
Abstract
Objective
Although hypothermia is preventable, little has been published on its epidemiology. This study estimates the incidence of hypothermia and other cold-related morbidity emergency department (ED) visits in the United States.
Methods
We identified hypothermia and other cold-related morbidity ED visits from the 1995–2004 National Hospital Ambulatory Medical Care Surveys using the International Classification of Diseases, Ninth Revision (991.6–991.9) or cause-of-injury E-codes (901.0–901.9 and 988.3).
Results
In the United States there were an estimated 15 574 (95% CI = 9 103–22 045) hypothermia and other cold-related morbidity ED visits during 1995 to 2004. Compared with other ED patients, those with hypothermia and other cold-related morbidity diagnoses were older (mean age 45 vs 36 years; P = .009) and were more likely to be uninsured (risk ratio [RR] = 2.44; 95% CI = 1.54–3.84). Hypothermia and other cold-related morbidity ED visits required more transfers to critical care units (RR = 6.73; 95% CI = 1.8–25.0) than did other ED visits.
Conclusions
Hypothermia and other cold-related morbidity is a preventable resource-intensive condition that tends to affect the disadvantaged.
Introduction
Hypothermia is a preventable cause of morbidity and mortality in the United States. 1 People exposed to cold temperatures may be unable to generate enough heat (eg, through shivering) to maintain a normal core body temperature of 37°C ± 1°C (98°F). Hypothermia occurs when the core body temperature drops below 35°C (95°F) and cardiac, renal, or central nervous system dysfunction develops.2,3 Central nervous system depression caused by excessive exposure to cold temperatures can impair a person's ability to seek shelter, thus leading to further drop in core body temperature. Hypothermia can be potentially fatal as a result of central nervous system depression and dysrhythmias. 4 During 1999 to 2002, an estimated 4607 people in the United States died from hypothermia-related conditions (annual incidence = 4/1 000 000). 1 Advanced age (ie, >65 years), male sex, living in cool or cold homes, wearing too little or inappropriate clothing, and using mood- and cognition-altering drugs were among the risk factors associated with hypothermia-related death.5,6 The most frequent causes of death associated with hypothermia were falls, drownings, and atherosclerotic cardiovascular disease.
Although much has been published about hypothermia mortality, little has been published on the incidence and risk factors associated with hypothermia morbidity.1,6 This information is needed to develop public health strategies and interventions for cold-related morbidity and mortality. Information on the annual incidence of hypothermia morbidity in the United States is currently unavailable. Based on international literature, the incidence of nonlethal hypothermia is likely to be much greater than hypothermia mortality. 7 The objective of this study was to use National Hospital Ambulatory Medical Care Survey (NHAMCS) data to estimate the incidence and identify the risk factors of hypothermia and other cold-related morbidity evaluated at emergency departments (EDs) in the United States. The intent of our study is to help guide public health strategies aimed at preventing hypothermia and other cold-related morbidity through community interventions.
Methods
The National Hospital Ambulatory Medical Care Survey is a nationally representative probability sample of visits to randomly selected general and short-stay hospitals (excluding federal, military, and Veterans Affairs Hospitals) in the United States (U.S.). 8 The survey is directed by the National Center for Health Statistics at the Centers for Disease Control and Prevention. The survey uses a 4-stage probability sampling of geographically defined areas, hospitals within these areas, EDs within these hospitals, and patient visits within these EDs. 9 Visits sampled occurred during randomly selected 4-week reporting periods that were representative of all 12 months of the year. The survey data include demographics, reason for visit, diagnostic testing information, external cause-of-injury E-code, 3 physician International Classification of Disease, ninth edition (ICD-9-CM) diagnoses, medication therapy, and disposition for each ED visit.
We defined hypothermia and other cold-related morbidity ED visits as visits with the following ICD-9-CM codes and E-codes: 991.6 (hypothermia); 991.8 (other specified effects of reduced temperature); 991.9 (unspecified effect of reduced temperature); E901.0 (excessive cold due to weather conditions); 901.8 (excessive cold other specified origin); E901.9 (excessive cold of unspecified origin); E988.3 (injury by other extremes of cold). We did not include codes for localized cold-related morbidity in our analyses (eg, 991.0 [frostbite of face]; 991.1 [frostbite of hand]; 991.2 [frostbite of foot]; 991.3 [frostbite of other and unspecified sites]; 991.4 [immersion foot]; 991.5 [chilblains]) because patients with these conditions are treated differently than those with hypothermia. Hypothermia diagnoses related to surgery, birth, or exposures to refrigerated environments were also excluded from our analyses because we wanted to focus the study on hypothermia that results from naturally occurring cold environments. Effective public health interventions may reduce the number of people who are affected by this type of hypothermia.
Because hypothermia has a low prevalence, we combined NHAMCS data from 1995 to 2004 to obtain national estimates of hypothermia and other cold-related morbidity ED visits. We estimated the number of these ED visits throughout the United States by applying the appropriate NHAMCS sampling weights. The chi-square statistic was used to test for differences in proportions of the variables of interest between hypothermia and cold-related morbidity and other ED visits. The incidence of hypothermia and other cold-related morbidity ED visits was calculated using the U.S. Census 2000 population estimates. 10 Analysis was conducted using SAS 9.1 (SAS Institute, Cary, NC).
Results
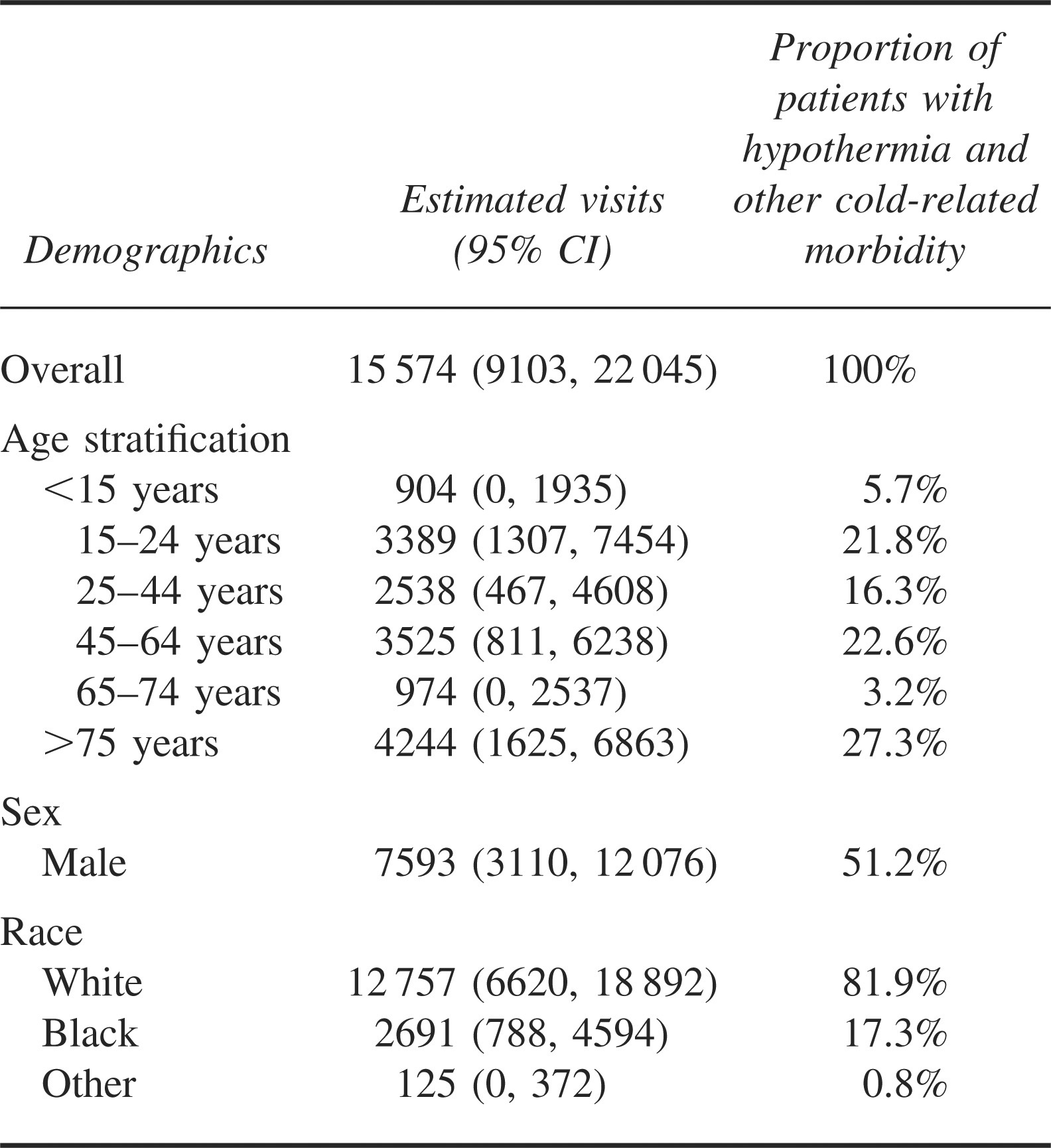
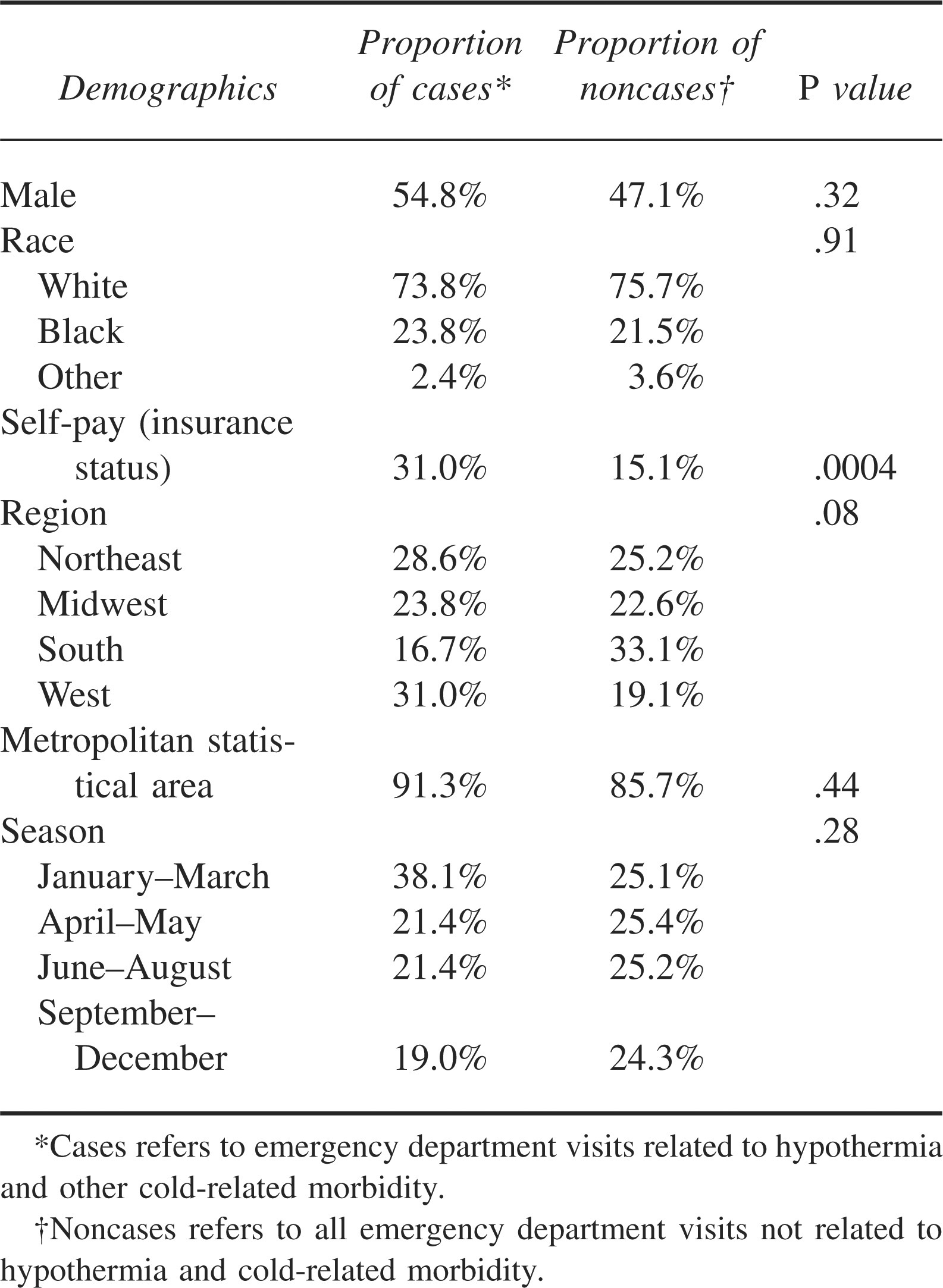
From the 42 hypothermia and other cold-related morbidity visits recorded in NHAMCS, we estimated that there were 15 574 (95% CI = 9103–22 045) hypothermia-related ED visits during 1995 to 2004. Hypothermia and other cold-related morbidity visits were 0.01% of a total annual 105 million (95% CI = 97 million–114 million) ED visits in the United States during this period (annual incidence of 5.6 per 1 000 000 persons) (Table 1). These visits occurred throughout the year and peaked during February (Figure 1). Hypothermia and cold-related morbidity case patients were older than other patients (mean age 45 vs 36 years, respectively; difference = 9.4; 95% CI = 2.4–16.5) (Table 1). Fifty-five percent of case patients with hypothermia and other cold-related morbidity conditions were male (Table 2). The number of hypothermia and other cold-related morbidity visits was insufficient to produce reliable stratified population estimates for age, race, ethnicity, and alcohol use.
Visits to United States emergency department for hypothermia and other cold-related morbidity, 1995–2004
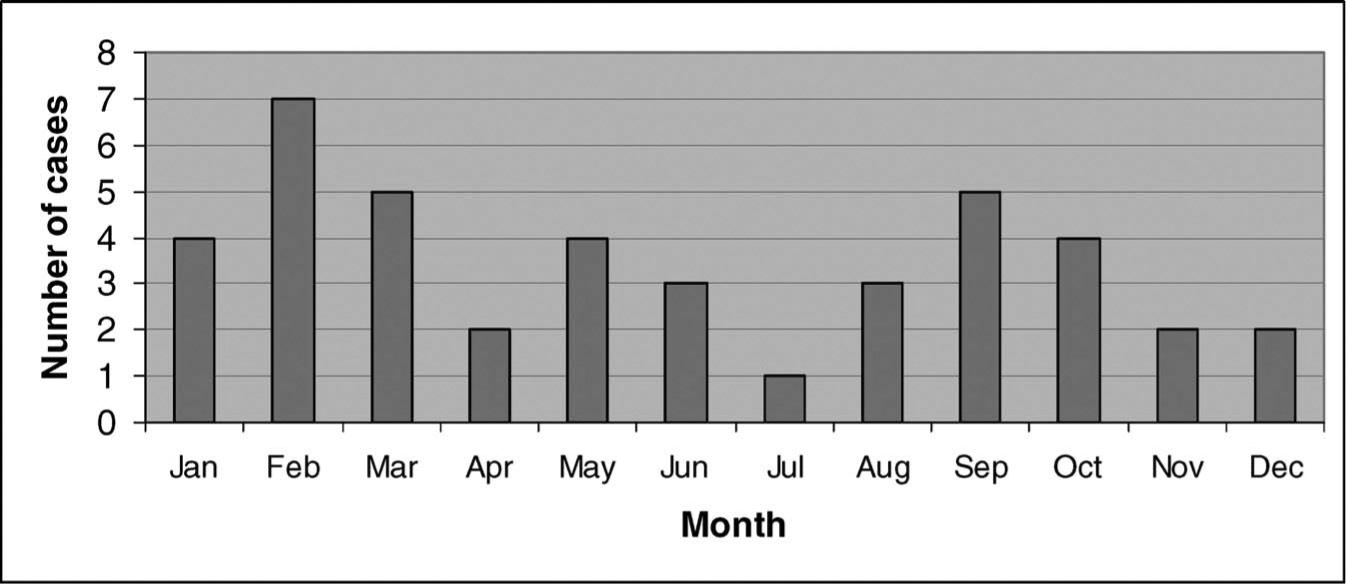
Absolute frequency of hypothermia and other cold-related morbidity emergency department visits recorded in National Hospital Ambulatory Medical Care Survey by month from 1995 to 2004.
Comparison of hypothermia and other cold-related morbidity visits to United States emergency departments with nonhypothermia visits, 1995–2004
The most frequent reasons for hypothermia and other cold-related morbidity ED visits were adverse effects of the environment (27%); endocrine, nutritional, or metabolic disorders (9%); foot and toe symptoms (9%); altered state of consciousness (7%); adverse effects of drug abuse (6%); alcohol-related problems (6%); and general weakness (6%). The cause of injury was specified for 38 of the 42 case patients. The most frequent causes of injury were excessive cold (82%), fall (5%), alcohol use (5%), poisoning (5%), and accidents with watercraft that caused submersion in cold water (3%). The most frequent primary diagnoses of hypothermia and other cold-related morbidity ED visits were effects of reduced temperature (ICD9 code 991, 66%), nondependent abuse of drugs (ICD9 code 305, 9%), and disorders of the pancreas (ICD9 code 251, 9%). Thirty (71%) of the 42 case patients diagnosed with hypothermia and other cold-related morbidity diagnoses had an initial temperature of <35°C (<95°F) measured in the ED. Only 1 (2%) of the 42 case patients identified died in the ED.
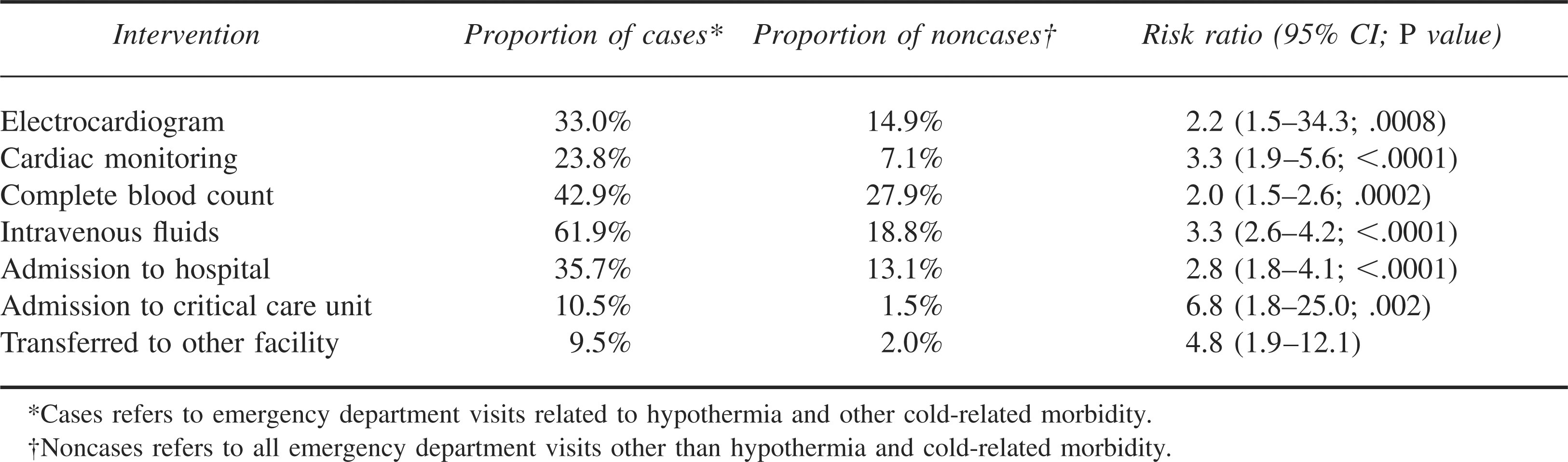
Hypothermia and cold-related morbidity visits were more resource intensive than other visits (Table 3). Patients with hypothermia and cold-related morbidity were more likely to receive electrocardiograms (RR = 2.2; 95% CI = 1.5–3.4), cardiac monitoring (RR = 3.3; 95% CI = 1.9–5.6), or intravenous fluids (RR = 3.3; 95% CI = 2.6–4.2) than other patients. Patients with hypothermia and cold-related morbidity patients were also more likely to be admitted to the hospital wards and the critical care units or to require transfer to different hospitals.
Care patients received during hypothermia and other cold-related morbidity visits to United States emergency departments, 1995–2004
Discussion
This study has 3 predominant findings. First, the annual incidence of hypothermia and other cold-related morbidity is higher than the incidence estimated based on the annual incidence of cold-related mortality. 1 Second, the demographics of hypothermia and other cold-related morbidity ED patients are similar to what is reported in the literature. 6 Third, hypothermia and other cold-related morbidity ED visits are resource intensive.
The predominant focus of hypothermia research and literature has been on mortality. Our findings suggest that relying on mortality data alone is likely to underestimate the annual incidence of hypothermia and other cold-related morbidity. 11 Furthermore, because NHAMCS is limited to ED visits, it is likely that the annual incidence of hypothermia-related illness in the United States is higher than we estimated because people may also seek clinical care at other locations.
In our study, the demographics of patients who visited the ED with hypothermia and other cold-related morbidity, specifically the findings that patients tend to be older and male, are similar to reports from mortality databases. 1 Although U.S. Army data suggest that males and females are equally susceptible to excessive exposure to cold temperatures, most people who die from hypothermia are male.1,12 Socially isolated elderly people with chronic medical conditions are at increased risk for developing hypothermia. 13 Both hypothermia-related deaths and hypothermia-related ED visits occur throughout the year, suggesting a need for prevention efforts throughout the year. 1
We have focused on hypothermia and other cold-related morbidity because these conditions are potentially lethal but preventable. People can decrease their risk of developing hypothermia and other cold-related morbidity by wearing a hat, hand coverings, and clothing that creates a static layer of warm air, provides a barrier against the wind, and keeps the body dry; by avoiding alcohol and other mood-altering drugs; and by learning to recognize the signs and symptoms of hypothermia (eg, shivering, slurred speech, and somnolence) that indicate the need to seek shelter and call for help.
Limitations
This study has a few limitations. The small number of individuals identified from the database limits our ability to extrapolate reliable national estimates, particularly with regard to subgroups of interest (eg, sex, race). There is also no way to determine the accuracy of ICD-9 coding.
Conclusions
Analysis of NHAMCS data suggests that hypothermia and other cold-related morbidity, which are preventable conditions, are an environmental health concern that warrants public health attention. To reduce the incidence of hypothermia in the community, future research should focus on identifying modifiable risk factors and developing and implementing strategies tailored to address the needs of vulnerable populations.
Footnotes
Acknowledgment
This work was supported by the Centers for Disease Control and Prevention.
*
The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention and the Agency for Toxic Substances and Disease Registry.