
Abstract
Recent studies in normal participants have shown that right to left shunt blood vessels in the lung open up during exercise. We describe the first field study to investigate this phenomenon at altitude. This study aimed to assess the effect of altitude and partial acclimatization on inducible right to left shunting at rest and with exercise. A contrast-enhanced transcranial Doppler imaging technique to detect microbubbles after injection of blood and saline agitated with air was used to measure right to left shunting in 10 normal participants at rest and immediately after exercising to maximum oxygen consumption (V
Introduction
Exercise-induced hypoxemia may have several possible mechanisms, but until recently right to left extra- or intrapulmonary shunting has not been demonstrated. However, through the use of contrast echocardiographic techniques at sea level, it has been shown that exercise induces right to left shunting1,2 through the recruitment of intrapulmonary anastamoses. Particles >50 μm can pass through the human lung, and such shunting could compromise both gas exchange and the ability of the lung to filter out microemboli. 3
For field assessment we have employed a similar approach using contrast-enhanced transcranial Doppler (TCD). Agitated saline (mirobubbles) is injected into a peripheral vein, and early detection of transient cerebral microbubbles is indicative of the presence of an intracardiac shunt. Delayed appearance of the microbubbles is thought to occur when shunting is intrapulmonary. 4 We hypothesized that functional intrapulmonary shunting may become more pronounced at altitude, be further accentuated by exercise, and contribute to hypoxia in these circumstances.
Methods
Participants
Ten healthy, white Europeans (aged 21 to 68 years; 9 males, 1 female) were studied. Their mean and SD physiologic parameters were height 178.4 cm (8.0 cm), weight 77.5 kg (9.2 kg), and body mass index 24.3 (2.1). All were nonsmokers, physically fit, and living at 50 m to 150 m above sea level with no recent exposure to high altitude and were familiar with cycle ergometer–based exercise tests. No participant had a history of hypertension. Measurements were recorded at Coventry, UK (80 m), and after travel to Leh, India (3450 m) by air. The first measurement (acute exposure study) at high altitude was made 24 to 48 hours after arrival at 3450 m. Eight of the group then trekked for 6 days, reaching an altitude of 5289 m; the highest sleeping altitude was 4770 m. The partially acclimatized study was performed on return to 3450 m after the trek on 8 participants (aged 21 to 68 years; 7 male, 1 female). The Research and Ethics Committee of the South Birmingham Health Authority granted approval for the study, and participants gave their written, informed consent.
Experimental Protocol (Figure 1)
Participants rested in a supine position for 30 minutes to allow baseline recordings. An intravenous injection of microbubbles was then given (injection 1), and the participant was monitored for microbubbles for 5 minutes. Participants were then fitted to a supine ergometer (Alticycle, QinetiQ, Farnborough, UK), which allowed continuous monitoring of the middle cerebral artery.
5
Maximum oxygen consumption (V
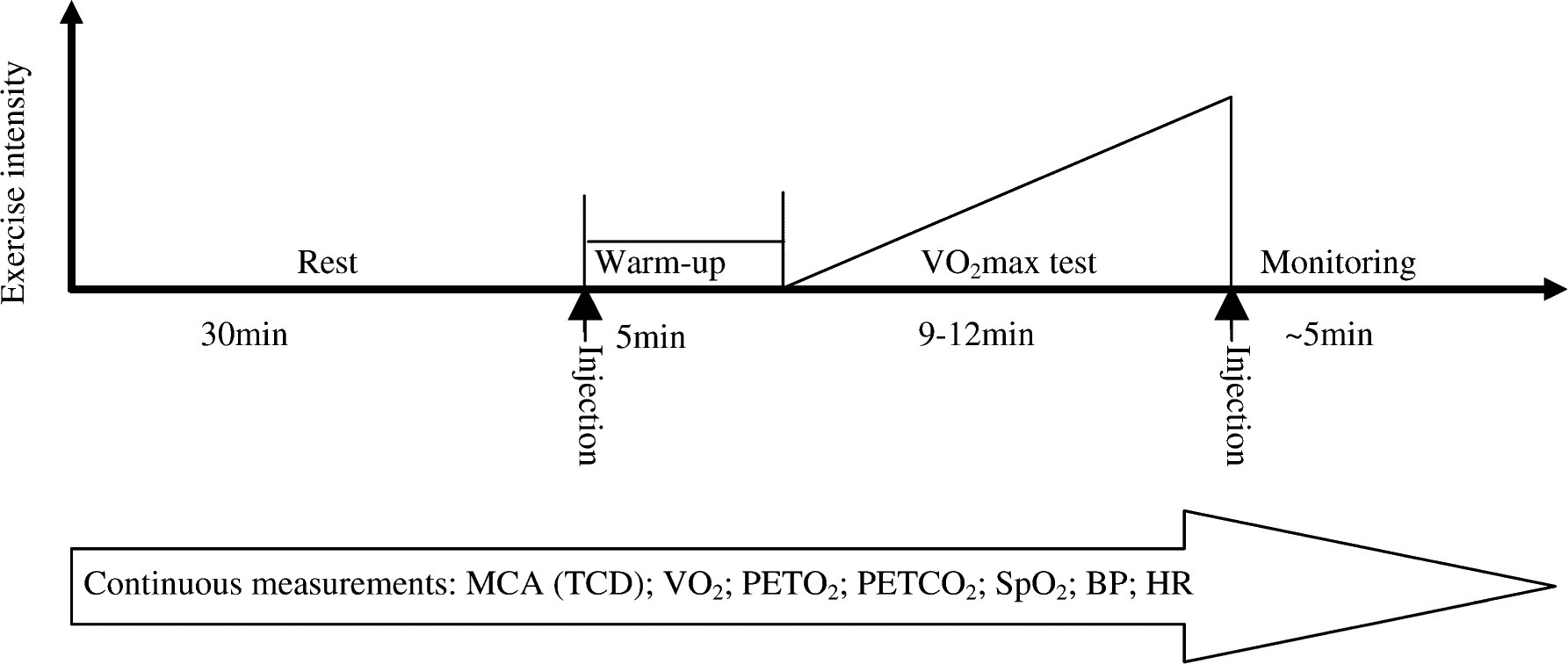
Experimental protocol. MCA indicates middle cerebral artery blood velocity (TCD, transcranial doppler); VO2, maximum oxygen consumption; PETO2, end-tidal oxygen; PETCO2, end-tidal carbon dioxide; SpO2, oxygen saturation; BP, blood pressure; HR, heart rate.
Expired gas was analyzed breath by breath using a Cosmed K4b 2 portable gas exchange unit (Cosmed Srl, Rome, Italy) for oxygen uptake, end-tidal CO2, and minute volume. Gases were collected via a tight-fitting facemask. Arterial oxygen saturation was measured using an Ohmeda Biox 3740 pulse oximeter (Ohmeda, CO). Continuous beat-to-beat blood pressure was measured with a Portapres Model-2 monitor (Finapres Medical Systems, Amsterdam, The Netherlands).
Middle cerebral artery (MCA) blood velocity was measured using a 2-MHz, pulsed-wave, range-gated Doppler ultrasound (DWL Multi-Dop T1, DWL Elektronische Systeme, Singen, Germany). The middle cerebral artery time-averaged mean velocity (cm·s−1) was recorded electronically.
Contrast-Enhanced Transcranial Doppler Assessment of Right to Left Shunting
Gaseous or solid emboli detected by TCD are referred to as transient cerebral microembolic signals. Such signals are unidirectional, occur at random within the cardiac cycle, and are recognizable by their characteristic sound or “chirp.”8,9
A 20-gauge intravenous catheter was placed into the participant's left basilic vein. A 3-way stopcock was attached, and 2 20-mL syringes were attached to the other 2 ports. One syringe contained 2 mL of air, and the other contained 16 mL of sterile saline and 2 mL of the participant's blood. The contrast bubbles were created by flushing the saline solution from one syringe to another repeatedly. Ten milliliters of the agitated saline solution were injected rapidly on completion of the rest period (injection 1). Injection 2 was administered within 5 seconds of completion of the V
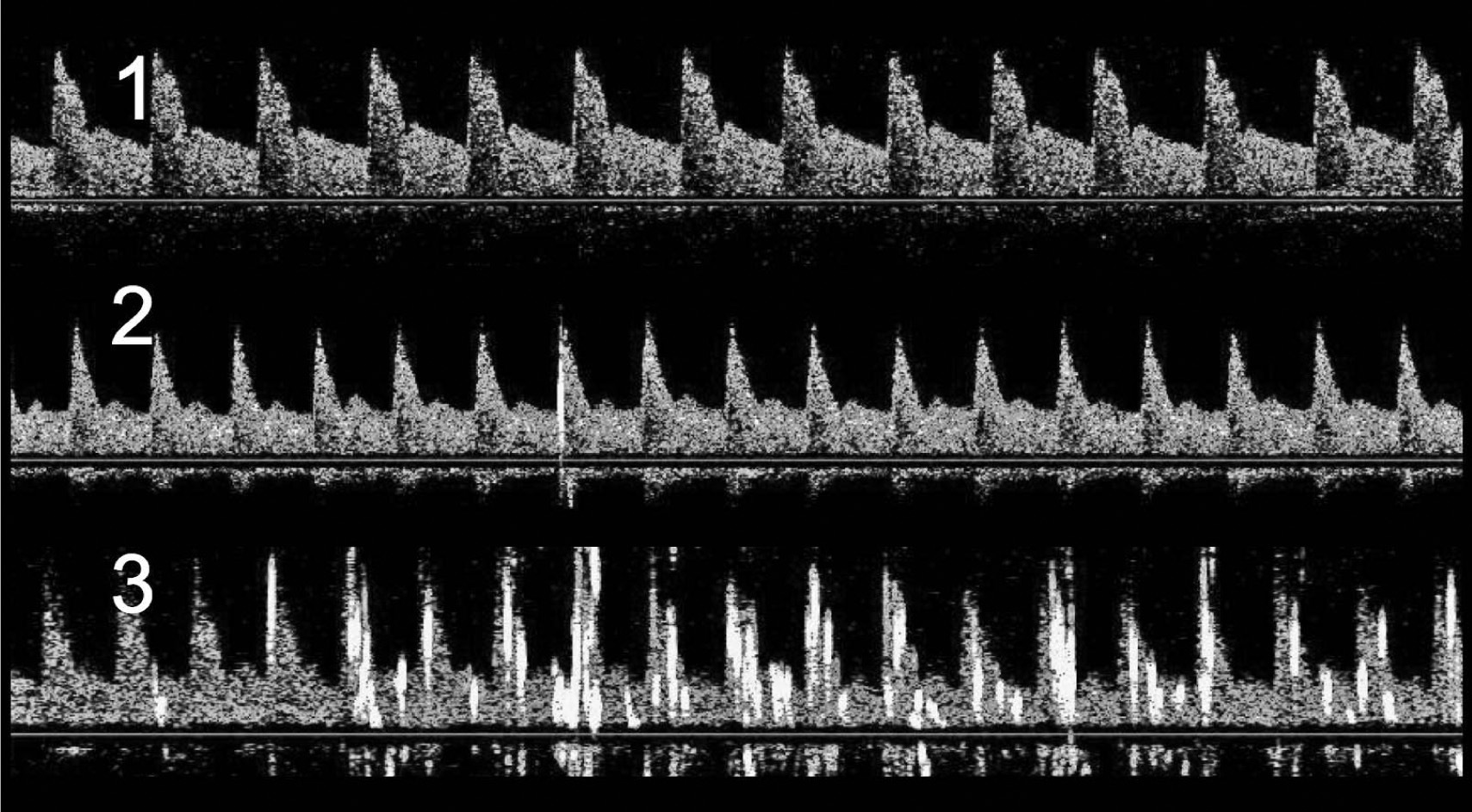
Transcranial doppler traces at maximum oxygen consumption on acute exposure to 3450 m after the injection of contrast media into the left antecubital vein.
Echocardiography
All participants underwent contrast-enhanced transthoracic echocardiography at sea level to assess intracardiac shunting on return to sea level after the altitude observations. Studies, including a valsalva maneuver, were undertaken by an experienced echocardiographer who was blinded to the altitude results (Sonos 5500, Hewlett Packard, Andover, MA).
Statistical Analyses
Data were collected continuously by a laptop computer and a data acquisition device (Power 1401, Cambridge Electronic Design, Cambridge, UK). The K4b
2
data were collected using its own software, and time marks allowed correlation between the 2 data sets. All data are reported as mean and SD unless indicated otherwise. Resting and V
Results
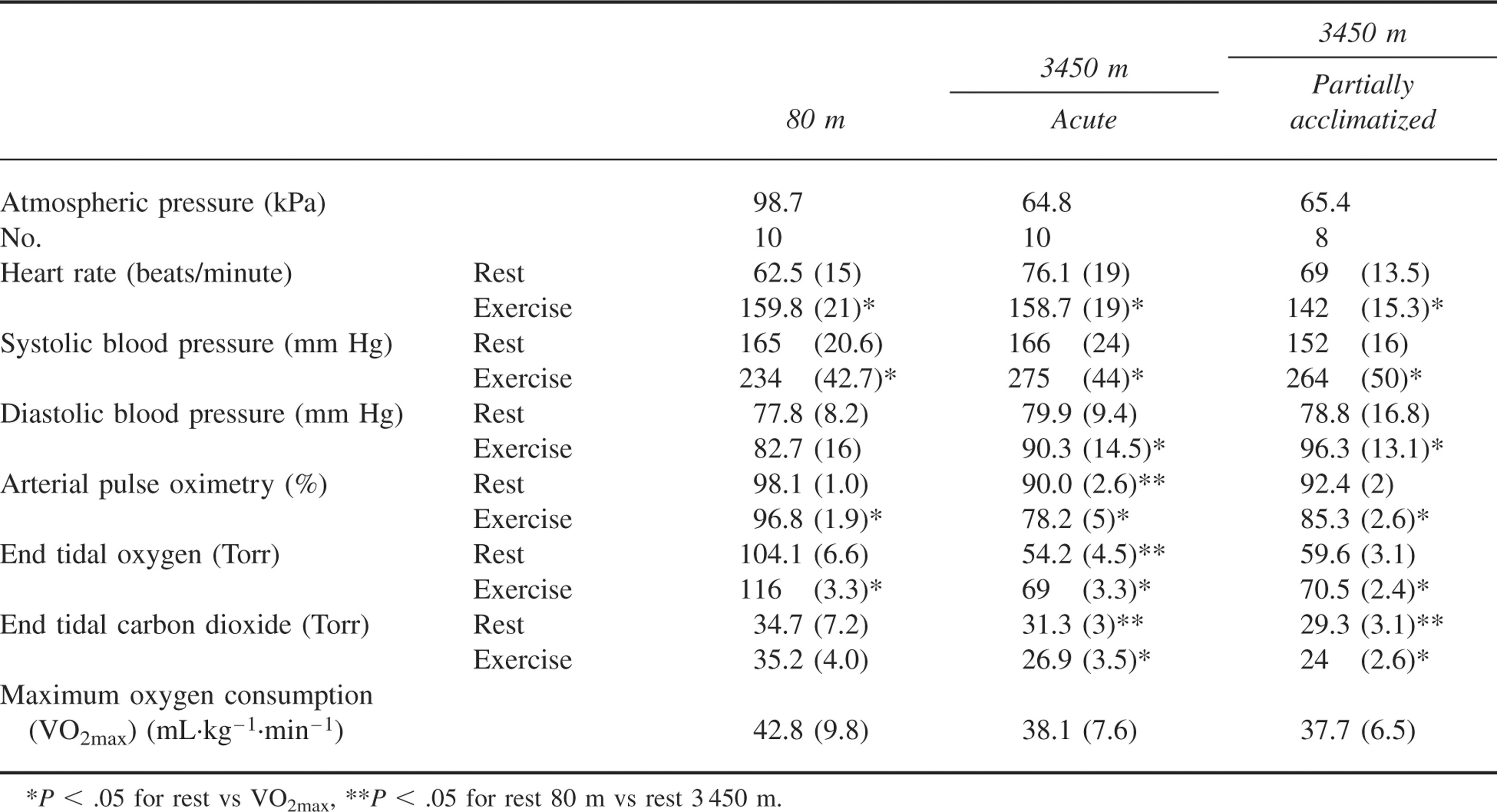
The changes in physiologic parameters are summarized in Table 1. Based upon the number of gaseous cerebral microbubbles detected at V
Cardiorespiratory data; mean (SD)
Cerebral microbubbles as a measure of right to left shunting at 80 m and 3450 m; numbers of cerebral microbub bles detected in the right middle cerebral artery at rest and immediately after exercising to maximum oxygen consumption (VO2max)
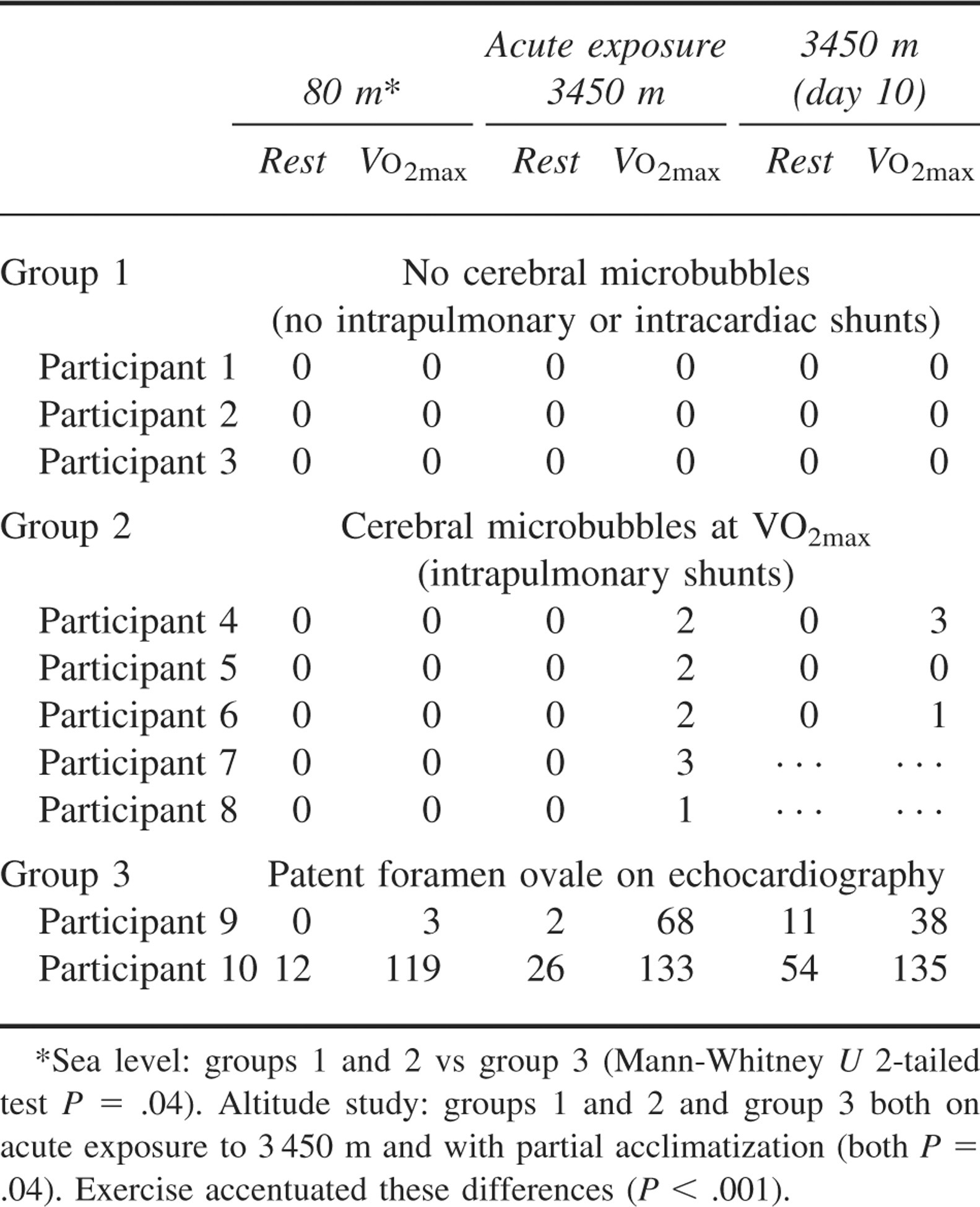
There was a significant difference between groups 1 and 2 vs group 3 (Mann-Whitney U 2-tailed test P = .04). At altitude there was a significant difference at rest between groups 1 and 2 and group 3 both on acute exposure to 3450 m and with partial acclimatization (both P = .04). Exercise accentuated these differences (P < .001).
Discussion
The new findings in this study were that inducible intrapulmonary shunts occurred with exercise at altitude in otherwise fit individuals. Participants with occult atrial right to left shunts demonstrated more shunting at altitude and shunted most on exercise at altitude. Partial acclimatization did not appear to affect the degree of intracardiac or intrapulmonary shunting. There were no significant differences in oxygen saturations, blood pressure, end tidal oxygen, and CO2 in those that shunted compared with those in whom shunts were not detected.
Our findings confirm and extend the observations at sea level1,2 to high altitude but do not suggest that the degree of shunting contributed significantly to exercise-induced hypoxemia. It would seem unlikely that the relatively small shunt fraction calculated at 2.2% 1 would make a significant contribution to hypoxia at low and moderated altitudes. Indeed, our finding of intracardiac shunts in 2 participants, which were larger than the intrapulmonary shunts, was not associated with greater hypoxia. However, the situation at higher altitudes may be different.
There is evidence that contrast-enhanced TCD shows improved accuracy for patent foramen ovale detection compared with transthoracic echo
10
when poor transthoracic echo images are obtained. Contrast-enhanced TCD may have underestimated the amount of intrapulmonary shunting. Saline contrast bubbles are inherently unstable, with survival times that are determined by a number of factors, including bubble size, surface tension, gas concentration gradients, vascular pressures, and ultrasonic energy. Consequently, there are concerns about variation in bubble survival time with exercise. It has been proposed that with exercise, vascular pressures and shear stresses will increase and this will result in an increased rate of destruction of bubbles, particularly in the left ventricle and the arch of the aorta. If this theory is correct, then contrast-enhanced TCD is likely to underdetect right to left shunting. Another factor that may have led to an underestimation of shunting is that the echo contrast was injected 5 to 10 seconds after V
There are several clinical implications, apart from hypoxemia, arising from the finding of intrapulmonary shunts. The contrast microbubbles injected are estimated to be 60 to 90 microns in diameter 11 , consequently microemboli up to this size could theoretically pass through the pulmonary shunts. Strokes and other neurological deficits are well described at high altitude,12,13 and some of these may be caused by paradoxical emboli, as has been shown in studies of ischemic strokes, especially in people younger than 55 years of age. 14 Although flow rather than pressure may be the most important factor in the opening of intrapulmonary shunts, 2 intrapulmonary shunting may act as a protective parallel circuit and could be of importance in avoiding the development of high-altitude pulmonary edema. 1 Failure to open up a parallel circuit may increase the likelihood of capillary stress failure, a postulated mechanism for high-altitude pulmonary edema. High-altitude pulmonary edema has been reported in study participants with an intra-atrial shunt but not confirmed in other participants with similar shunts who did not develop high-altitude pulmonary edema. 15
We have shown that contrast-enhanced TCD is a potentially useful technique for studying shunting in the field and provide a semiquantifiable measure of the level of shunting. 16 Functional right to left intrapulmonary shunting was demonstrated at altitude for the first time, and partial acclimatization did not appear to lessen the effect. Intracardiac shunts, which were of no clinical importance at rest at sea level, increased with exercise and increased still further with exercise at altitude. The physiologic and pathologic significances of intrapulmonary and intracardiac shunting require further study at lesser workloads and at different altitudes, and a larger number of participants are required to assess the effects on hypoxia.
Footnotes
Acknowledgments
This work was supported by a grant from the Arthur Thompson Trust.
Funding
K. Pattinson is supported by the Medical Research Council (UK). There are no financial interests to be declared.
*
Presented at the 15th International Hypoxia Symposium, Lake Louise, Alberta, Canada, February 27 to March 4, 2007.