
Abstract
The prevention and management of venomous snakebite in the world's mountains present unique challenges. This paper presents a series of practical, clinically sound recommendations for management of venomous snakebite in a mountain environment. The authors performed an extensive review of current literature using search engines and manual searches. They then fused the abundant knowledge of snakebite with the realities of remote first aid and mountain rescue to develop recommendations. A summary is provided of the world's most troublesome mountain snakes and the mechanisms of toxicity from their bites. Preventive measures are described. Expected symptoms and signs are reviewed in lay and medical terms. A review of currently recommended first-aid measures and advanced medical management for physicians, paramedics, and other clinicians is included. Venomous snakebites in mountainous environments present unique challenges for management. This paper offers practical recommendations for managing such cases and summarizes the approach to first aid and advanced management in 2 algorithms.
Introduction
Managing medical emergencies in mountainous terrain demands unique measures to deal with limited on-scene resources; communication and transportation difficulties; ongoing environmental stresses on victims, rescuers, equipment, and supplies; and protecting the patient from hazards inherent in mountain rescue. Standard preparation and training are oriented towards the injuries resulting from mechanical trauma that constitute the majority of mountain emergencies. 1 There is a need, however, for mountain travelers (“mountaineers”) and mountain rescuers to have a working knowledge of unusual emergencies, such as snakebite, both to prevent such injuries and to initiate appropriate management when necessary.
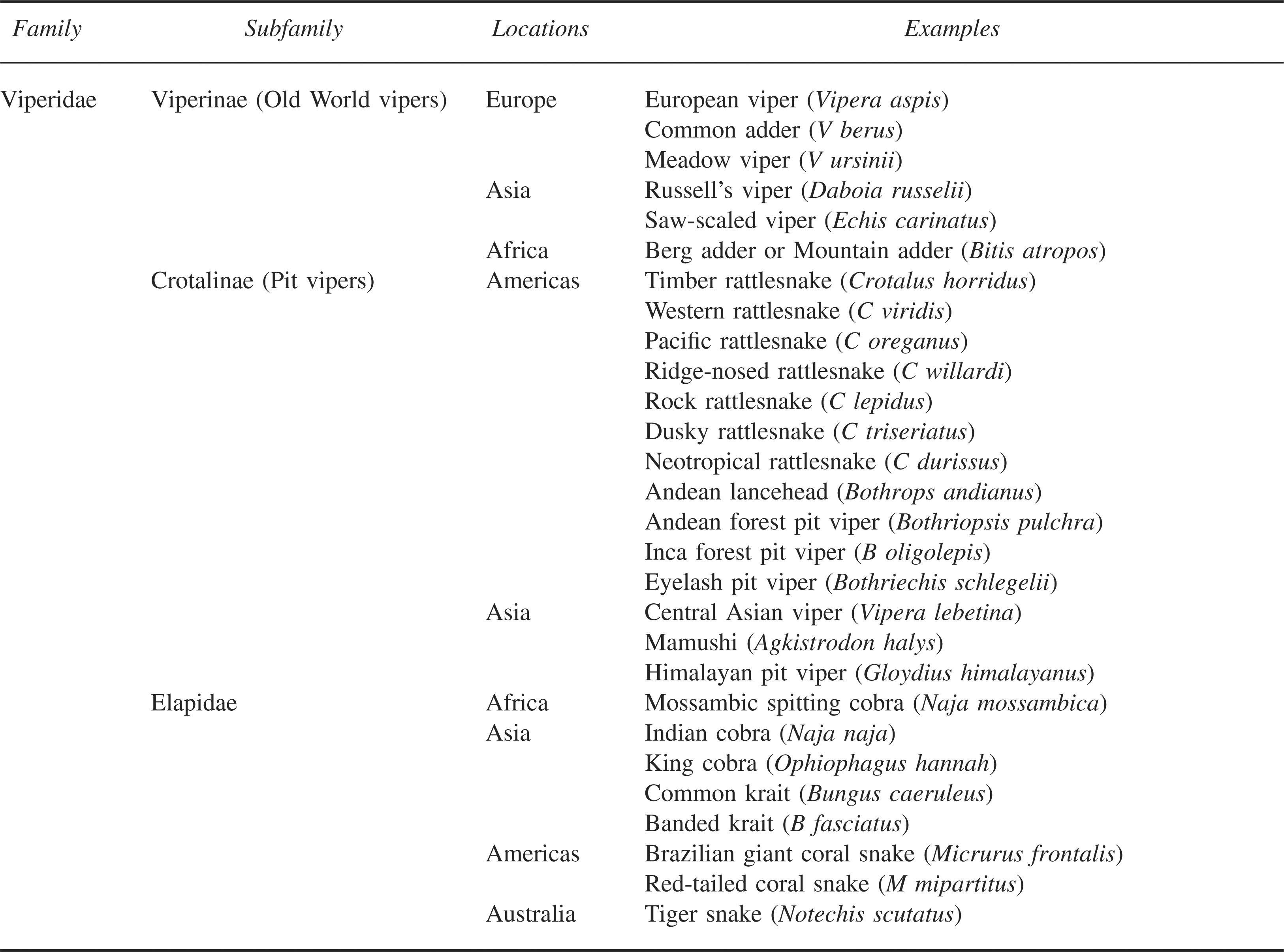
Venomous snakes are found in a number of mountain habitats (Table 1), and bites occasionally occur in remote mountain settings. Management of such bites involves a wide spectrum of priorities. General prevention and management are comprehensively described in first-aid manuals 2 and in emergency medicine textbooks.3,4 Such texts are rarely available at the scene during a mountain rescue, and communication links to obtain outside advice may not be available in remote areas or if communications fail. 5 For these reasons, the Medical Commissions of the International Committee for Alpine Rescue (ICAR) and the International Mountaineering and Climbing Federation (UIAA MEDCOMS) have compiled the core knowledge and recommendations presented in this article.
Examples of venomous snakes found in mountainous terrain
Methods
Reference articles were located by searching Pub Med, EMBASE, and Google Scholar using the phrase “snake bite” and similar terms. In addition, appropriate reference textbooks were hand searched. The search returned more than 3500 references that were then examined for relevance and current content. From these references, the recommendations found herein were developed.
Epidemiology
Venomous snakes inhabit the foothills and mountains of all the continents except Antarctica. Terrestrial snakes that are of most concern in the mountains are from the families Viperidae (vipers and pit vipers) and Elapidae 6 (Table 1).
Globally, only approximately 15% of the 3000 species of snakes are considered dangerous to human beings. 7 Of venomous snakebites reported in the United States, it is estimated that significant envenomation occurs in only 80% of pit viper bites and 75% of coral snake bites.8,9 In other regions of the world, nonenvenomations or “dry bites” also occur with regularity. The case fatality rate from pit viper bites in the United States has improved from 5 to 25% in the nineteenth century to 2.6% with the advent of critical care and to 0.28% with the introduction of antivenom. 3 Similarly, in South Africa and Europe, the case fatality rate is currently reported as 0.3%. 10 However, in developing countries, case fatality rates are reported to be considerably higher, with Nepal reporting a fatality rate of 27% in envenomed victims. 11
Mechanisms of toxicity and symptoms and signs
It is important for those venturing into wilderness environments to learn the patterns of effects for the snake species found in their destinations. Snake venoms, particularly viperid venoms and necrotizing elapid venoms, contain many enzymes and other toxins (low–molecular weight polypeptides) that disrupt cellular processes, resulting in vascular damage and tissue destruction (eg, muscle cell disruption ;obrhabdomyolsis;cb). This results in tissue loss and release of potassium into the circulation. If potassium levels rise high enough (hyperkalemia), this may cause heart irregularities (dysrhythmias). Muscle destruction also releases protein (myoglobin) into the circulation, and this can result in kidney damage (acute renal failure). Vascular damage allows leakage of fluid into the tissues, resulting in peripheral edema, pulmonary edema, hypovolemia, and metabolic acidosis.3,4 Other toxins disrupt the coagulation process. Some promote coagulation and result in diffuse intravascular clotting that can, rarely, result in heart attacks (coronary artery thrombosis) or strokes.12,13 More commonly, snake venoms result in the consumption of blood-clotting factors and may produce incoagulable blood and excessive bleeding at essentially any site 14 (eg, bleeding in and around the brain [intracranial hemorrhage] 15 ).
Venom components, especially in many of the elapids, can also poison the nervous system, causing numbness and muscle weakness, including weakness of the muscles of respiration leading to respiratory failure. Cardiac toxins can result in poor pumping of the heart (myocardial depression), as well as direct rhythm irregularities (eg, atrial fibrillation, atrioventricular block, ventricular tachycardia or fibrillation).16,17
Envenomation can cause early cardiovascular collapse (syncope, shock, cardiopulmonary arrest), notably in bites from European vipers (Vipera species),18,19 Australian brown snakes (Pseudonaja species), 20 and some rattlesnakes.21,22 Early collapse may be due to fainting (neurogenic syncope), direct cardiac toxins, or severe allergic (anaphylactic or anaphylactoid) reactions.18,20,22,23
In general, vipers tend to cause significant local effects (pain, swelling, bruising, and tissue necrosis) due to cellular and coagulopathic toxins, although they may also cause systemic effects, including bleeding, shock, and cessation of breathing in severe envenomations. 24 A few viperid species, such as certain populations of the Mohave rattlesnake (Crotalus scutulatus), have neurotoxic components in their venoms that can cause significant neurological dysfunction in the absence of impressive local findings. 25
Many elapid venoms are predominantly neurotoxic and tend to cause fewer local effects. These snakes may cause paralysis (through either pre- or postsynaptic neurotoxins). Early findings after significant bites by these snakes tend to involve cranial nerve abnormalities (eg, eyelid drooping [ptosis], difficulty speaking [dysarthria]) but may progress to disruption of breathing (respiratory failure). Some elapids, such as the Australian common tiger snake (Notechis scutatus) and eastern brown snake (Pseudonaja textilis), can cause clotting problems, resulting in widespread bleeding. 14 Other elapids, such as Asian and African cobras, can cause significant local injury and severe necrosis.26,27 Spitting cobras (certain Naja sp) and rinkhals (Hemachatus haemachatus) can accurately spit venom into the eyes of a victim from a distance of up to 2.5 meters. This causes severe conjunctival irritation and produces temporary or permanent impairment of vision. 4 Systemic envenomation does not follow isolated ocular exposure to spitting cobra venom.
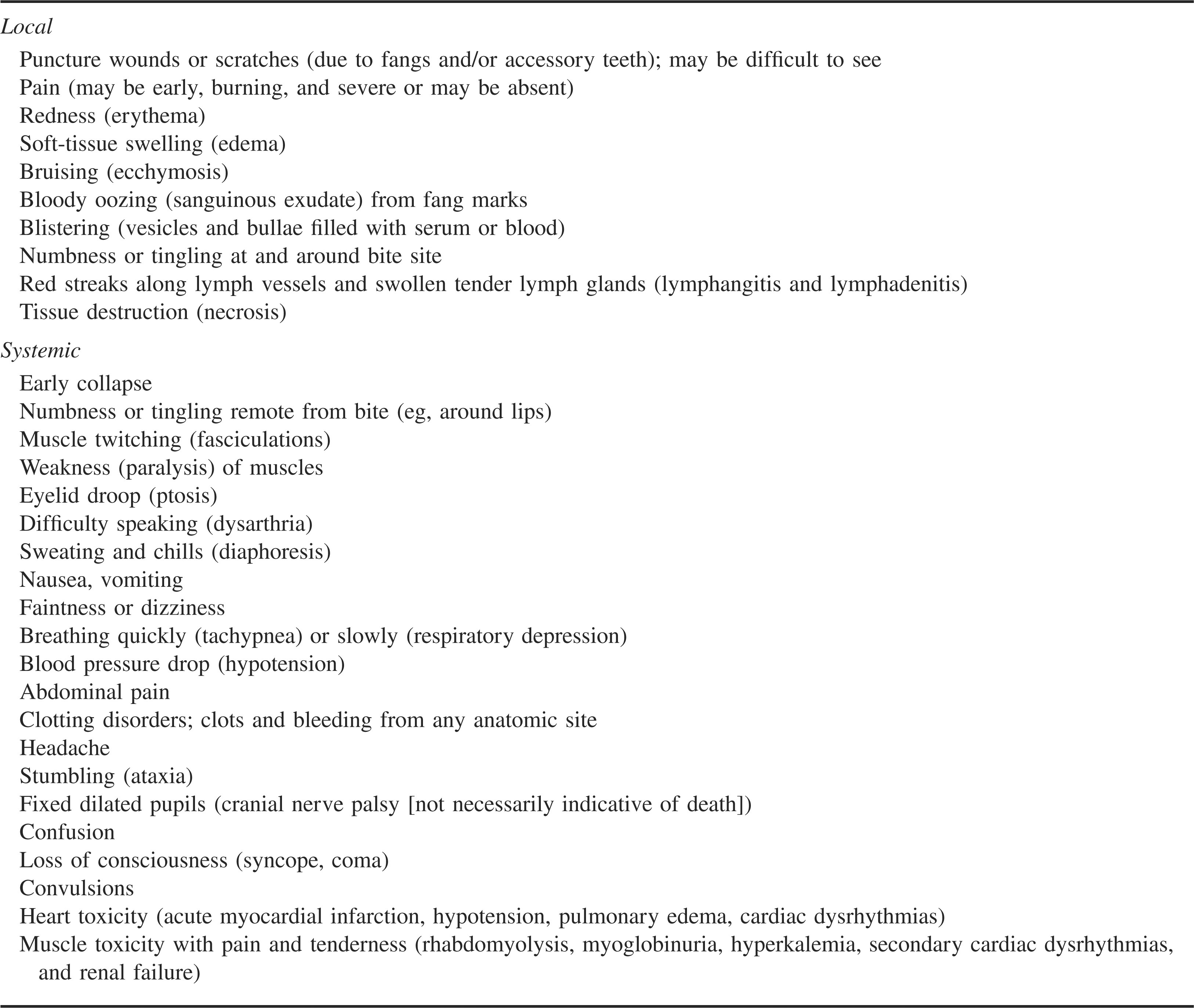
These generalities aside, every snakebite is different. There are countless variables involved in any particular incident including the species and health of the snake, the health of the victim, environmental conditions, and the care rendered. Thus, with a suspected venomous snakebite, the caregiver must be vigilant for the onset of a varied and complex sequence of outcomes; local changes, bleeding, neurological dysfunction, renal failure, cardiovascular collapse, and respiratory distress being among the most important. Some of the possible symptoms and signs of envenomation are listed in Table 2.
Some local and systemic symptoms and signs of venomous snakebite
Prevention
Conscientious application of preventive measures during rescue and other operations can reduce the risk of snakebite even in areas with a high density of venomous snakes. 28 Before going into a new area, gather as much information about the local snakes as possible, including color photographs of indigenous species to be used for identification purposes. This will promote appropriate preventive behaviors, dictate what emergency equipment and supplies should be carried, and direct the most appropriate management should a bite occur. Clinicians traveling with expeditions to remote ranges should develop a snakebite management plan that considers limited logistics, methods of evacuation, and access to antivenom resources. Preventive measures should include wearing adequate protective clothing such as long baggy trousers, long boots or gaiters, and thick socks when traveling in areas where venomous snakes may be encountered.29,30 Baggy (bloused) clothing provides some barrier protection and may reduce the depth of penetration if a bite occurs.
While walking, always scan the path ahead and look around carefully before squatting or sitting down. Probe ahead of you with a walking stick before entering an area with an obscured view of your feet. If preparing to step over a log, scan the other side before proceeding. Avoid putting hands into areas where snakes may be hiding, such as in long grass, under rocks or logs, in trees, or on rock ledges. Gloves add a degree of protection. Be aware of snakes even in vertical places (eg, on ledges or in fissures while climbing) or in the water (eg, while canyoneering).
If a snake is seen, no attempt should be made to approach, capture, or kill it. Many bites occur to victims attempting to move or kill a snake. If a snake has been killed, it should not be handled because recently killed snakes possess a reflex biting mechanism for some time after their death, and fatalities have occurred in victims bitten by decapitated snake heads. 31 In addition, venom remains active in dead snakes for long periods and can result in envenomation if a person is penetrated by a fang while handling the specimen. 32
Use a torch or flashlight at night when walking, and never go about with bare feet. Do not sleep in the open or in poorly sealed accommodations 33 in areas where snakes are common, and do not put sleeping bags near rocks, cave entrances, or rubbish piles. Carefully check your sleeping bag, boots, and other equipment before use.
Onsite treatment
Most recommendations for managing venomous snakebites are based on limited studies, and these recommendations should, therefore, be considered guidelines only. First aid and advanced medical treatment are summarized in Figures 1 and 2.
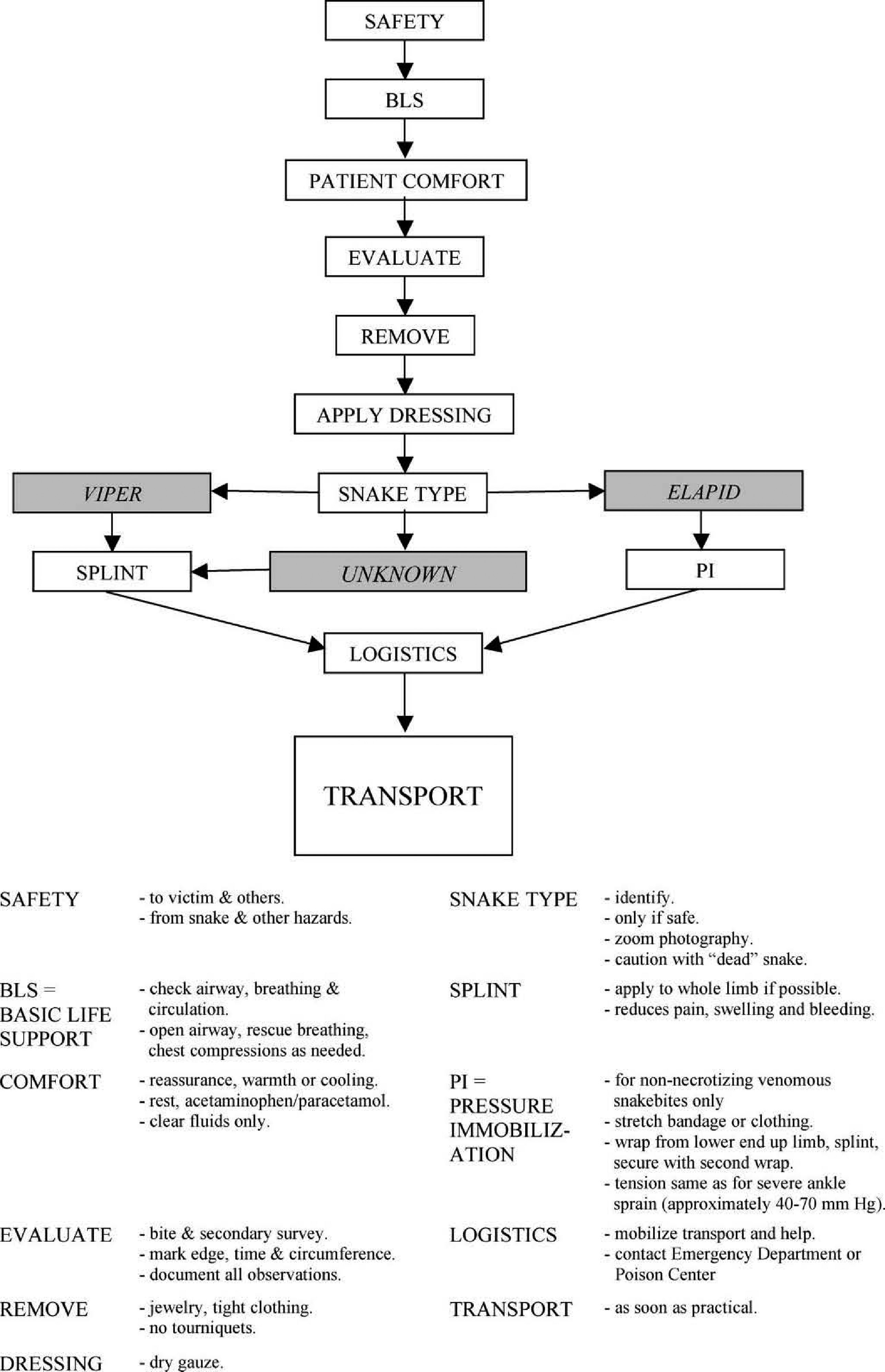
First-aid algorithm. Transportation is a priority and should be organized as soon as possible.
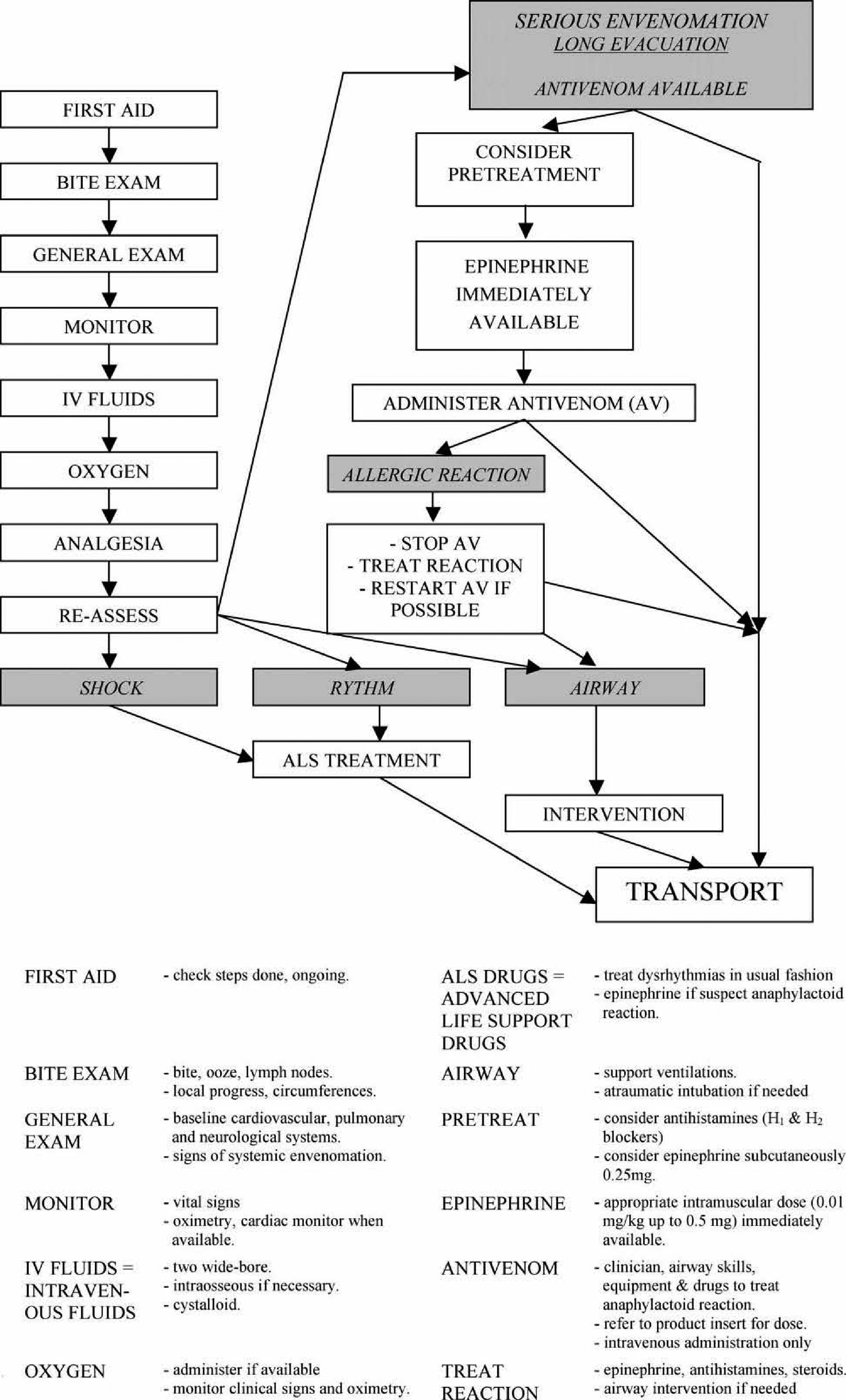
Advanced field medical treatment algorithm.
Snake Identification
Interviewing the victim and witnesses may reveal useful identification information. 34 Digital photography of the snake using zoom settings may be helpful, but the snake should be approached only if it is safe to do so. A snake's effective striking range is approximately half its body length. The remains of a killed snake, if needed for identification, are best maneuvered into a thick receptacle (eg, heavy rucksack) with a stick or trekking pole. Because all US pit vipers are adequately covered by crotalid antivenoms available in this country, precise species identification of US pit vipers is not necessary. It is important in other regions of the world to carefully identify the snake, because antivenoms in these regions may be species specific. 35 Being able to differentiate a venomous snake from a nonvenomous snake is certainly worthwhile, because a bite by a harmless snake should not necessarily end an outing.
First Aid
Safety, basic life support, victim comfort, secondary survey
Initial considerations for first aid should follow standard approaches and incorporate safety, basic life support, 36 comfort of the victim, and a targeted secondary survey. Cardiopulmonary resuscitation may be lifesaving and immediately necessary in snakebite that produces early collapse.18,22 Prolonged rescue breathing may be necessary. 37
Evaluate bite, remove constrictions
The bite should be examined, and the leading edge of swelling marked indelibly with a line, along with the time of the observation in order to track progression. The circumference of the limb at a marked site above the wound can also be noted. If local effects progress, re-mark the perimeter with the time and measure the circumference every 30 minutes or more frequently if advancing quickly. Rings, watches, and constricting clothing should be removed to avoid a tourniquet effect as swelling progresses.
Do no harm
Incision, excision, heat, ice, cryotherapy, poultices, topical chemicals or herbals, electrical shocks, alcohol, or stimulants offer no benefit and may worsen outcomes.38,39
Mechanical suction not recommended
Recent evidence indicates that mechanical suction devices do not extract venom, may impair natural oozing of venom from the bite, and may increase tissue damage. 40 –43 Their use is, therefore, not recommended.
Dressings
The bite site should not be manipulated, although a simple, dry dressing can be applied.
Constriction bands and tourniquets
Constriction bands and tourniquets have never been found to improve outcome and should be avoided because of their inherent risk of worsening local tissue damage.
Pressure immobilization
Pressure immobilization (PI) is now recommended in many regions of the world for non-necrotizing elapid snakebites because it reduces absorption of these neurotoxic venoms into the central circulation. 44 –46 To apply pressure immobilization, a broad elastic or crepe bandage or a torn item of clothing is bound from the distal portion of the bitten limb firmly up over the bite site, at similar pressures as for a severely sprained ankle. 47 The bandage is then wrapped up the extremity as far as possible and the limb is splinted or placed in a sling (Figure 3). 48 For PI to be effective, the pressures achieved by the wrap must be within a narrow range (approximately 40–70 mm Hg). 49 Pressures outside of this range are ineffective and may actually enhance venom spread. 50 Use of a splint or sling is also required for the technique to work, and the victim must be carried from the location. Pressure immobilization should not be used if the offending snake's venom is of a necrotic variety, as with most vipers, pit vipers, and certain Asian and African cobras, due to the risk of worsening local venom effects.26,27 When used, PI should be left in place until the patient reaches definitive care and antivenom, if indicated, is started. 39 Definitive proof of efficacy of this technique or ability of rescuers to apply it remains lacking.
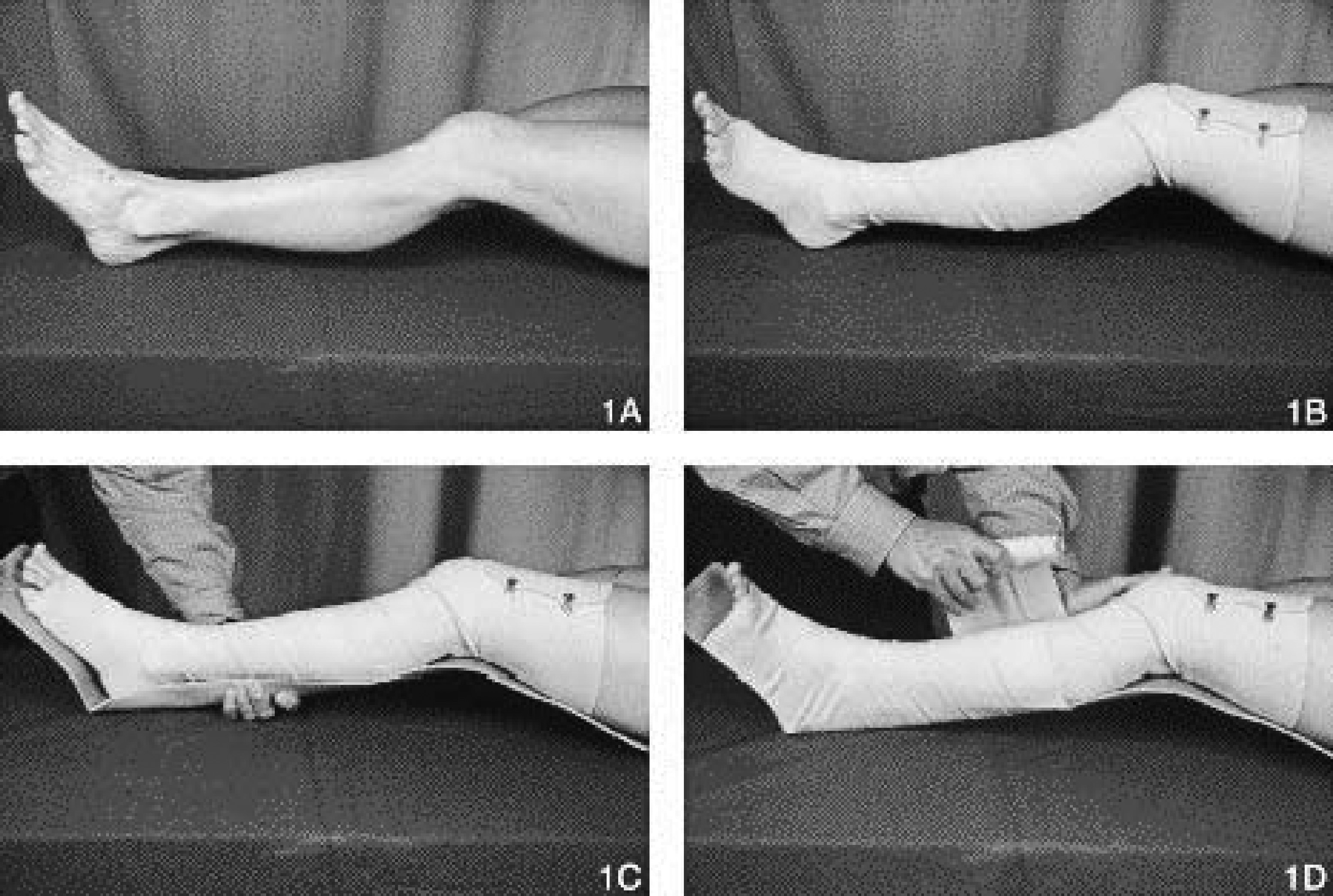
Pressure immobilization of the lower extremity using an elastic wrap and a SAM splint.
Splint
Whether or not PI is to be used, apply a splint to the limb to reduce pain, swelling, and bleeding, and keep the victim at rest as much as possible.
Pain control
Acetaminophen (paracetamol) will give pain relief, but avoid aspirin and anti-inflammatory agents (eg, ibuprofen), which may worsen bleeding.
Fluid management
If transport times are long and an intravenous line is not running, allow the victim to take clear liquids (but no solids) as long as there is no nausea or vomiting.
Logistics
The first responder should obtain expert advice and begin rescue logistics as early as possible by contacting the most appropriate local emergency dispatch center, emergency department, and/or poison center. Most rescues are initiated using modern wireless communications, 1 and mountaineers are encouraged to carry wireless devices appropriate to the region. Mobile cell phones that use code division multiple access (CDMA) technology have greater ranges (up to 70 km) than global system for mobile (GSM) phones (limited to 35 km), and analogue modes give greater range than these CDMA and GSM digital modes. Hand-held programmable radios may be useful in areas with repeater networks that allow emergency access. Satellite phones are the only option in many remote mountain ranges. Intervening obstacles, such as mountains and canyon walls, impair all wireless communications and may render them useless.
Helicopter rescue has become common, 51 although this may require a ground team to first get the victim to a suitable location for slinging or hoisting. Attempting to sling or hoist through trees is hazardous. 5 Helicopter operations are limited by availability, fuel capacity, geography, weather, and visibility.
Rescue team requirements will be influenced by such factors as the need for ground evacuation and first aid and medical management on scene and during transport. Rescue breathing may be required for many hours or even days when evacuation is delayed, especially after serious neurotoxic elapid envenomation. 37
Eye exposure to spitting cobra venom
Irrigate the eyes extensively with water or saline for 15 to 20 minutes.52,53
Transport
Transport should not be significantly delayed by any first-aid measure.
Advanced Medical Treatment
This section is intended for qualified clinicians and presumes that all appropriate measures in the first-aid section have been instituted.
Baseline physical examination
The physical examination should be targeted and brief with special attention to the bite area, as well as the cardiovascular, pulmonary, and neurological systems to obtain a baseline assessment.
Monitoring
Monitor vital signs, key physical findings (eg, soft-tissue swelling, evidence of neurotoxicity), and cardiac rhythm and oximetry when available.
Intravenous access
Ideally, at least 2, large-bore intravenous lines should be started to provide access for fluid and antivenom administration as needed. In a mountain wilderness setting, it is not unusual for victims to be somewhat volume depleted from physical activity and reduced fluid intake. This can compound venom-induced hypotension. It is, therefore, prudent to provide hydration to the victim prior to or during transport as long as there is no contraindication to doing so. If hypotension occurs, the victim should receive intravenous physiologic crystalloid resuscitation (20 mL per kg, repeated as necessary). Intraosseous access is an alternative if the victim is in shock and an intravenous line cannot be established. Fluids administered through an intraosseous line may need to be given under pressure. A blood pressure cuff can be wrapped around the fluid bag and inflated to a pressure that achieves an adequate flow rate.
Oxygen
Oxygen should be administered according to the clinical condition and availability.
Analgesia
Local pain may be severe, especially after most viperid and some elapid bites, and may require parenteral opiates. Alternatively, ketamine has been advocated for analgesia in wilderness settings 54 and for mountain rescue, 55 although its use has not been studied in snakebites.
Advanced life support interventions
Early collapse after a snakebite (within minutes) could be due to venom toxicity or an anaphylactic or anaphylactoid reaction. Such patients should be managed with intravenous fluid boluses, intramuscular epinephrine (0.01 mL/kg of 1:1000 solution up to 0.5 mL), antihistamines, and steroids, 56 in addition to antivenom, as soon as possible 18 (see later). Intramuscular injections should be avoided in a coagulopathic patient if possible, but, if necessary, concentrated direct pressure should be applied to the site to prevent hematoma formation. Alternatively, if cardiovascular collapse is severe, epinephrine may be administered cautiously intravenously according to advanced life support guidelines for anaphylaxis. 56 Likewise, cardiac dysrhythmias should be managed according to advanced life support guidelines. 57
Airway intervention
If the patient develops respiratory distress, ventilations may need to be supported using a bag-valve-mask, mouth-to-mask, or mouth-to-mouth technique. Definitive control of the airway is obtained via placement of a cuffed endotracheal tube below the vocal cords, generally via direct laryngoscopy, but this should be done with great care to avoid traumatizing the airway and causing additional bleeding and swelling. The use of sedating and paralytic agents (rapid sequence intubation) may be needed. If, however, it is predicted that securing the airway will be difficult, it may be best to perform intubation under direct visualization with the patient lightly sedated but not paralyzed (ie, awake intubation). In the wilderness setting, if airway equipment is very limited, the availability of an endotracheal tube and stylet may allow securing the airway of an apneic victim by the digital or tactile technique. As a last resort, if the need for a secured airway exists and the patient cannot be intubated from above the cords, a surgical airway (cricothyrotomy) is needed, although this can be especially challenging if the victim is coagulopathic. In bites to the head or neck, as might occur in a person climbing up a rock face, airway management should be considered early, before severe edema and coagulopathy develop.
Antivenoms
All currently available snake antivenoms are heterologous serums produced by injecting laboratory animals (generally horses or sheep) with the venoms of snakes for which the product is intended. Antivenoms are relatively specific for the venoms for which they are protective, and there is little to no cross-protection against venoms of unrelated snakes. All heterologous serums carry a risk of inducing acute adverse reactions, typically anaphylactic or anaphylactoid in nature, or delayed serum sickness.
Field administration of antivenom
The decision as to whether or not to carry antivenom on wilderness excursions must be made based on several factors. These include the risk of snakebite (based on snake population densities and the practicality of preventive measures), the logistics related to evacuation (transportation availability, access to definitive care, etc), the availability of equipment and expertise to administer antivenom and deal with potential complications, and the financial resources of the team. In well-equipped and adequately staffed expeditions to remote regions, having antivenom immediately available might prove beneficial, because the sooner antivenom is given after a significant bite, the more effective it will be. 58 In elapid envenomations, for example, neurotoxicity, once established, may not be reversible with antivenom and the consequences, including respiratory failure, may persist for weeks. Administering antivenom in such bites at the earliest sign of toxicity may prevent the need for prolonged intubation and mechanical ventilation. 5 Although the ability of antivenom to prevent local tissue damage after necrotizing bites is suspect, any benefit of the antiserum in this regard is clearly dependent on getting it on board within the first hour after the bite, 58 a requirement that can only be met if antivenom is available in the field.
Likewise, a qualified rescue team may consider carrying antivenom to a snakebite victim in the field in circumstances in which rescue may be prolonged, if the bite appears severe, and if snake identification allows the appropriate choice of antivenom. 5 Field transport of antivenom must always ensure appropriate storage conditions, as detailed in the manufacturer's product insert.
Depending on the quality of the product used, acute anaphylactic or anaphylactoid reactions may develop in 5 to 80% of patients given antivenom. 38 Field antivenom therapy should, therefore, only be contemplated when a qualified clinician is on scene and when all equipment and drugs are available to manage an anaphylactic or anaphylactoid reaction (ie, definitive airway drugs and equipment, intravenous supplies, epinephrine, antihistamines, and corticosteroids). 3
Antivenom administration should generally proceed according to the manufacturer's product insert, which may need to be translated into the physician's native language before embarking on an expedition or rescue. The insert provides information regarding the species covered by the product and dosage recommendations. It may be prudent, whenever possible, to confirm recommended dosing and redosing intervals with a physician knowledgeable about the use of the chosen antiserum, because antivenom product inserts produced by some manufacturers may contain misleading or erroneous recommendations. 59 Antivenom should only be given intravenously (or intraosseously). The total dose to be given should be placed into an intravenous bag, and the infusion should be started slowly for the first several minutes. If no reaction occurs, the rate is increased to get the total dose in within 1 to 2 hours.
Skin pretesting for potential allergy to antivenom, although occasionally recommended by manufacturers, is unreliable, delays antivenom administration, and should be omitted.3,4
It is possible that acute anaphylactic or anaphylactoid reactions to antivenom will be prevented or blunted by expanding the victim's intravascular volume with crystalloid and by pretreating with standard doses of intravenous antihistamines (H1 and H2 blockers) and, when the risk of reaction is felt to be particularly high, subcutaneous epinephrine. 60 The efficacy of prophylactic antihistamines is controversial. 61 Caution must be used if pretreating with epinephrine in a patient with coagulopathy, because epinephrine-induced hypertension could increase the risk of intracranial hemorrhage.62,63 Whether or not pretreatment is used, these drugs must be immediately available to intervene if an acute reaction occurs.3,56
Anticholinesterase trial for venom-induced neurotoxicity
The anticholinesterase drugs, edrophonium and neostigmine, may reverse the effects of snake venoms with postsynaptic neurotoxins, such as some cobras (eg, Naja sp) and Australian death adders (Acanthophis sp). 64 –66 It is reasonable to administer a test dose of an anticholinesterase drug in any victim of snakebite who is demonstrating clear neurological dysfunction (eg, ptosis). Patients should be pretreated with atropine (adults: 0.5 mg intravenously; children: 0.02 mg/kg body weight; minimum 0.1 mg). After this, edrophonium (0.25 mg/kg intravenously; maximum 10 mg) or neostigmine (0.025–0.08 mg/kg intravenously; maximum 2.5 mg) is given. If after 5 minutes there is clear improvement in neurological function, the patient should receive additional neostigmine at a dose of 0.01 mg/kg, up to 0.5 mg intravenously every 30 minutes as needed until recovery occurs. 64 Atropine should also be redosed periodically as indicated by significant bradycardia, especially with hypotension. Anticholinesterase therapy may reverse neurotoxicity to a degree such that intubation and ventilatory support are not required, making extraction from the mountain much easier. Care must be taken to closely monitor the victim, however, during such therapy and evacuation for any evidence of cholinergic crisis, to ensure that neurotoxicity is not progressing and to prevent aspiration.
Disposition
Any victim clearly bitten by a venomous snake should be immediately evacuated from the field to definitive medical care, regardless of whether or not there are early findings of envenomation. Once definitive care is reached, all victims with clear evidence of venom toxicity must be admitted for at least 24 hours, even if antivenom is not required. In the United States, victims who are asymptomatic for 6 to 8 hours after a pit viper bite can be discharged home with instructions to return if they develop any delayed signs or symptoms. In other regions of the world, even asymptomatic patients should be admitted to hospital for 24 hours of observation, given the potential delay in onset of venom toxicity. 22
Limitations
This article is intended to provide mountaineers, first responders, and rescue clinicians with a working knowledge of snakebite in the mountains. Readers are encouraged to seek more extensive information regarding the indigenous snakes of the regions they will be visiting or in which they provide rescue support and to develop specific management and evacuation plans before they leave on their next trip into the mountains.
Footnotes
Acknowledgments
These recommendations have been discussed and officially approved at the ICAR MEDCOM meetings in Liechtenstein, April 15–17, 2004; in Zakopane, Poland, October 13–17, 2004; and in Paklenica, Croatia, April 12–16, 2004, by the following members of the International Commission for Mountain Emergency Medicine: Hermann Brugger (President) (I), Giancelso Agazzi (I), Borislav Aleraj (HR), Jan Beaufort (CZ), Jeff Boyd (CA), Ramon Chiocconi (corresponding member) (Argentina), Tore Dahlberg (N), Florian Demetz (I), Fidel Elsensohn (Vice President) (A), John Ellerton (GB), Silvia Ferrandis (UIAA MEDCOM) (E), Herbert Forster (D), Hans Jacomet (CH), Sylveriusz Kosinsky (PL), Horia Lapusan (RO), Xavier Ledoux (F), Peter Mair (A), Peter Paal (I), Peter Rheinberger (FL), Günther Sumann (A), Dario Svajda (HR), Michael Swangard (CA), David Syme (GB), Iztok Tomazin (SLO), Urs Wiget (CH), Eveline Winterberger (CH), Gregoire Zen Ruffinen (CH), Igor Zuljan (HR). Both Silvia Ferrandis and Arthur Morgan have represented the UIAA MEDCOM during these meetings and communications and have obtained the assent of the President of the UIAA MEDCOM, Buddha Basnyat, for the Prevention section. Gratitude is additionally expressed to Dr Michael Shuster and Ms Kiera Traversy for assistance with this paper.
*
Official recommendations of the International Commission for Mountain Emergency Medicine and of the Medical Commission of the International Mountaineering and Climbing Federation (ICAR and UIAA MEDCOMS) intended for mountaineers, first responders, paramedics, nurses, and physicians.
**
This article reflects the consensus of opinion of the ICAR and UIAA MEDCOMS, which have full responsibility for the content.
1
None of the authors has any commercial affiliations that might pose a conflict of interest.