
Abstract
Objective
Acute hypoxia causes vasoconstriction in the pulmonary arteries. This hypoxic pulmonary vasoconstriction (HPV) has been reported to be common in subjects exposed to high altitude. In the past, it has been difficult to directly measure this HPV because of the invasive nature of tests, but the recent availability of portable color flow Doppler ultrasound has enabled measurements of pulmonary artery systolic pressure (PASP) in the field. We set out to study the feasibility of this method to detect changes related to HPV at 4250 m. We hypothesized that significant changes in the cardiopulmonary circulation are seen at high altitude and are detectable with Doppler echocardiography. In addition, we hypothesized that detected changes are related to the syndrome of acute mountain sickness (AMS) and could be reversed using 100% oxygen.
Methods
Over a 10-week period in the spring of 1998, 56 healthy lowlanders not normally residing at altitude were studied while visiting 4250 m in Nepal having walked from 2774 m. This was a cross-sectional observational study conducted by a single experienced observer at high altitude, using transthoracic color flow continuous wave Doppler echocardiography. Subjects were initially assessed for significant tricuspid regurgitation (TR) to measure PASP. After estimating PASP under ambient conditions at altitude, oxygen was delivered and PASP remeasured.
Results
Of 56 subjects, 36 had Doppler signals appropriate for estimation of pulmonary artery systolic pressure. In these 36, a wide range of PASP was observed (mean 25 mm Hg, range 18–36 mm Hg), but none fell outside of the normal range. After oxygen administration, PASP was reduced (from mean 25 mm Hg to mean 18 mm Hg, P < .0001) suggesting that a degree of hypoxic pulmonary vasoconstriction was present. No subjects in the study group reported clinical AMS.
Conclusions
We found PASP at 4250 m to be within the normal range but higher than would be expected at sea level; however, unlike previous reports, we found such increases to be mild and reversible with oxygen. In addition, the observed incidence of AMS was low when compared with earlier studies, perhaps related to adequate acclimatization.
Keywords
Introduction
Hypoxia associated with high altitude causes changes in cardiopulmonary function. The advent of portable echocardiography has enabled us to evaluate these functional changes in very remote locations. We hypothesized that changes in the cardiopulmonary circulation associated with the hypoxia of high altitude would be detectable with Doppler echocardiography and could be reversed using 100% oxygen. In addition, we hypothesized that these hypoxic changes would be related to the syndrome of acute mountain sickness (AMS).
It has been known since 1946 that alveolar hypoxia causes vasoconstriction of pulmonary arteries. 1 –5 Many previous studies have relied on invasive measures of right ventricular pressure requiring a right heart catheter to establish the extent of hypoxic pulmonary vasoconstriction (HPV), and this has limited the use of other methods in the field as they are mostly invasive. However, Doppler echocardiography offers a noninvasive measure of pulmonary artery systolic pressure (PASP) based on a calculation using tricuspid regurgitant (TR) jet velocity detected in upwards of 70% of otherwise normal individuals. 5 This pressure gradient between the right atrium and the right ventricle (RA-RV) measured from the TR jet velocity has been used to estimate pulmonary artery systolic pressure 5 –8 and vascular responses in normobaric hypoxia at sea level4,7,9 as well as hypobaric hypoxia at altitude1,10,11 and in a hypobaric chamber. 12
Hypoxic pulmonary vasoconstriction has been implicated in the pathophysiology of high altitude pulmonary edema (HAPE),2,4,13,14 but not in the more common syndrome of AMS.2,10,13,15–19 High altitude pulmonary edema, unlike AMS, which is self limiting, has a mortality of 44% when untreated. 20 We hypothesized that changes in HPV may be associated with AMS, as in this setting even mild hypoxic pulmonary vasoconstriction may exacerbate hypoxemia, which is a key feature in the development of AMS. 21
Methods
Setting
The study took place at the Himalayan Rescue Association (HRA) aid post, located in the settlement of Pheriche in the Solo Khumbu region of Nepal, at an altitude of 4250 m, close to Mount Everest Base Camp (Figure 1).

Himalayan Rescue Association clinic, Pheriche, Nepal, 4250 m.
Subjects
Over a 10-week period in the spring of 1998, 56 subjects, all healthy lowlanders not normally resident at altitude, were studied while visiting the Himalayan Rescue Association aid post (for educational lectures). Prior to reaching the study location at 4250 m these subjects had acclimatized by walking from 2774 m. Exclusion criteria included age greater than 70 years, intercurrent illnesses, and predisposing cardiac conditions as documented by history. The protocol was approved by the University of Glasgow Regional Ethics Committee and all subjects gave informed consent.
Study Design
This was a cross-sectional observational study conducted by a single experienced observer at high altitude, using transthoracic color flow continuous wave Doppler echocardiography (Challenge Doppler Colour Cardiac Ultrasound powered by a photovoltaic array, Imotek/ Esaote Biomedica, Huntington, UK). Subjects were initially assessed for significant TR to measure PASP. After estimating PASP under ambient conditions at altitude, oxygen was delivered and PASP remeasured. In addition, oxygen saturation and heart rate measurements, as well as medical and ascent profile trekking history, were recorded. Acute mountain sickness was assessed using the Lake Louise questionnaire. 21
Study Protocol and Measurements
Subjects were examined in the semireclining position by a single, experienced observer using a transthoracic 2.5 MHz ultrasound probe applied to the chest wall (Figure 2). Those subjects found to have measurable tricuspid regurgitant jets, as defined by a peak velocity (Vmax) greater than 1.5 ms−1, were assessed for right artrial–right ventricular pressure gradient by measuring the velocity of the tricuspid jet before and after oxygen intervention. Mean Vmax was calculated by averaging the values of the 5 highest measured TR jet velocities (Figure 3). The RA-RV pressure gradient was calculated using the modified Bernoulli equation. 5 Subjects with evidence of right ventricular dysfunction from history or echo images were excluded, right atrial pressure (RAP) was not formally assessed, and a universal value of 5 mm Hg was used in the calculation of estimated pulmonary artery systolic pressure. Oxygen was delivered via a non-rebreathing mask at 2 to 4 L/min until the oxygen saturation stabilized at 98% or greater for more than 5 minutes and PASP was remeasured. Subjects were also continuously assessed for changes in PASP during oxygen therapy (as permitted by solar-power availability). Transcutaneous finger pulse oximetry (SpO2) was continuously monitored using a pulse oximeter (Nellcor Puritan Bennett/Mallinckrodt Inc, St Louis, MO).
Subject being examined at Himalayan Rescue Association clinic, Pheriche, Nepal, 4250 m.
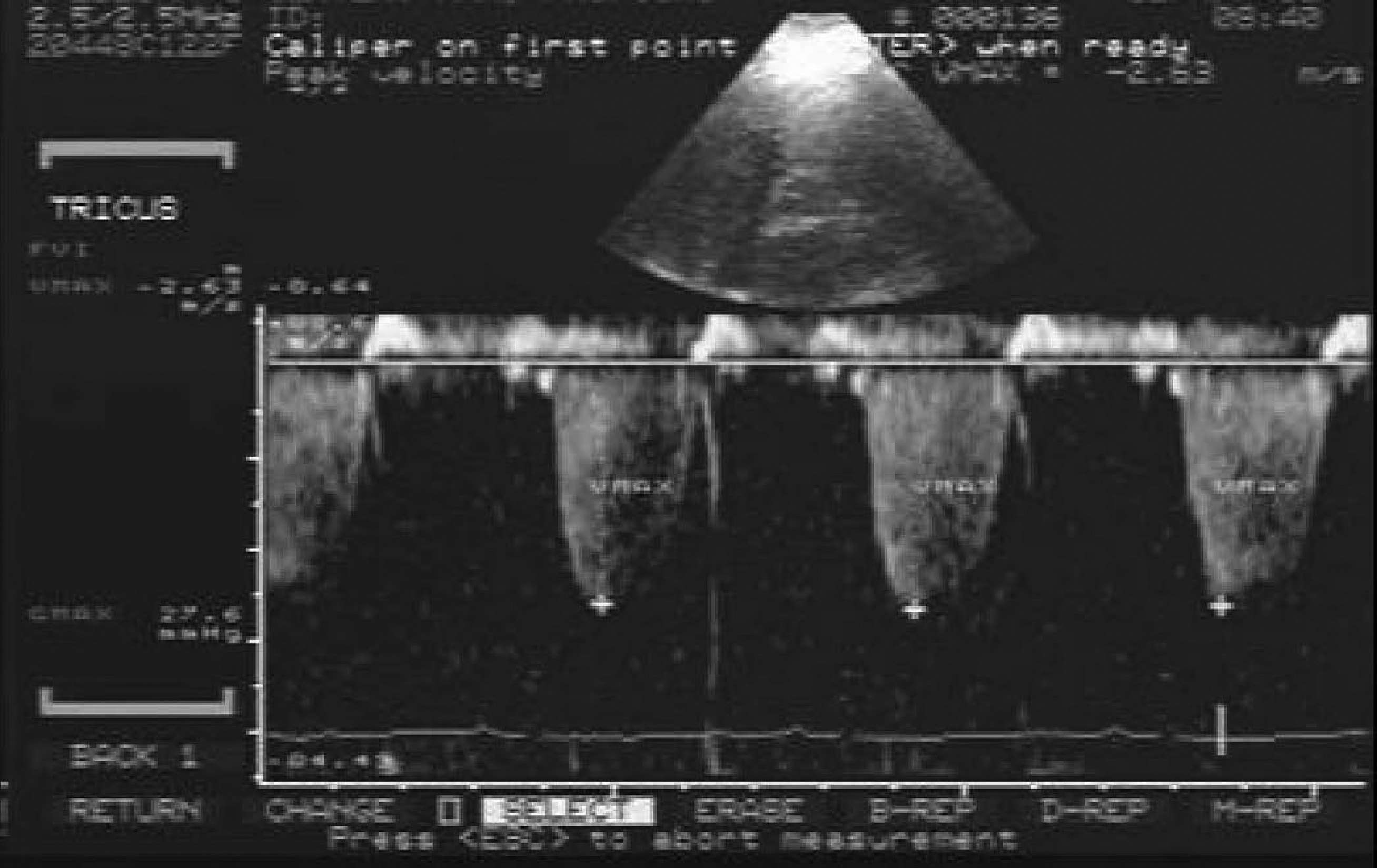
Typical tracing of tricupid regurgitant jet as seen using echo Doppler from a subject at 4250 m, before intervention with oxygen.
Pulmonary artery pressure calculations were compared for differences between PASP under ambient conditions at 4250 m and while subjects breathed oxygen. The effect of acclimatization on PASP was determined by comparing the PASP of those individuals ascending for the first time with those who had been higher in the previous 2 weeks.
Symptoms of AMS were assessed by completion of the self-reporting questionnaire-based Lake Louise score. 22
Data Analysis
PASP variation before and after oxygen and its relationship to AMS were compared by regression analysis. Mean values were compared by a Student's t test. A multivariate analysis was then used to compare the categorical subgroups of males, females, and ascending or descending subjects with the continuous variables including saturation, AMS score and PASP. Data are reported as mean, SD, and/or range in the test as well as 95% CI; statistical significance was defined as P < .05. (Statistics Package for Social Sciences, SPSS, JMP for Mac, SAS Institute, Cary, NC).
Results
Tricuspid Regurgitation
Subjects had spent a mean of 8 days (range 5–16 days) above 2774 m (range 4250–5545 m). In total, 56 subjects were observed (45 male and 11 female), age range 23 to 68 years. Of 56 subjects examined, 36 (30 males, 6 females) had significant (Vmax > 1.5 ms−1) TR flow at 4250 m. The remaining 20 subjects, who did not show significant TR, were not significantly different from the study population (with respect to age, gender, AMS, or previous medical problems). This prevalence is comparable with previous observations of the presence of TR in otherwise normal individuals at sea level. 5
Pulmonary Artery Systolic Pressure
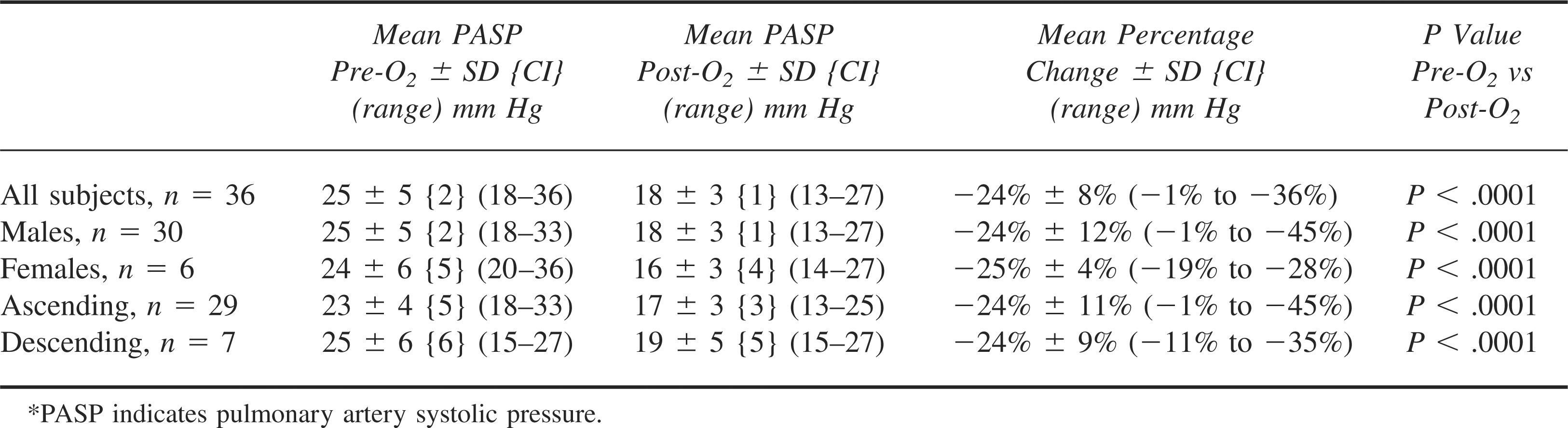
While breathing air at 4250 m, mean Vmax was 2.17 ± 0.28 ms−1 and calculated PASP was 25 ± 5 mm Hg (range, 18–36 mm Hg). After intervention with oxygen, mean Vmax was significantly reduced to 1.80 ± 0.24 ms−1 (P < .05) and mean PASP after 02 was 18 ± 3 mm Hg (range = 13–27 mm Hg; P < .0001; T = 10.34; DF = 35) (Table 1 and Figure 4). In the subjects who were continuously assessed during oxygen therapy, the PASP was seen to stabilize synchronously with the saturation (within 15 minutes).
Pulmonary artery systolic pressure at 4250 m before and after intervention with oxygen*
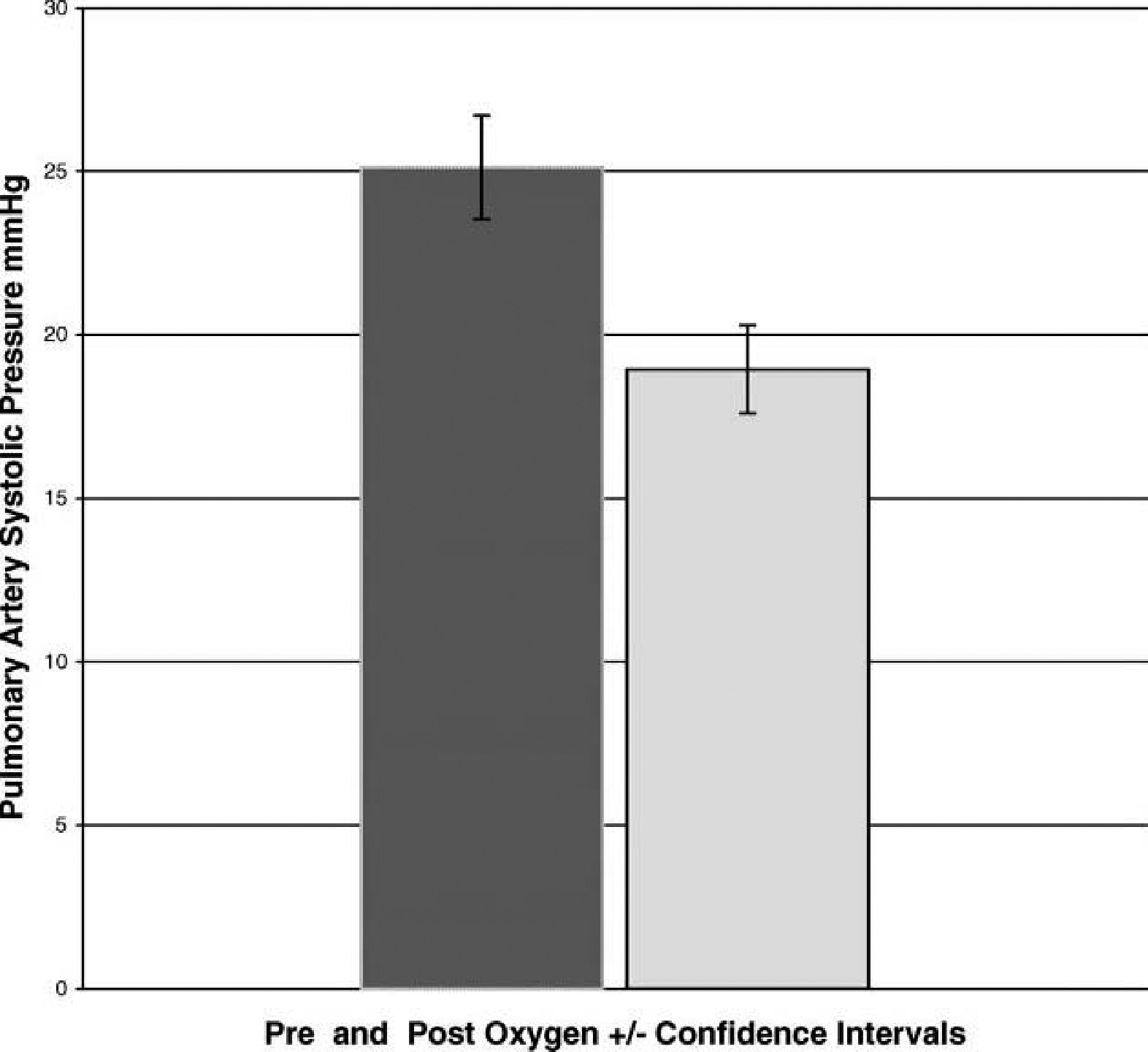
Mean pulmonary artery systolic pressure before and after oxygen intervention at 4250 m.
A multivariate analysis showed that there was no difference between values of PASP in male and female subgroups and no difference compared with individuals who had arrived at 4250 m (after 5–10 days of trekking) for the first time and those who had already ascended higher and were descending through 4250 m (F = 1, P > .05) in spite of the fact that the descending subjects had spent up to 10 days longer at altitude.
Pulse Oximetry
The mean SpO2 was 87% ± 5% (range 62%–93%). Analysis of the saturation data revealed there was no correlation between oxygen saturation and PASP before intervention with oxygen (F = 0.1, P > .05).
Acute Mountain Sickness
Acute mountain sickness was not found in any subjects, as defined by the Lake Louise score of headache plus one symptom (in spite of some symptoms scoring greater than 2), therefore no relationship to PASP could be established (P > .05). The mean AMS score was 1 ± 1.7 (range 0–8), and in spite of a high score, some of these individuals did not exhibit a headache, therefore they did not meet the criteria for AMS.
As there was no AMS (using the Lake Louise criteria), we could not determine the relationship between PASP and AMS. However, using raw Lake Louise scores, a regression analysis showed that there was no correlation between the AMS scores and the PASP values. The AMS score vs PASP at baseline was r2 = 0.02, F = 0.46, P = .50; the AMS score vs PASP after oxygen was r2 = 0.004, F = 0.13, P = .73.
Discussion
We obtained usable data from transthoracic echo in 56 subjects, 36 of whom had TR. Because of the observational nature of this study, we were unable to get sea level data on this study group. However, compared with similar data at sea level, these individuals demonstrated only mild increased PASP at 4250 m; all were within the normal range in spite of evidence of hypoxia by pulse oximetry. Intervention with oxygen, however, reduced the PASP, suggesting preservation of pulmonary vascular reactivity. Based on previous studies, longer time at altitude might be expected to reduce PASP due to acclimatization,12,19 but this did not appear to affect PASP in this group, nor did ascending higher and then returning to 4250 m for the study (Table 1).
Our results were consistent with other studies using both invasive and noninvasive measurements of PASP at altitude.1,7,9–11,19,23–26 However, our study group showed lower PASP readings when compared with studies at similar altitude, which may reflect differences in the study timing and populations and ascent profiles. Ascending according to rapid protocol, as opposed to a self-determined ascent profile, not only leads to higher incidences of AMS but also produces higher PASP values.1,2,11,14 There is also a possibility of selection bias, whereby individuals who suffered significant illness either didn’t volunteer for inclusion in the study or were unable or unwilling to ascend to the altitude where the study was undertaken. Therefore, the study group may accurately represent a healthy cross-section of this trekking population. The authors did not observe these individuals to be especially trained or experienced but rather people who had merely approached the altitude in a controlled fashion and thus avoided significant symptoms.
Although we have inadequate prospective data on the effect of acclimatization on pulmonary artery systolic pressure, our observations at 4250 m suggest that acclimatization and a slow ascent profile may be important factors that lead to lower PASP measurements (in spite of the range of SpO2 suggesting persistent hypoxia).
Study Limitations
Because of the nature of the study, we were unable to get baseline PA measurements as the subjects came from many different countries and were not known prior to the study.
The yield of measurable Doppler signals could have been improved by the use of agitated saline but this option was eliminated by the logistics imposed upon us by the study environment. This was a reflection of the remote setting and transient nature of the subjects’ involvement in the study, making it impractical to perform more invasive procedures, as well as hard to obtain informed consent for them (such as intravenous access).
The estimation of PASP using the modified Bernouille equation ignores viscous friction, which could be a consideration at altitude where the blood viscosity may be altered due to higher hematocrit. However, comparative data have shown that this potential increase in viscosity does not significantly affect measurements at altitude. 11
Conclusions
We conclude that portable echo Doppler cardiography is a valuable tool, which is feasible to use in a very remote high-altitude setting. Improvements in the portability size and power requirements since the time of this study have made it even more versatile. As all the data were within the normal range in this study, we also conclude that pulmonary hypertension was not seen in this well-acclimatized population. In addition, we conclude that oxygen reduces PASP in acclimatized subjects at 4250 m. However, it is also possible that mild increases in pulmonary pressure are seen (compared with sea level values) as reflected in our data, as we also show that the PASP can be reduced with oxygen. As we were unable to obtain sea level data on baseline PASP values in this study population, we do not know in this population if oxygen returns PASP to sea level values or even below sea level values. The presence or absence of mild increases in PASP can be best confirmed by a longitudinal study, making daily observations of pulmonary artery pressures during a controlled ascent over several days or during a rapid ascent. By observing subjects sequentially during an ascent from sea level to their high point, and after a sojourn at high altitude, we may be able to further understand the dynamic changes in HPV as reflected in PASP variability at high altitude. It would then be possible to relate these changes to the differing performance of individuals at altitude, as well as their susceptibility to illnesses such as AMS and HAPE.
Footnotes
Acknowledgments
We would also like to acknowledge the Himalayan Rescue Association for their support in undertaking this study and thank Nelson B. Schiller, MD, for his comments on the manuscript and data.
Funding
This project was supported by a grant from the British Heart Foundation.