
Abstract
Objective
Studies on the neurologic effects of high-altitude travel have focused on psychometric and cognitive testing and the long-term effects of hypoxia on memory and cognition. Few authors have discussed overt clinical psychiatric illness during high-altitude travel, and those few have focused on patients with preexisting psychiatric diagnoses. We describe a series of patients with new-onset anxiety disorders at high altitude treated at the Himalayan Rescue Association (HRA) clinic in Pheriche, Nepal (4240 m) in the spring season of 2006.
Methods
We report on all 6 cases of anxiety-related illness diagnosed at the HRA Pheriche Clinic during the spring season, 2006. Three cases, representing the 3 discrete types of illness we encountered, are described in detail.
Results
Six of 76 foreign patients and none of the 224 Nepalis seen during the season had anxiety-related primary diagnoses. None of the 6 patients had a history of psychiatric disorders or anxiety-related problems at low altitude. Three of the 6 patients were seen after hours, and all 6 required multiple visits. We describe 3 types of anxiety-related disorders: limited-symptom panic attacks induced by nocturnal periodic breathing, excessive health-related anxiety, and excessive emotionality.
Conclusions
Anxiety-related illness requires significant use of medical resources by high-altitude travelers. Further research is needed to define the epidemiology of anxiety-related disorders at high altitude, to quantify the contributions of various etiologic factors, and to identify safe, effective treatments.
Introduction
Studies on the neurologic effects of high-altitude travel have focused on psychometric and cognitive testing and the long-term effects of hypoxia on memory and cognition.1,2 Some have considered emotional processing using instruments designed to identify subtle differences in mood states.1,2 Few authors have discussed overt clinical psychiatric illness during high-altitude travel, and much of this work has focused on patients with preexisting psychiatric diagnoses.3,4 As high-altitude tourism results in increasing numbers of people traveling to high altitude who previously might have avoided the rigors of high-altitude travel, the number of anxiety-related medical problems at high altitude may be increasing. 4 In this article we briefly describe our experience with anxiety-related disorders at the Himalayan Rescue Association (HRA) clinic in Pheriche, Nepal (4240 m), and we describe in detail 3 cases representing discrete manifestations of anxiety-related problems that we encountered at the HRA. We discuss some of the possible causes and treatments of these problems. We hope this will stimulate more research into this important and not uncommon phenomenon.
Cases
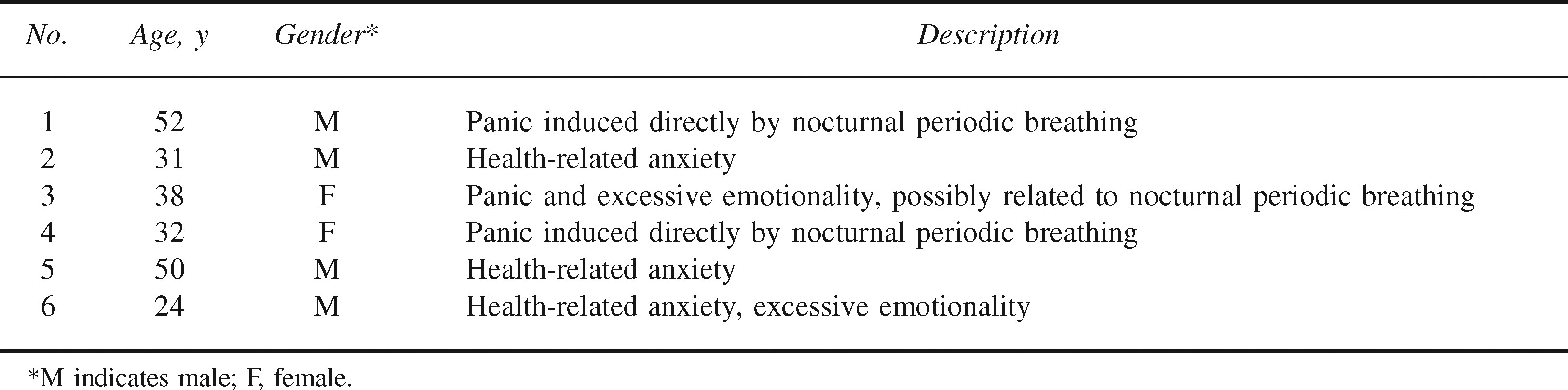
From March 3, 2006, through May 14, 2006, we saw 300 patients at the HRA Pheriche Clinic. Two hundred twenty-four of these patients were Nepali, and 76 were foreign trekkers. We identified no cases of anxiety-related disorders in Nepalis and 6 cases in foreign trekkers. Demographic characteristics and brief descriptions of the anxiety-related problem of each of these patients are found in the Table. None of the patients had a history of psychiatric illness. Every anxiety-related case required at least 2 physician visits, and 3 patients were seen after hours. Below we describe in detail 3 cases that represent 3 different types of anxiety-related disorders that we came to recognize: anxiety or limited-symptom panic attacks caused directly by nocturnal periodic breathing, health-related anxiety in a subject not prone to this phenomenon at low altitude, and excessive emotionality. By our institutional standards, this type of report does not require institutional review board approval or written informed consent from patients.
Anxiety-related cases presenting to the Himalayan Rescue Association Pheriche Clinic, spring 2006
Case 1
A 52-year-old male ascended without difficulty from Lukla, Nepal (2840 m) to Pheriche over 5 days. The patient had a history of mild hypertension, took no medications, and denied alcohol use. He had never previously slept higher than 2800 m. He developed shortness of breath while attempting to sleep during his first night in Pheriche. He described that he awakened gasping for air and subsequently was unable to catch his breath, stating he was “unable to establish a rhythm to his breathing.” Lying supine exacerbated the condition and induced a sensation of panic. He presented to the HRA clinic at 3:00
On presentation, the patient was an obese-appearing male in no apparent distress. His respiratory rate was 16, room air oxygen saturation was 89% (normal for the altitude), and heart rate was 78 with a regular rhythm. His lungs were clear to auscultation bilaterally, and lower extremities were without edema or tenderness. The patient was given 125 mg of acetazolamide to treat periodic breathing and sleep disturbance and was advised to return to the clinic if symptoms persisted. He returned the next morning and described good sleep throughout the rest of the night.
The following day the patient took an acclimatization hike to approximately 4600 m without undue difficulty or dyspnea before returning to Pheriche. That night he took 125 mg acetazolamide before bed but awoke numerous times with shortness of breath and described repeated episodes of panic-inducing gasping for breath. The following morning he again returned to the clinic for evaluation of these nocturnal symptoms. Repeat examination was similarly unremarkable. Largely to reassure the patient, chest ultrasonography was performed, which revealed no evidence of pulmonary edema, pleural effusion, or pericardial effusion. In spite of reassurance about his medical condition, the patient decided to descend.
Case 2
A 31-year-old, well-conditioned climber with extensive high-altitude experience to over 7000 m traveled to Nepal as part of a team attempting to climb Mt Everest (8848 m). He had no past medical or psychiatric history and he denied alcohol use. The team flew to Lukla and walked to Namche (3450 m elevation) the following day. After spending the night in Namche, the patient awoke with a dry cough and sore throat. While the rest of the team continued the trek up to Everest Base Camp, the patient spent 3 rest days in Namche. His symptoms persisted and he returned to Kathmandu, where he underwent a medical assessment and was given a course of antibiotics for a presumed upper respiratory tract infection. Four days later he returned to Lukla feeling refreshed. The following day he trekked to Pheriche.
The patient spent 2 days in Pheriche, during which he presented to the HRA clinic on 3 occasions for reassurance, including repeated oxygen saturation checks (at his request), although he was experiencing no symptoms and had undertaken acclimatization hikes to 5000 m without difficulty. The physical exam, including vital signs and oxygen saturation, was uniformly normal. Eventually he ascended to Lobuche (4900 m) and on arrival noted a slight subjective fever. During the night he slept poorly, and he described being unable to catch his breath and a feeling that he “couldn’t get enough oxygen into his lungs.” This was not specifically linked to gasping or periodic breathing. He also described a sensation of “lack of oxygen to his fingers,” although he denied numbness, weakness, or parasthesia. Other than poor sleep, there were no symptoms of acute mountain sickness. The following morning he descended to Dughla (4620 m), where he spent the day resting; however, that evening breathlessness and anxiety returned, and the next day the patient descended to Pheriche and presented again to the HRA clinic for evaluation. On arrival he was well and in no apparent distress, with normal vital signs and physical exam. He was reassured and advised to commence acetazolamide 125 mg before bed for his nocturnal symptoms. That night he slept well, and after presenting again to the HRA clinic for evaluation, he departed for Dughla. Several days later he arrived at Mt Everest base camp but was not welcomed back to his expedition and so left for home shortly thereafter.
Case 3
A 38-year-old woman ascended from Lukla to Pheriche over 6 days without difficulty. The afternoon after sleeping in Pheriche she presented to the HRA clinic complaining of shortness of breath associated with tightening of her throat, anxiety, and tearfulness at night and with mild exertion. The night before presentation, while in Pheriche, she awoke gasping for breath. She felt that her throat was “constricted” and that she could not get enough air as a result. She became anxious and tearful and awakened one of her traveling companions to ask for assistance. After about an hour of efforts to calm her, which included encouragement of slow, deep breathing, she was able to get back to sleep. She was awakened by a similar episode at 5:00
On presentation she complained of the sensation of throat constriction described above, but also of her multiple crying episodes, which she deemed extremely atypical, stating “this is not like me at all.” Even during these episodes she was perplexed by them and was unable to explain to herself or her companions why she was so upset. She denied cough, sore throat, congestion, fever, or acute mountain sickness symptoms other than difficulty sleeping. She had no history of medical or psychiatric illness. She usually drank 1 to 2 glasses of wine with dinner, but she had abstained from alcohol since arriving in Lukla. She had never previously slept higher than 3200 m. She took no regular medications, but she had taken acetazolamide (125 mg) once on the morning of presentation. On exam she was alert and oriented, in no acute distress, and appeared calm. Vital signs and oxygen saturation were normal. Head and neck exam was normal, there was no erythema or exudate in the oropharynx, no lymphadenopathy, and no stridor. The remainder of the physical exam was also unremarkable. She was reassured that her symptoms were not grave and was encouraged to take another 125 mg of acetazolamide before bed to limit the periodic breathing that may have precipitated her initial attack. She did so and slept well but was so unnerved by her experience of the day before that she decided to descend.
Discussion
In addition to the 6 patients who presented acutely to the clinic with anxiety-related complaints, a number of other trekkers sought our advice after similar episodes or relayed stories of companions who had terminated their treks because of insurmountable anxiety of one form or another. This indicates that anxiety may be a common phenomenon at high altitude and that cases presenting to medical professionals may represent only a fraction of clinically significant disease. As is the case at low altitude, clinically relevant anxiety-related problems at high altitude may be underrecognized. 5 Whether the 6 new-onset cases we report here represent an unusually high incidence of anxiety-related problems is impossible to know given the heterogeneous and transient population of the Khumbu during the time covered by this report and our inability to capture all cases.
In a study by Basnyat and Litch 6 of 155 porters and trekkers in the Nepal Himalaya, the only 2 cases of anxiety were in porters, and these cases resulted in 2 of the 7 medical evacuations undertaken, though no other details are available. This Nepali predominance is in contrast to our experience in Pheriche, and the discrepancy is difficult to explain given our methodology and the limited data available from the other study. It must be considered that the exclusive presence of English-speaking physicians at the HRA clinic (although a translator was always immediately available) may have discouraged Nepali patients with anxiety-related problems from presenting or may have inhibited our ability to identify anxiety-related problems in Nepalis. In the study of Basnyat and Litch, subjects were interviewed by a Nepali physician. Additionally, because of cultural differences, Nepalis as a group may have been less prone than foreign trekkers to approach any physician with a psychiatric problem. Though the countries of origin of our patients were not reported to protect their identities, it should be noted that these patients were diverse, including 2 patients from North America, 2 from Western Europe, 1 from Eastern Europe, and 1 from Asia.
Insofar as high-altitude travel may have played a role in the psychopathology we describe, we suggest that this may be mediated by a combination of hypoxia's direct effects on the brain, its secondary physiologic effects (such as hyperventilation and periodic breathing), and the remoteness of the setting described in this report. Nocturnal periodic breathing was at least implicated in all of the cases we detail here. Periodic breathing and frequent arousals during sleep are well-described phenomena at high altitude. 7 Ongoing shortness of breath and anxiety symptoms after waking have received little attention, although anxiety has been associated with sleep apnea and nocturnal panic is common in panic disorder patients at low altitude.8,9 Common models of panic (specifically, the hyperventilation and suffocation false-alarm models) implicate some of the same physiologic processes that occur during exposure to hypoxia, particularly those responsible for nocturnal periodic breathing. 3 Hyperventilation also occurs during normal acclimatization while awake and may, if we accept these theories of anxiety, contribute to some of the anxiety-related psychopathology that we describe in waking patients.
While anxiety may manifest as a behavioral reflex to certain physiologic conditions, such as hyperventilation or hypocarbia, anxiety may also be considered an emotional product of cognitive processing. 10 How hypoxia affects this processing is unknown. The health-related anxiety we describe in case 2 and noted in others may result from the hypoxic misinterpretation of normal stimuli. For example, slight shortness of breath with exertion, which might be evaluated and discarded as unimportant at low altitude, could be interpreted by the hypoxic brain as dangerous and thus anxiety provoking. 10 Hypoxia has been shown to impair cognitive and reasoning ability in multiple studies. 1 It could also be implicated, via a cognitive pathway, in clinical anxiety disorders at high altitude.
The relative degrees to which the setting of Pheriche and actual high altitude contributed to the psychopathology in these cases deserve attention. Certainly, knowledge that evacuation is difficult and prolonged in the Khumbu Valley could provoke anxiety in many people who would not experience such anxiety in a less remote setting at the same altitude. Similarly, the unfamiliar culture of Nepal, rather than altitude, might cause anxiety in foreign travelers. 11 While awareness of altitude illness among travelers has probably contributed to a significant decrease in the incidence of serious altitude illness, such as high-altitude pulmonary or cerebral edema, in the Khumbu Valley over the last several decades, such awareness may also fuel anxiety in some people and lead to the types of problems described above. 4 All the cases described above involved travelers who were well informed about altitude illness and who were traveling with friends on noncommercial trips without professional guides. Our anecdotal experience is that many travelers, wary of the possibility of serious altitude-related illness, may become hypersensitized to their bodies and seek repeated medical evaluation for extremely mild symptoms (for which they would not normally seek medical attention) or just for reassurance. The absence of commercial trekkers in our series may indicate that informed reassurance, even from a nonmedical professional such as a guide, could play a role in mitigating the seriousness of anxiety-related problems or in obviating the need for professional medical assistance when acute problems do occur. Education must strike a balance between adequately conveying the possible perils of high-altitude travel while not provoking unwarranted anxiety in high-altitude travelers. While shortness of breath and discomfort at night at altitude may sometimes warrant evaluation for more serious causes, increased awareness among high-altitude travelers of nocturnal periodic breathing, other physical responses or sensations occurring at high altitude, and the possibility of anxiety or panic attacks might help allay concerns and allow these travelers to recognize certain phenomena as benign, possibly defusing the panic response before it becomes overwhelming.
The paucity of prior studies limits our ability to offer evidence-based recommendations geared specifically to the treatment of anxiety-related problems at high altitude. Cognitive therapy, including education about sensations related to hyperventilation, has had mixed success in panic disorder patients at low altitude. 3 Benzodiazepines are recommended for the short-term treatment of panic disorder at low altitude and can be useful for a variety of other anxiety-related disorders. 12 Increasing evidence has shown that these medications improve sleep quality and reduce periodic breathing at high altitude without adverse effects on oxygenation or acclimatization. 13 If future research continues to dispel concerns about their potentially detrimental effects on adaptation to high altitude, limited doses of benzodiazepines may be considered for anxiolytic therapy at high altitude. Acetazolamide improves sleep and reduces nocturnal periodic breathing at high altitude. 7 Many of acetazolamide's proposed mechanisms result in increased ventilation. 7 How this might influence anxiety, which may be exacerbated by hyperventilation, has not been studied. The nonbenzodiazepine hypnotic zolpidem improves sleep at high altitude, including reducing the arousals associated with the hyperpneic phase of periodic breathing, without preventing periodic breathing or otherwise significantly influencing respiration. 14 Whether these sleep-related effects alone, in the absence of independent anxiolytic or respiratory effects, can influence the types of anxiety experienced at high altitude is unknown, but may bear investigation. As in other altitude-related illness, descent should always be considered a simple, safe, and likely effective therapeutic option for altitude-related anxiety.
The problem of newly acquired anxiety disorders at high altitude deserves further study. Future research might attempt to define the epidemiology of anxiety and panic disorders at high altitude, quantify the contributions of our proposed etiologic factors or identify others, describe the effects of high altitude on people with preexisting anxiety disorders, and identify safe, effective treatments.
Footnotes
Acknowledgments
The authors would like to thank the Himalayan Rescue Association for the opportunity to staff the Pheriche Clinic and for access to the clinical data for publication.