
Abstract
Objectives
In India, venomous snakebite remains an enigma. Although ineffective first aid treatments that are centuries old continue to be used by people bitten by snakes, important factual information, such as the importance and uniqueness of bites by the northern saw-scaled viper (Echis sochureki), has been largely lost and forgotten. In this paper, we report the first systematically gathered data on the clinical course of envenoming by E sochureki in Rajasthan, India. Clinical information is reported on 12 victims bitten by definitively identified E sochureki, and 2 clinical cases are described in greater detail to illustrate the severity of envenoming by this snake.
Methods
A data collection form was developed and used to prospectively gather clinical information regarding patients who were bitten by E sochureki and who brought the dead snake with them to hospital. All snakes were definitively identified by an experienced herpetologist. Information on symptoms and signs, management (both first aid and hospital), and outcomes was collected.
Results
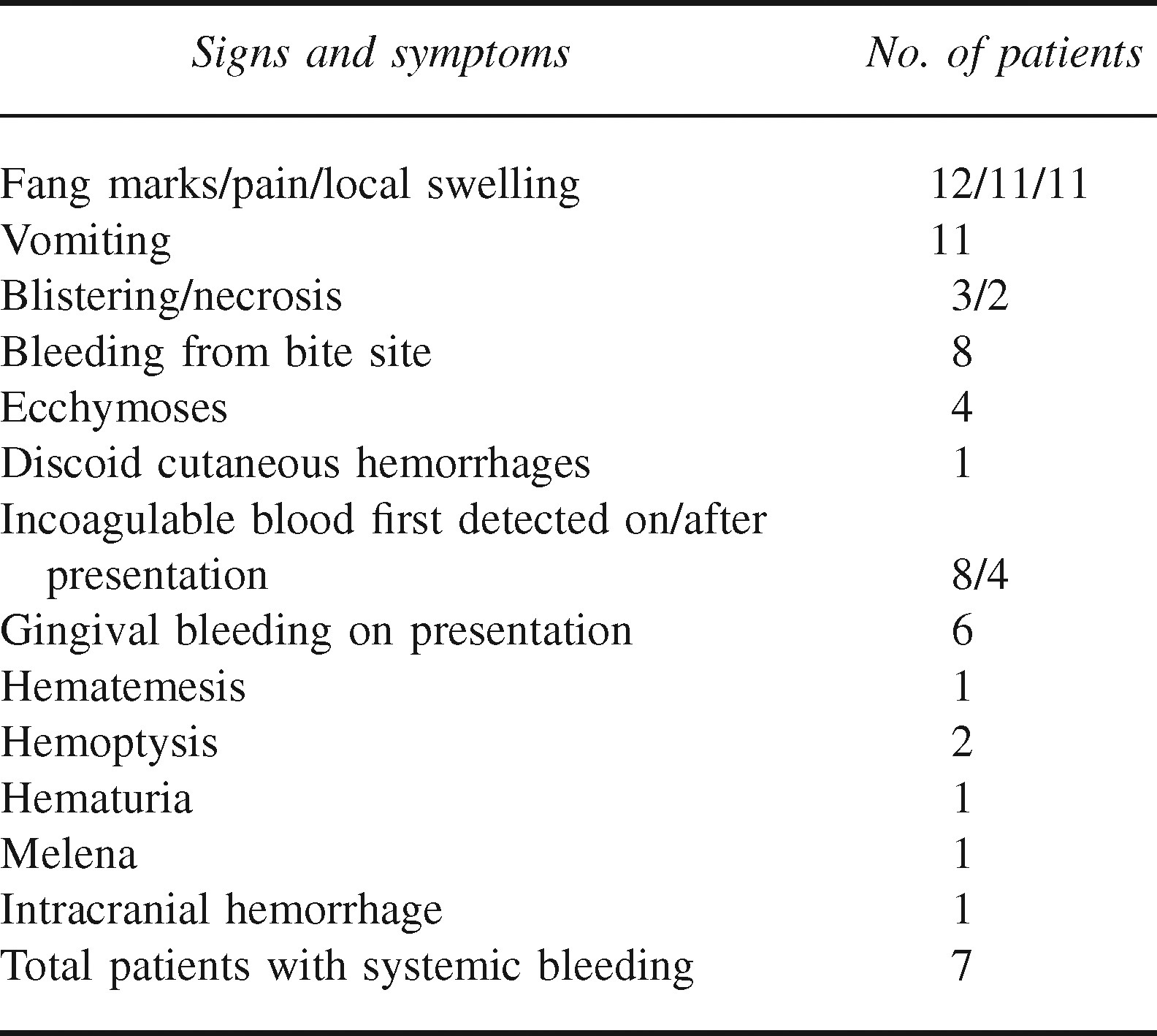
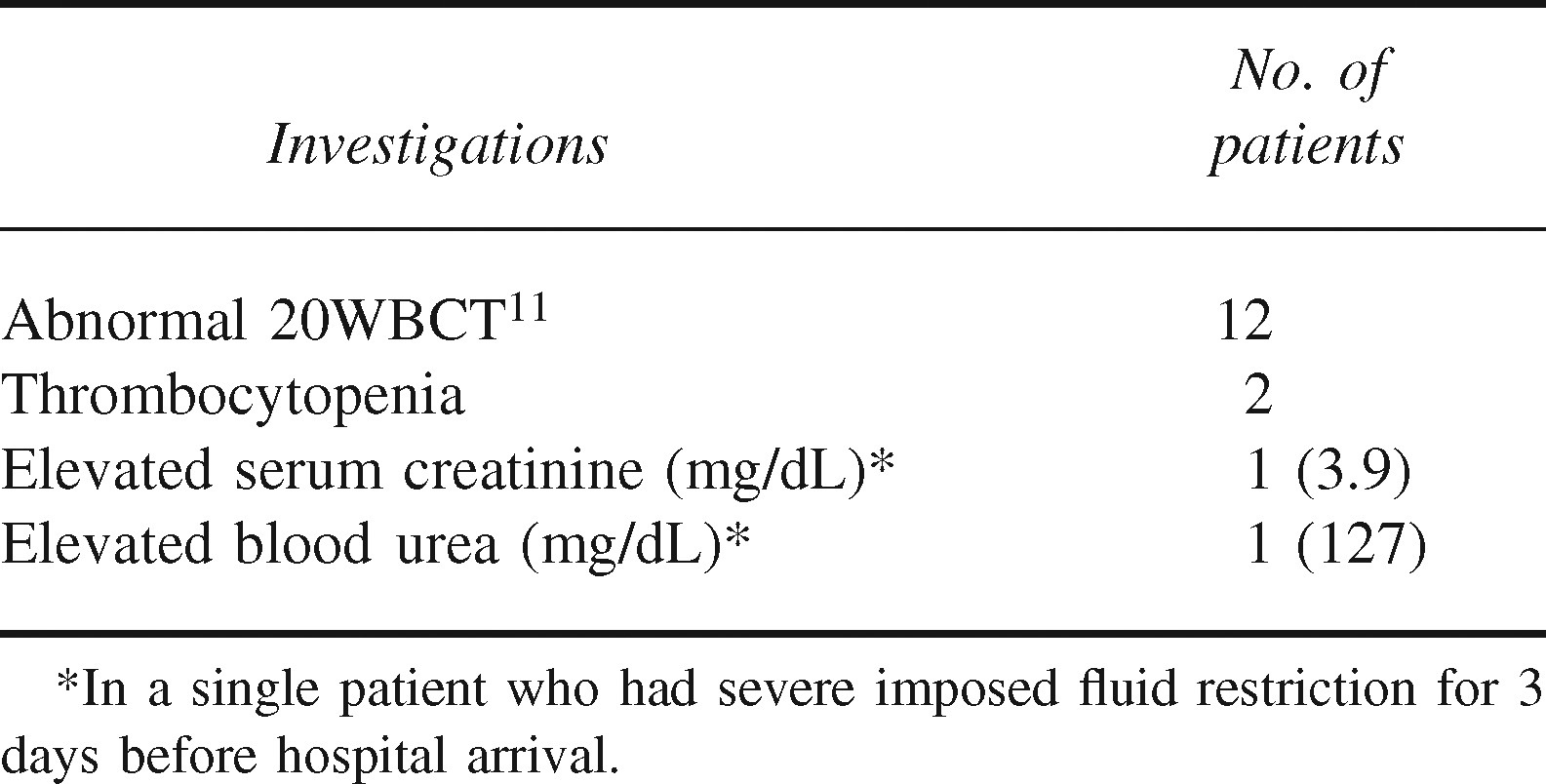
All 12 victims had evidence of systemic envenoming, including abnormal 20-minute whole blood clotting tests (with systemic bleeding in 7). All received polyvalent antivenom made, in part, with Echis carinatus venom from southern India. Antivenom was relatively ineffective in restoring coagulation to these patients. All patients survived, although 1 patient suffered an intracranial bleed with residual hemiparesis.
Conclusions
Echis sochureki causes severe bites in Rajasthan. Work needs to be done to alter the first aid practices used for snakebites in this area, to encourage more rapid presentation to hospital, and to develop antivenom that is more effective against E sochureki.
Introduction
The challenge of snakebite management in India is complex and interesting. India's history of dealing with snakebites dates back many centuries, and the Ayurvedic medical tradition includes snakebite treatments that are many thousands of years old. Many aspects of current popular snakebite management have survived from these periods. The most commonly enduring first aid device is the tourniquet, discussed as early as the 12th century. 1 Correct modern snakebite management, however, must be based on the latest scientific evidence, and those beliefs from the past which have been demonstrated to be ineffective or dangerous need to be abandoned.
One of the great ironies of India, however, is that although ineffective historical treatment methods have been retained, other valuable historical findings have been largely forgotten. In situations such as these, observations and findings that have implications for treatment today have receded into history and become unknown.
This paper examines one such issue and rediscovers the role that one species of Indian snake, the northern saw-scaled viper (Echis sochureki), has had in causing severe envenoming. Historical accounts from the geographic area clearly point to severe envenoming by this snake occurring in the region of modern day northwest India and Pakistan. 2 –4 However, at the time of these reports, only one species of saw-scaled viper was believed to be responsible for bites across the whole geographic range of Africa to peninsular India. Since that time, species reclassification has determined that another distinct species is present in this region. 5 Since reclassification, E sochureki has received almost no attention in the medical literature while the focus has been on the southern species (Echis carinatus). Recent zoological studies have failed to highlight the presence of E sochureki in the Rajasthan area of northwest India.6,7 This has major implications across the northern species’ range, which extends from India to Pakistan, Afghanistan, and Iran. 8 All current Indian polyvalent snake antivenoms (AVs) are prepared with venom from E carinatus and not E sochureki. The efficacy of the current AV must therefore be questionable at best.
In Rajasthan, the traditional tight tourniquet, which is extensively used as an attempt at first aid in the rest of India, is rarely encountered. Instead, the local variant is the use of a peacock feather (“morpunki” in the local Hindi language) tied loosely around the limb. The practice originates from the belief that the peacock is a natural enemy of the snake in the desert and the feather acts to prohibit venom absorption proximal to the feather. In addition, neem (Azadirachta indica) leaves are applied (orally or topically) to counteract the venom, clarified butter or “ghee” is consumed to induce vomiting and expel the venom, and periods of prayer or “Jhadda” are carried out at the local temple. The latter practice is perhaps the most perilous because the prayer can last 3 to 4 days and can seriously delay the patient seeking hospital care.
The S.P. Medical College P.B.M. Hospital in Bikaner, Rajasthan, is a tertiary hospital situated in the Thar Desert in Rajasthan. The college deals with a large number of walk-in patients from the surrounding Districts as well as referral patients. In total, approximately 200 snakebites per annum are treated, mainly in the period June to October. Many of these victims develop quite serious symptoms and signs, which have been previously believed by the medical community to be caused by E carinatus. We, therefore, decided to study the snakebite situation at P.B.M. Hospital. In this paper, we report on systematically gathered data on the clinical course of envenoming by snakes subsequently determined to be E sochureki in 12 patients at P.B.M. Hospital and describe 2 illustrative clinical cases in greater detail.
Methods
Data were gathered at P.B.M. Hospital from September 9, 2006, to October 11, 2006, under the following conditions: A detailed proforma (see Appendix at All consecutive snakebite victims presenting with the dead offending snake were eligible for inclusion in the study. All dead snakes were examined systematically by a herpetologist (I.D.S) with standard keys of morphological characters5,9,10 to establish their identity. Patients bitten by snakes identified as other than E sochureki were excluded. Patients were followed until the time of discharge from hospital. Two senior authors (I.D.S. and D.K.K.) reviewed all study forms for completeness and accuracy. The study received approval from the P.B.M. Hospital administration.
Results
Snake Identification
A total of 12 specimens were brought to P.B.M. Hospital with the patients included in this study. All specimens exhibited all the morphological features detailed by Cherlin 5 as representing E sochureki: ≥32 dorsal scales, ≤187 ventral scales, <39 caudal scales, and regular and even-sized infralabial scales. The specimens were thus confirmed to be E sochureki (Figure 1). The size range of the specimens was 32 to 80 cm, with an average size of 60 cm.

Adult northern saw scaled viper (Echis sochureki) poised to strike in the Thar desert.
Epidemiology
The activity of the victim at the time of the bite fell into 1 of 3 groups: being inside a building or structure (33%), participating in agricultural activity such as millet harvesting or shepherding (25%), and walking to or from an occupational activity to the home (42%).
First Aid Treatment
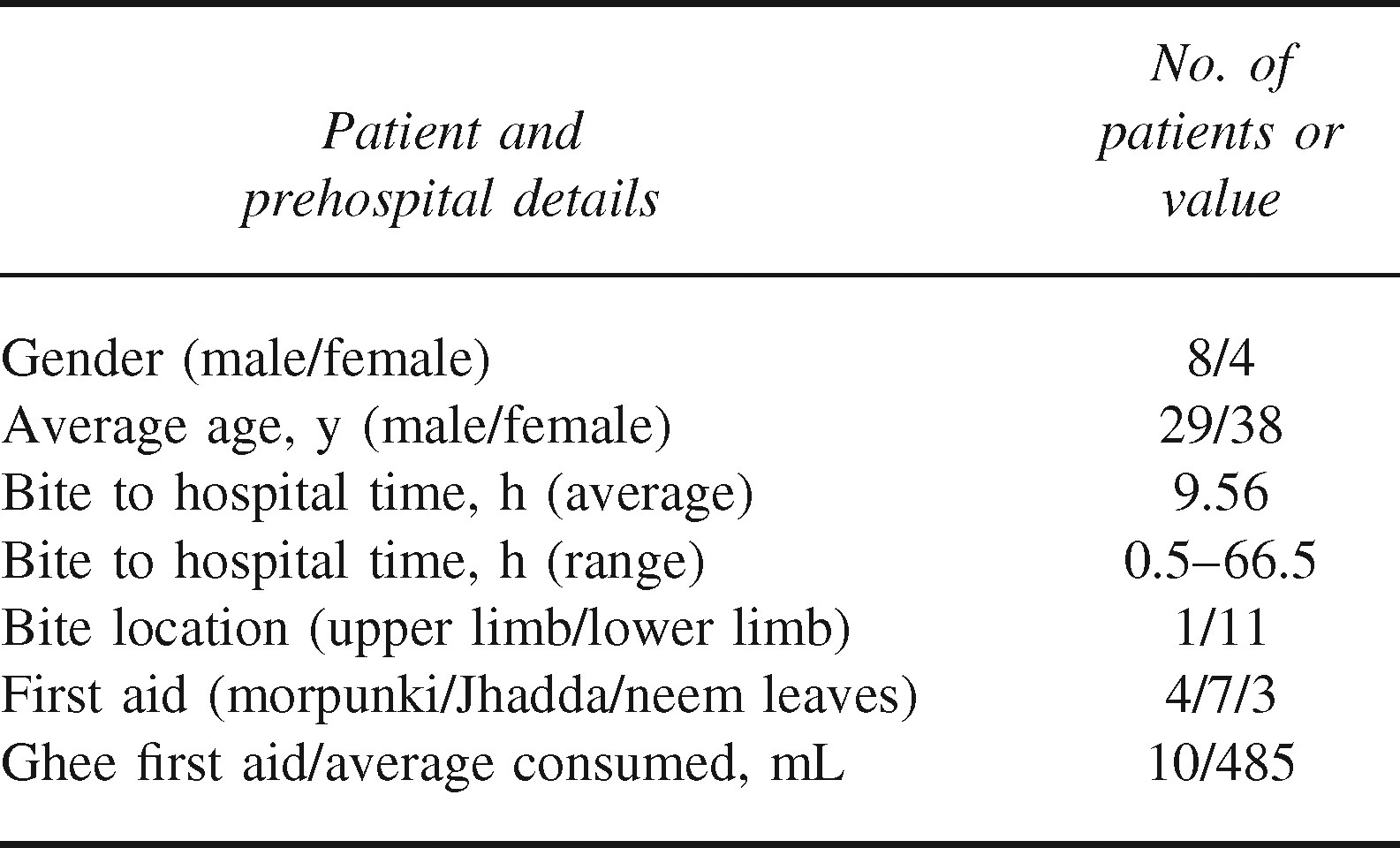
No patients resorted to ill-advised application of tourniquets. Prehospital efforts used by victims to try to reduce the severity of envenoming are listed in Table 1. These included 4 patients who applied morpunki (Figure 2), 7 who spent time in Jhadda, 3 who applied neem leaves, and 10 who ingested ghee.

The use of “morpunki” in a victim of Echis sochureki envenoming. A peacock feather is tied loosely above the bitten foot in the belief that it will prevent venom absorption.
Summary of Clinical Findings
The clinical characteristics of the 12 envenomed patients are described in Tables 1 through 4. The bite to hospital arrival time was highly variable, and was negatively affected primarily by the practice of Jhadda. Of the 8 patients who presented at hospital with incoagulable blood, 7 subsequently showed evidence of systemic bleeding (Table 2). The average bite to hospital arrival time of these patients was 14.5 hours. Excluding the highest value of 66.5 hours, the remaining average arrival time was 6 hours. In the 4 patients who presented with coagulable blood, which subsequently became incoagulable after admission, the average bite to arrival time was 2.5 hours. None of these 4 patients experienced systemic bleeding.
Characteristics and first aid details in 12 patients bitten by Echis sochureki in Rajasthan, India
Signs and symptoms in Echis sochureki envenoming.
Laboratory values following bites by Echis sochureki (20WBCT = 20 Minute Whole Blood Clotting Test).
Treatment details in 12 patients bitten by Echis sochureki.
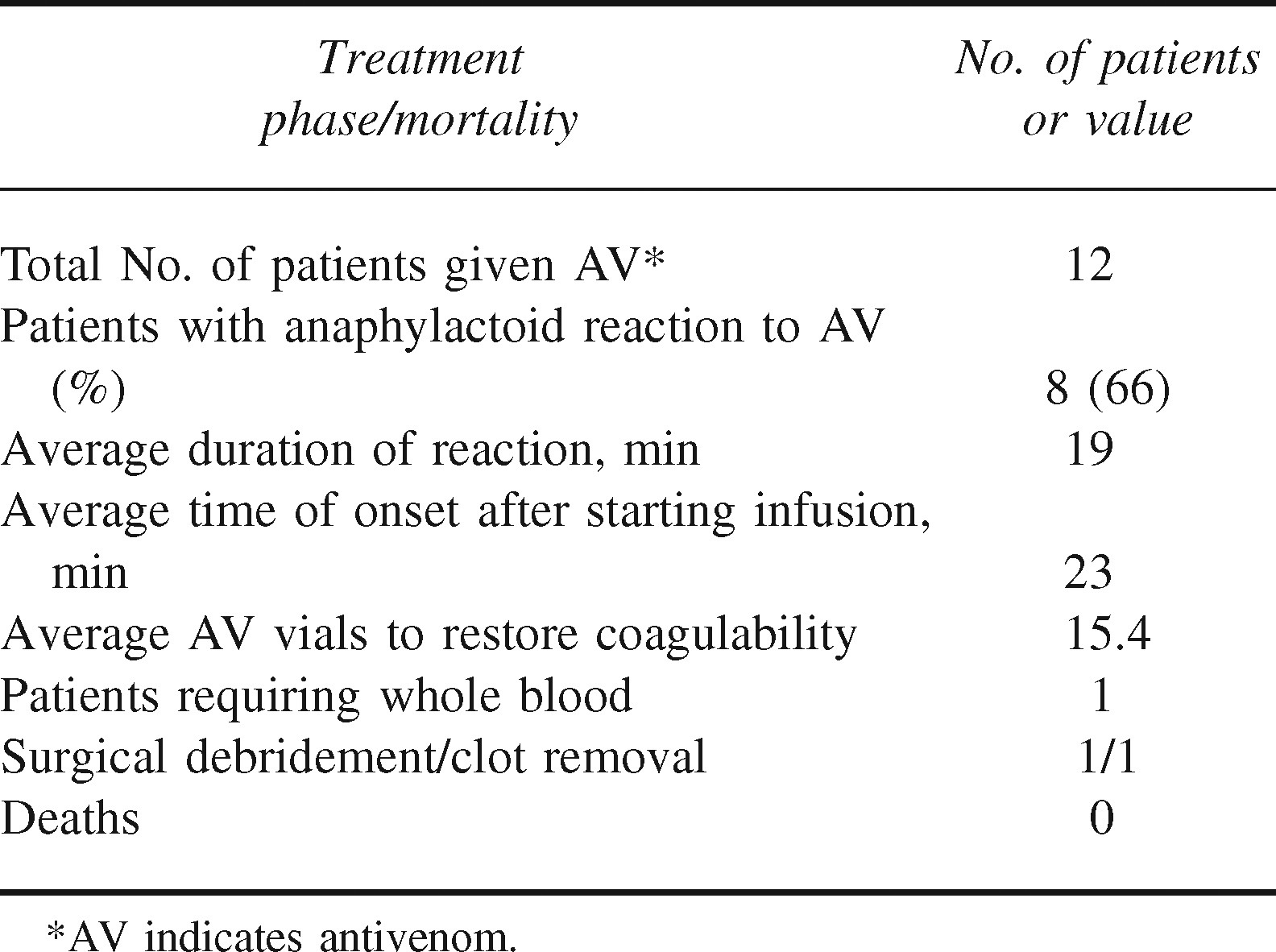
All 12 patients received Bengal Chemicals polyvalent AV, and acute anaphylactoid or anaphylactic reactions occurred in 66% (Table 4). These reactions were typically manifested by acute urticaria and hypotension during AV infusion. The local protocol advocates the early use of intramuscular epinephrine (adrenalin) 0.5 mg 1:1000 at the first signs of a reaction. In 7 of 8 cases, 1 dose of epinephrine reversed the acute reactions. A second dose of epinephrine was required in only 1 case. In 2 cases, acute allergic reactions recurred when AV was restarted after the initial reactions had been reversed, and these were successfully treated with epinephrine as well. No patient developed clinically apparent hematoma formation at the injection site despite the presence of coagulopathy. Because patients were routinely lost to follow up after discharge from hospital, no data are available on the occurrence of delayed serum sickness in this group.
Illustrative Case Reports
Case 1
A 24-year-old female agricultural worker was bitten on the left foot at 0900 hours while harvesting millet, a crop with the grain growing at head height, thus drawing the worker's attention away from the ground where the snakes are most often found. The victim applied morpunki to her midcalf and neem leaves to the bite site and undertook Jhadda for 2 hours at the temple. The victim experienced severe pain at the bite site, and ecchymoses rapidly spread to the midcalf. At 1100 hours, the victim was taken to a local hospital. The offending snake was brought to the hospital and subsequently confirmed to be E sochureki. The patient immediately received 1 vial of polyvalent AV. At 1600 hours, the victim complained of a severe headache, and at 2300 hours, the patient became unconscious and was referred to P.B.M. Hospital. Difficulty in obtaining the funds to hire a vehicle for the 40-km journey resulted in the victim not reaching P.B.M. Hospital until 0730 hours the next morning. On arrival, the patient was unconscious, had a widely dilated right pupil (Figure 3), and complete hemiplegia on the left side of her body. At 0800 hours, because of the ecchymoses and suspected intracranial hemorrhage, 5 additional vials of polyvalent AV were started by continuous infusion. At 0850 hours, during the AV infusion, the patient developed acute urticaria. The AV was temporarily stopped, and 0.5 mg 1:1000 epinephrine was administered into the deltoid muscle. A second dose of epinephrine was given at 0905 hours because her condition had not improved. At 0926 hours, the urticaria had reversed, and the AV infusion was completed. At 1100 hours, a 20-minute whole blood clotting test (20WBCT) 11 showed incoagulable blood. Her blood pressure (BP) at that time was 136/90 mm Hg, with a pulse rate (PR) of 84 beats per minute (bpm) and her hemoglobin (Hb) was 8.0 gm/dL. A computerized tomography scan of her head confirmed the presence of a subdural hematoma. Given the presence of severe intracranial bleeding, at 1120 hours, 10 further vials of polyvalent AV were administered by continuous infusion in an attempt to ensure complete neutralization of venom components. She received no human blood products.

Fixed, dilated right pupil in a 24 year old victim of Echis sochureki envenoming complicated by intracranial hemorrhage (22½ hours following the bite).
Repeat 20WBCT at 1700 hours showed coagulable blood. The patient remained unconscious with a BP of 120/80 mm Hg and PR 80 bpm. A neurosurgery consultation was obtained, and at 1850 hours, 300 mg of intravenous phenytoin sodium was given, followed by 100 mg every 8 hours. Her Hb was 11.6 gm/dL. At 0930 hours the following day, the victim underwent frontotemporal burr hole placement with suction and evacuation of approximately 100 mL of clot. The patient was then transferred to neurosurgery. The patient gradually improved, regaining consciousness on day 18, and was subsequently discharged 20 days after her bite with return of her speech, ability to walk, and moderate residual weakness of the left side of her body.
Case 2
A 65-year-old female agricultural worker was bitten on the left foot at 1530 hours while harvesting watermelon. The snake was subsequently identified at P.B.M. Hospital as E sochureki. The victim experienced severe pain and rapid local swelling to the midcalf. The victim undertook a nightly period of Jhadda for 3 consecutive days. As a result of the relatives’ perception that her condition was not improving, the victim was taken to P.B.M. Hospital, arriving at 0952 hours, approximately 66.5 hours after the bite. The patient was conscious and oriented and complained of shortness of breath. Her BP was 130/70 mm Hg, PR 96 bpm, and respiratory rate 24 breaths per minute. The patient had pale conjunctivae and a very white tongue (Figure 4). She had jugular venous distension and hepatomegally, indicative of congestive heart failure. Extensive ecchymoses were observed 20 cm in diameter on the abdomen (Figure 5) and on the upper and middle sections of the right leg and right upper gluteal region (Figure 6). Three discoid hemorrhages were also present on the right lower leg in the region of the knee. There was significant edema and discoloration of the left foot, with an area of necrosis 10 cm in diameter, and 5 blisters approximately 1 cm in diameter filled with hemorrhagic fluid.



Given her severe anemia on clinical exam, she was given oxygen via nasal cannula. At 1030 hours, a 20WBCT was administered which revealed her blood to be incoagulable. Her Hb was 2.0 gm/dL, platelets 22 × 109/L, serum creatinine (Cr) 3.9 mg/dL, and blood urea nitrogen (BUN) 127 mg/dL. She was oliguric on arrival but had been given only minute quantities of water during the period of Jhadda. Urine output steadily increased as fluids were given. Ten vials of Bengal Chemicals Polyvalent AV were given over 1 hour by continuous infusion. At 1220 hours, 1 unit of whole blood was administered to treat her severe anemia. At 1338 hours, repeat Hb was 2.8 gm/dL, and 5 more vials of polyvalent AV were administered in an attempt to ensure complete neutralization of venom components given her severe anemia. A chest radiograph was normal. At 1430 hours, a second unit of whole blood was given to increase the Hb level, which rose to 3.3 gm/dL. At 2020 hours, a further 20WBCT was carried out, which showed the patient's blood was still incoagulable. Five further vials of polyvalent AV were given. At 0430 hours the following morning, the 20WBCT showed that coagulation had been restored, Hb was 4.0 mg/dL, serum Cr was 2.1 mg/dL, and BUN was 90.9 mg/dL.
She received amoxicillin and clavulinic acid 1.2 gm by mouth 3 times daily as prophylaxis against wound infection. Two days after admission, necrotic tissue was debrided. Popliteal and distal pulses were palpable and symmetrical in both lower extremities throughout her course. Given her abnormal renal function, abdominal sonography was performed to determine whether any renal impairment was present. This showed no abnormal collections of fluid in either pleural space or peritoneal cavity. The right kidney was 10.0 by 4.0 cm and the left 10.2 by 5.4 cm. Both kidneys showed normal echogenic patterns.
The patient was discharged 2 days after her surgical debridement and did well with continued outpatient management.
Discussion
Originally, the saw-scaled or carpet viper was assumed to be a single species, E carinatus, whose range extended from Africa, through the Middle East and Pakistan, down into peninsular India. 11 In 1969, Stemmler 9 classified all populations in Pakistan and a few other places as Echis carinatus sochureki. In 1983, Cherlin 5 established E sochureki, known as “Bandi” in Hindi, as a separate species and restricted E carinatus to peninsular India. There is still doubt as to whether E sochureki merits full taxonomic species status, but the number and severity of its bites clearly make it a highly medically important snake. During the course of this study, a further 27 snakebites were admitted to the hospital without the snakes being brought with the patients. All these patients developed incoagulable blood, and the patients and families identified the offending snake as Bandi, making E sochureki the most likely culprit. Among these additional cases were 2 deaths and many cases of severe bleeding.
Recent findings12,13 have confirmed that there is still much to discover concerning the species that constitute snakes of medical importance in India. In addition to establishing that species previously considered relatively harmless are capable of causing life-threatening envenoming, the reclassification of species such as those in the Echis complex creates the need to review these groups of snakes to evaluate the composition of their venoms, the consequences of their bites, and the effectiveness of currently available AVs. Clinical experience of one of the senior authors of this paper (I.D.S.) gained from treating numerous bites by E carinatus and, now, E sochureki suggests that envenoming by E sochureki is significantly more severe than that typically caused by E carinatus. This observation is not surprising; historical accounts list distinct geographical areas in which more severe envenoming from saw-scaled viper bites was recognized, but this was considered a geographical rather than a species variation. In 1895, Dr Imlach, 14 a civil surgeon in Sind, stated, “By far the greatest majority of cases of serious injury and death have been caused by the bite of this species” (Echis). He went on to add, “It is without exception the most deadly poisonous snake in Sind.” In 1890, Vidal 15 remarked, “In all those districts [eg, Sind and Ratnagiri] where Echis is known to abound, the average mortality from snakebite is markedly high.” The Sind district in modern Pakistan, much of Rajasthan, and parts of Gujarat and Punjab are all located in the Thar Desert region and therefore have similar climatic conditions and fauna. Wall's account of Echis envenoming in India 16 details 3 fatal case studies. It is interesting that all 3 of these bites were recorded in the range of E sochureki, and not a single case was detailed from peninsular India where E carinatus is found.
Echis sochureki is a much larger snake (average length 60 cm) compared with E carinatus (average length 35 cm), 17 which should translate to a larger venom yield for E sochureki. Although this could partially explain the more severe envenoming than typically occurs with E carinatus, further research is needed to analyze E sochureki venom to determine precisely which components are operant. Likewise, research is needed to determine the degree of cross-protection from current Indian AVs. Although the recommended interval for repeating doses of AV to reverse on-going coagulopathy is 6 hours 18 (to allow the liver and bone marrow to replete coagulation components), this presumes an effective AV is being given. The uncertainty regarding the efficacy of current Indian polyvalent AVs in completely neutralizing E sochureki venom led to the decision to give additional AV in a shorter time period in the 2 cases detailed here. Furthermore, in our study, 9 patients required more than 10 vials of polyvalent AV to restore coagulation. This suggests that an excess of 45 mg of unneutralized venom 19 was present in the victims at the commencement of treatment, or it gives further evidence that the current AV is ineffective to some degree in neutralizing E sochureki venom. Although many victims presented late, they still had high residual unneutralized venom, indicating that if the AV is effective, then the level of initial envenomation must have been very high. The average venom yield from E carinatus has been estimated to be 13.68 ± 1.26 mg. 20 Although data are not available on venom yield for E sochureki, its larger size should equate to a higher yield. Given the severity of envenoming by this snake, E sochureki venom perhaps should be added to the mix used in AV production or a different regional polyvalent AV developed for use in northwestern India and Pakistan.
Epidemiology reveals some interesting features. Because of the high surface temperature of the desert environment, the vast majority of the population in the area wear substantial shoes or sandals. This is in contrast with the rest of India, where agricultural workers tend to go barefoot. Bites in the region still occur however, at a significant level. The environmental features of high temperature and lack of irrigation determine that agricultural activity, typically millet, pulses, and watermelon farming, takes place during June to October. The monsoon rain occurs from June to September and harvesting is in October. Farmers often reside many kilometers away from the fields they cultivate because of lack of irrigation. To maximize the available working time in the fields, farmers construct buildings or “Dhanis” that are temporarily occupied during peak agricultural activity. At other times, the structures are left unoccupied. A significant percentage of bites (25%) occur in or around these structures. The Dhanis provide cool, dry habitat for the snakes and are uninhabited for 7 months of the year, offering prime opportunity for snakes to take up residence in the structures. Most bites occur at dawn and dusk when both snakes and people are moving into or out of the Dhanis.
Prehospital management in the region presents some unique challenges. In contrast with the vast majority of India, victims in this area, fortunately, do not employ tight ligatures in an attempt to prevent venom absorption. Nor do patients place great reliance on herbal treatments, apart from neem leaves, which are used occasionally either topically or orally. In addition, Ghee, or clarified butter, has been consumed since the 1850s in quantities up to 1 liter to induce vomiting. 21 The major issue in the Rajasthan region is the use of Jhadda, or prayer. Prayers are offered to a local saint who is believed to be able to reverse the action of the venom. This saint differs between districts and sects. For example, the Bishnoi sect, based around Jodhpur, direct prayers to Jamboji, a 16th century saint and founder of the Bishnoi sect. Educational efforts need to be applied to convince locals to send bitten victims immediately to hospital, while family and friends perform Jhadda.
Available laboratory investigations in rural Indian medical colleges are limited to hemoglobin, platelet count, serum creatinine, blood urea nitrogen, and 20WBCT. If formal clotting factor analysis is desired, these tests must be sent out to a central laboratory, with results taking up to 5 days to return. In this study, 2 patients developed thrombocytopenia, with 1 patient's platelet count falling to 22 × 109/L within 67 hours of the bite. It has been reported that a component of E carinatus venom, echicetin, binds to platelet glycoprotein (GP)Ib and further binds to a plasma protein Mκ(Ig Mκ) and induces platelet agglutination. 22 Echis sochureki venom has been demonstrated to activate prothrombin and protein C. 23
In common with other reviews,11,23 our series found no evidence to suggest that E sochureki venom has any negative effect on renal function, in contrast with Russell's viper (Daboia russelii), which regularly causes acute renal failure. Only the victim in case 2 developed elevated serum creatinine (3.9 mg/dL) and blood urea nitrogen (127 mg/dL). In that case, as part of the Jhadda ritual, she was given only minute quantities of water over the 3-day period in very hot conditions. When adequate quantities of water were given during hospital treatment, her renal function returned rapidly to normal.
Bhat's paper 24 on viperine poisoning in Jammu, India, is the only recent literature concerning Echis envenoming from the region. Although not explicitly stated in the paper, it does include data on E sochureki. Specimens originally described as E carinatus from the area have subsequently been examined in the United Kingdom and determined, in fact, to be E sochureki (D. A. Warrell, electronic mail communication, September 2006). All symptomology and pattern of envenoming data in this paper were combined with Russell's viper (Daboia russelii) bite data and, therefore, do not allow direct comparison with the findings of our report. The incidence of severe envenoming in Bhat's series, 24 however, is remarkably consistent with our findings.
A single further case of a snake handler, bitten by E sochureki in the United States has been reported. 22 Clinical effects included profound coagulopathy and gum bleeding. Haffkein Indian polyvalent AV was of limited efficacy in that case.
To gain more information regarding the terrible toll in human suffering this snake is taking in northern India, a more expansive, prospective study of envenoming by E sochureki is currently underway.
Conclusion
Echis sochureki is a highly medically important snake in Rajasthan, India. It is capable of causing severe envenoming typified by incoagulable blood and potentially severe systemic bleeding in victims. Further work is necessary to elucidate the components of its venom, to inculcate in the local population the appropriate first aid measures to be used following a bite, and to identify or develop a reliable AV to counter the consequences of its venom.
Footnotes
Acknowledgment
The authors express their thanks for the assistance provided by Mr Varad Giri and Mr Ashok Captain in obtaining the historical reviews of E sochureki envenoming from the archives of the Bombay Natural History Society.