resting period of 3 minutes on the bicycle, the participants exercised at zero workload for 3 minutes until the heart rate and respiratory values reached a steady state. At the end of the zero-load pedaling period, the work intensity was increased, starting at 30 watts followed by an incremental increase of 15 watts every minute until volitional fatigue occurred. When the heart rate was about 170 beats·min−1, participants were encouraged to continue the test until exhaustion. The volunteer breathed through a low-resistance respiratory valve and breathing circuit connected to a computer-controlled, breath-by-breath metabolic measurement system (Benchmark Exercise Test System and Nutrition monitor, PK Morgan, Kent, UK). Minute ventilation (VE) and oxygen consumption (V
Statistical analysis of the data was performed by 2-way classification of an analysis of variance technique using the Newman-Keuls multiple range test to compare the same group at different situations. An unpaired t test was used for the comparison of men and women for each situation. A 5% level of significance was considered the critical level.
Results
The mean and SEM values of age and height were 20.6 ± 1.02 years and 154.0 ± 1.32 cm for females and 22.38 ± 0.32 years and 154.50 ± 0.89 cm for males, respectively. Body surface area was similar in both the groups. The body weights were 47.25 ± 1.70 kg for females and 59.1 ± 2.79 kg for males. Mean ± SEM values of cardiorespiratory variables during maximal exercise at 2100 m and at 4350 m in men and women and their comparisons are presented in the Table. Total work time and maximal power output were less in women than men at both altitudes. At 2100 m men showed maximum work output of 181 watts compared with women, who reached only 115 watts. Total working time was 10.1 minutes in men and 5.7 minutes in women. On ascent to high altitude (4350 m), both men and women showed significant decrement of maximum work capacity, as well as working time. At 4350 m altitude, maximum power output for men was 156 watts and for women 102 watts, and total work times were 8.4 and 4.8 minutes, respectively.
Physiological responses to maximal exercise in men and women at different altitudes*
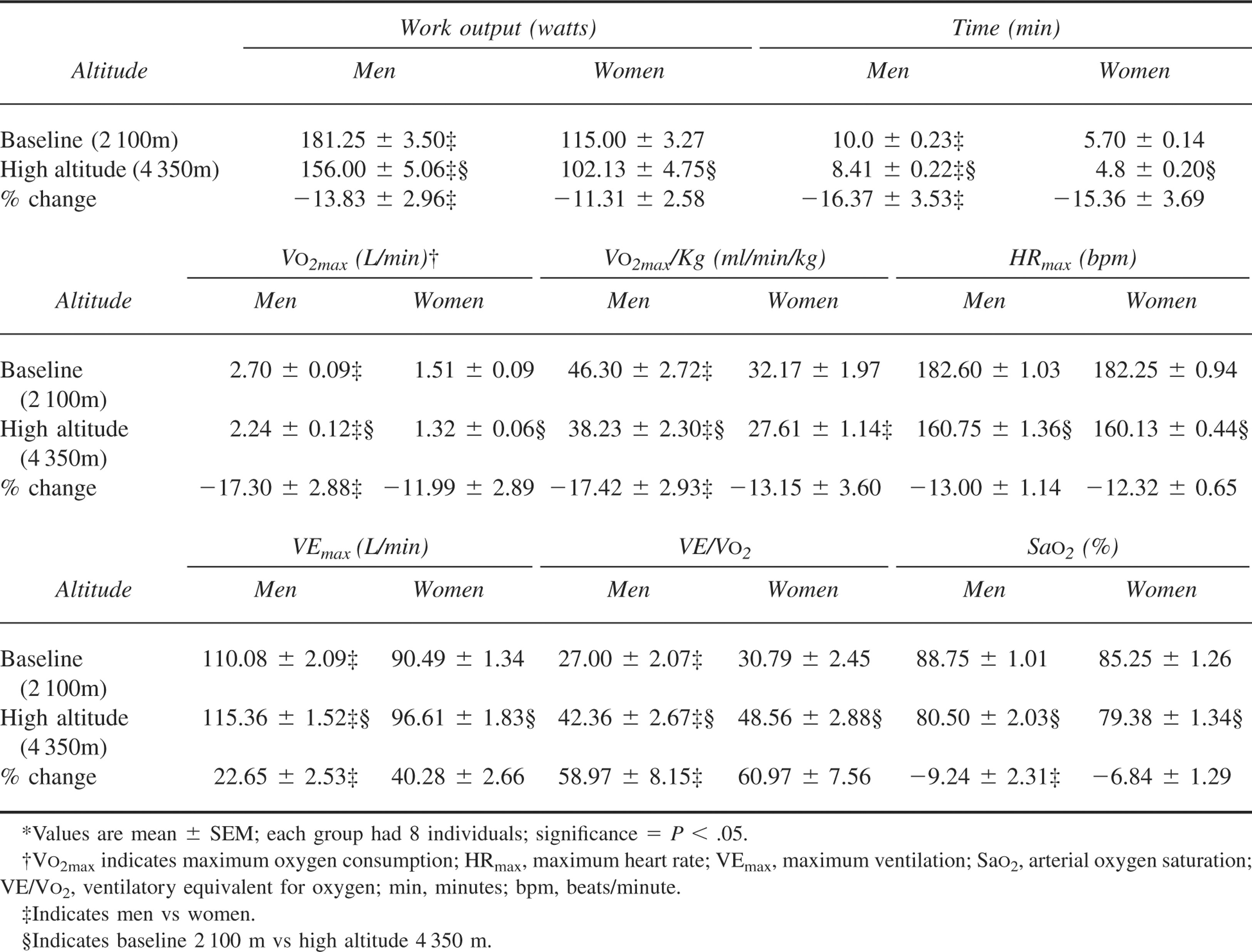
Maximum oxygen consumption (V
Discussion
Reports of gender variance on hypoxic tolerance
11
–13 and maximum exercise responses at high altitude are limited. A recent review by Jean et al
14
discussed women (both nonpregnant and pregnant) going to high altitudes for brief periods. The present study evaluated the decrement of maximum exercise responses of men and women at 4350 m altitude while undergoing mountaineering training that was similar to ascending by trekking. We found a significant reduction in V
In this study the minimal effect we found of altitude on maximal work performance in men and women mountaineering trainees may be due to their gradual ascent by trekking, as well as their participation in such mountaineering activities as heavy lifting, rock climbing, peak assault, and glacier marching. The participants of the present study appeared properly acclimatized on the day they reached 4350 m altitude. None of them showed any indications of acute altitude sickness, and they all ate and slept well during their stay at 4350 m, indicating a proper level of acclimatization. The limitation of our study is that we could not measure spirometry and hemoglobin levels due to unfavorable circumstances. A spirometry test given just before exercise would have enabled a better comparison in men and women participants with regard to evaluating ventilatory responses. The measurement of hemoglobin levels could have given a more distinct difference in aerobic capacity, because hemoglobin levels are 11% to 14% lower in women than men, 24 which further limits oxygen delivery and uptake capacity.
With respect to ventilatory response, the increase in VE/V
With acute altitude exposure, there is a reduction in arterial oxygen content.
28
However, with sustained exposure for a few days at high altitude, arterial oxygen content is restored to near sea level values due to hemoconcentration and an increase in Sa
In conclusion, our results indicated that there was a significant decrement of V
Footnotes
Acknowledgments
We are grateful to the Principal Himalayan Mountaineering Institute, Col Vijay Singh, Medical Officer HMI, Major A. Chakravorty and staff of HMI, Darjeeling, for providing logistic support for the study. Warm thanks are due to all the trainees of the Basic Mountaineering course who volunteered as participants for their whole-hearted cooperation. We thank the Field Director, as well as all the instructors of HMI for their help during the study. Acknowledgment is due to Dr S. S. Verma, Sc ‘F,’ Dr Y. K. Sharma, Sc ‘D,’ and Mrs Shikha Anand for statistical analysis of the data. We are thankful to Dr U.S. Ray, Sc ‘E,’ Divisional Head, Environmental Physiology Division, and Dr G. Ilavazhagan, Sc ‘G,’ Director of Defence Institute of Physiology and Allied Sciences.