
Abstract
Background
India has a high incidence of snakebite-related mortality, making effective snakebite management crucial. This study aimed to explore current practices, challenges, and opportunities for improvement in snakebite management across India.
Methods
A cross-sectional survey was conducted among physicians in India covering aspects such as scope of practice, snake identification, first aid measures, institutional management, and specific management practices for hump-nosed pit viper (Hypnale hypnale) bites. The survey included 37 questions across 5 sections, with data collected via emails, professional networks, and online platforms. Statistical analysis was performed using SPSS Statistics 23 (IBM Corp, Armonk, NY), and manual thematic analysis was applied to open-ended responses.
Results
The survey revealed a discrepancy between physicians’ confidence and accuracy in snake identification, with some still reporting outdated first aid and treatment practices. Despite recognizing the importance of snake species identification, a significant portion of respondents incorrectly identified the snakes. The study highlighted variability in institutional practices for snakebite management, such as administering prophylactic antibiotics and tetanus prophylaxis and monitoring periods for asymptomatic patients. In managing H hypnale viper bites, a demand for specific guidelines and a monovalent antivenom was evident because the current polyvalent antivenom is ineffective for this species.
Conclusions
The survey emphasizes the need for improved training in snake identification, standardized treatment protocols, and the development of region-specific antivenoms. It emphasizes the necessity of updating guidelines to address the unique challenges of snakebite management in India, particularly for species not covered by existing antivenoms.
Keywords
Introduction
Snakebite-related mortality in India is a significant concern because the country holds the unfortunate distinction of being the largest contributor worldwide. 1 Studies have consistently shown that doctors in various regions, including across the globe, have limited knowledge of venomous snakes, first aid, treatment, and prevention and lack confidence in managing snakebite patients.2–4 This knowledge gap is attributed to outdated and inaccurate information in core textbooks in certain regions. 5 Given the geographic diversity of India, it becomes apparent that a uniform approach may not address the issue effectively. Presently, the medical education system lacks a comprehensive, evidence-based snakebite management protocol that healthcare professionals can uniformly adhere to, and we rely on the national and international guidelines.6–10 Despite our belief that we treat snakebites according to contemporary evidence-based practices, the authors hypothesized that, in reality, many practitioners still depend on outdated knowledge.
The survey aimed to understand the scope of practice, snake identification, first aid, institutional management, and hump-nosed pit viper (Hypnale hypnale) bite management practices. The goal was to reveal gaps, challenges, and opportunities for enhancement in snakebite management practices.
Methods
Study Design
This study used a cross-sectional survey design to collect data on the current practices employed by physicians in managing snakebite cases in India. The aim was to gather information from a diverse yet representative sample of physicians from various regions of the country.
Survey Administration And Data Collection
Survey
Disseminated through email, professional networks, and online platforms, the survey consisted of 5 sections encompassing a total of 37 questions with multiple sub-questions totaling 59 data-entry columns (see online Supplemental File). Each page of the survey was dedicated to specific themes, titled as follows: Scope of Practice, Snake Identification, Snakebite First Aid, Snakebite Management in Your Institution, and Hump-Nosed Pit Viper Bite Management. Adaptive questioning targeted the fifth section to physicians with relevant experience, enhancing data relevance.
The survey was kept open for a specific time frame of 3 months. Each participant could answer with only 1 email address, using the “Limit to 1 response” feature provided by Google Forms.
Question Themes
The survey addressed participant information (ie, name, age, institute, and qualification), confidence in snake identification, first aid practices, institutional snakebite management, and opinions on H hypnale bite management.
Snake identification was based on images from a herpetologist (SD) and reviewed by a physician (SVA), considering focus, lighting, angle, visibility, and key identification features for accurate differentiation. Authors displayed 12 regionally relevant species, both venomous (V) and nonvenomous (NV), to measure the ability to identify a snake from images (eg, name [3 questions] or venom nature [2 questions]) by physicians (see online Supplemental File) There were 5 questions on snake identification: 3 single-best-answer questions and 2 multiple-choice questions, each scored 1 point for a correct answer, yielding a maximum score of 5. All confidence questions were captured using a 5-point Likert scale. Descriptive statistics were used to summarize participants’ snake identification scores and confidence levels. Correlations between identification accuracy and confidence levels were analyzed using Pearson's correlation coefficient.
Questionnaire Development, Pretesting, Ethical Considerations, and Incentives
The questionnaire was developed based on an exploratory pre–pilot interview within the investigator pool. A pretest was conducted among 2 general physicians, 2 emergency physicians, and 1 pediatrician and subsequently tested among the investigators to ensure its effectiveness and clarity. Informed consent was sought from all participants. Independent institutional review board and institutional ethics committee approvals were obtained to ensure ethical compliance (IEC No. 93/21/IEC/JMMC&RI). Participation in the survey was purely voluntary.
Sampling Strategy
Although a survey sample size of 400 was initially determined using Slovin's formula estimating the 1.2 million registered physicians in the country with an error tolerance e at 0.05 (ie, 95% confidence level [CI]), we pursued a purposive sampling to ensure inclusion of physicians with expertise in snakebite management, representing diverse perspectives and allowing for in-depth exploration of specific aspects such as H hypnale bites. The sample population consisted of physicians managing snakebites, including emergency physicians, general physicians, pediatricians, and intensivists. All physicians involved in managing snakebite were eligible to participate. Duplicate entries were excluded.
Statistical Methods
Descriptive and inferential statistical analyses were performed on the collected survey data using SPSS Statistics 23 (IBM Corp, Armonk, NY). Manual thematic analysis of the open-ended questions were done.
Addressing Nonresponse Error
To mitigate the potential issue of nonresponse, we implemented a series of reminder notifications. These reminders were sent to individuals who had initially agreed to participate in the survey but had not yet completed it. Additionally, 2 reminder notifications were sent to all recipients of the survey distributed by a research assistant (CD).
Missing Data
In cases where a knowledge questionnaire including snake identification was skipped, it was given a response of “I do not know” to ensure completeness of data analysis. All the rest of the missing data were analyzed as is. All other variables were a required question for the final submission of response.
Results
Participant Response Rate
Of the estimated 400 surveys that were distributed online, 64 participants responded, resulting in an approximate response rate of 16%.
Demographic Information And Frequency Of Snakebite Cases
The study included participants from government hospitals (n=6; 9.4%), government medical colleges (n=11; 17.2%), private hospitals (n=14; 21.9%), and private medical colleges (n=33; 51.6%). Participants consisted mostly of practicing clinicians with a postgraduate degree (n=54; 84.4%). Post hoc, we categorized the physicians into 2 groups: Group 1, participants who had a self-reported experience managing >100 snakebite cases (50%), and Group 2, participants with <100 cases (50%). However, the groups were not statistically different in terms of frequency of attending to snakebite cases (P=0.19).
Snake Identification
Regarding snake identification 56.2% of participants (n=35) expressed confidence in accurately identifying snakes. Yet, of these clinicians, 25% misidentified snakes from the images provided. When shown images of nonvenomous snakes for identification, the wolf snake (Lycodon fasciolatus) was identified correctly by 62.5% of respondents, whereas the banded kukri (Oligodon arnensis) was misidentified by 62.4%, although both snakes are members of the family Colubridae. Most participants (85.9%) considered identifying the snake species as important, but 67.2% reported not relying on this for treatment decisions. In distinguishing venomous from nonvenomous snakes, 42% correctly identified all nonvenomous snakes, and 29% correctly identified all venomous species.
The analysis of confidence and identification scores shows that the mean confidence score was 3.4±1 (95% CI, 3–3.8; range, 1–5). The mean identification score was 2.4±1.7 (95% CI, 2–2.8; range, 0–5). Pearson's correlation coefficient between confidence and identification scores was (r=0.44), indicating a moderate positive relationship.
Snakebite First Aid Measures
Participants’ opinions varied on first aid measures. Regarding cleaning the bite with soap and water, 29.7% advised against it. A substantial majority (96.9%) discouraged making an incision and trying to squeeze out the blood. Regarding the use of a tourniquet, 68.8% (44 of 64) believed that it should not be used, with 64% considering it completely irrelevant. However, bandaging the bitten limb was seen as highly relevant by 56.3% (36 of 64), and similarly, 56.3% (36 of 64) considered it necessary to position the bitten part below heart level.
A significant majority in both groups deemed making an incision and squeezing out the blood inappropriate (Group 1, 59.4%; Group 2, 40.6%; P=0.318). Responses varied on the relevance of washing the bite area, with no clear majority, indicating mixed opinions (P=0.122). Tourniquet application was widely discouraged, especially among more experienced individuals (Group 2, 68.8%; P=0.544). Bandage immobilization was supported by a large majority in the more experienced group (Group 2, 71.9%; P=0.178), as was positioning the bitten part below the heart level (Group 2, 56.3%; P=0.178). Across all questions, the P values (>0.05) suggest no statistically significant differences between the groups’ responses, indicating that experience level in snakebite treatment did not significantly influence the preferred first aid measures
Institutional Snakebite Management Practices
When the patient arrives, most participants (81.3%) would clean any locally applied medicine or herbs.
The administration of prophylactic antibiotics for contaminated or deep wounds was common (84.4%), as was tetanus prophylaxis (85.9%). One in 10 participants (n=7; 10.9%) reported that they would administer prophylactic antibiotics irrespective of the wound status for all snakebites.
Duration of monitoring asymptomatic patients for signs of envenomation varied across institutes, with 46.9% opting for a 24- to 48-h observation period and 45.3% opting for a 12- to 24-h observational period. It was interesting to note that 23% calculated the duration of observation from the time of hospital admission, whereas 71.9% calculated it from the time of the bite. It also was interesting to note that most (89.1%) conducted some blood tests routinely to detect envenomation, although 10% did not. Unfortunately, no follow-up question was given to assess the participants’ observational strategies. Many different blood-sampling timings were employed among participants, but 54.7% employed coagulation testing at 0 and 30 min, 1 h, the third and sixth hours, and every 6 h thereafter. The routine blood test for assessing coagulation at admission was the 20-min whole-blood clotting test (n=58; 90.6%), followed by determination of the prothrombin time with the international normalized ratio (n=42; 65.6%) and then the activated partial thromboplastin time (n=33; 51.6%), clotting time (n=26; 40.6%), and bleeding time (n=14; 21.9%). Given this general approach, 28.1% of participants indicated that they relied on bedside clotting time or the 20-min whole-blood clotting test alone, whereas 54.7% used a combination of clotting time and 20-min whole-blood clotting test with determination of the prothrombin time with the international normalized ratio and activated partial thromboplastin time. Other tests done at admission included serum creatinine concentration (n=43; 67.2%), hemogram (n=40; 62.5%), and liver function tests (n=15; 23.4%). Twelve respondents reported that the tests varied case by case (n=12; 18.8%), and 2 reported that no routine blood tests were done at admission (n=2; 3.1%).
Regarding antivenom administration, most respondents had an institutional antivenom protocol (59.4%). It was interesting to note that a minority of participants (12.5%) reported that they routinely administer a test dose of antivenom prior to the full dose.
Of those who did administer antivenom, practices varied, including intravenous and intradermal routes; 6 reported administering 1 vial of antivenom intravenously, 1 reported administering 2 vials, and 1 reported intradermal injection as test doses. Routine premedication prior to antivenom administration was reportedly practiced by 40.6% of respondents, and they used hydrocortisone (n=12), followed by antihistamine (n=7) and subcutaneous epinephrine (n=5).
The initial dose of antivenom administered for a hematotoxic snakebite typically was 10 vials (85.9%), but there was no clear consensus on the maximum total dose, with a range from 10 to >30 vials being reported. Seven respondents (10.9%) reported administering >40 vials of antivenom for hematotoxic snakebites, with 4 (6.3%) mentioning that there is no upper limit for the amount of antivenom to be used. Hematotoxic snakebite, for the purpose of this study, was defined based on current World Health Organization (WHO) guidelines. 7
H hypnale Bite Management
An additional section of the questionnaire aimed at assessing H hypnale bite management was answered by 42 respondents. A third of the respondents (n=11; 34.4%) in this section reported managing >10 cases per year. In H hypnale bites, commonly reported manifestations were prolonged coagulopathy (83.3%; n=35), bleeding (73.8%; n=31), local tissue damage (71.4%; n=30), nephrotoxicity (59.5%; n=25), and even death (11.9%; n=5).
When asked whether they would administer the currently available polyvalent antivenom for snakebites when the snake was identified as H hypnale, 42.9% of respondents (n=18) indicated that they would administer the antivenom. They were further questioned about the rationale behind their choice. Among those administering antivenom (n=18), the rationales included relying on a syndromic approach rather than species identification for administration of antivenom (35.7%; n=12), lack of confidence in snake identification (21.4%; n=9), and medicolegal concerns about denying antivenom to patients with signs of envenomation (14.3%; n=6).
Approximately 70% of respondents (n=30) reported using blood products in the management of H hypnale bites, and 81% (n=34) felt the necessity of a monovalent antivenom specifically designed for H hypnale bites. The survey indicated a perceived need for revised guidelines/practices (n=33; 78.6%), but there were only 16 participants who provided open-ended responses to elaborate on their rationale for supporting modifications in H hypnale management practices.
Thematic Analysis Of Open-Ended Responses
The survey indicated a perceived need for revised guidelines/practices (n=33; 78.6%). Sixteen participants provided open-ended responses to elaborate on their rationale for supporting modifications in H hypnale management practices. Manual thematic analysis of these responses revealed 5 prominent themes:
Specific antivenom development. Respondents stressed the need for a tailored monovalent antivenom for H hypnale and the demand for toxin identification via card tests. Guidelines and standardization. A recurrent theme focused on the need to include H hypnale in official guidelines, treating it on par with the “big four” venomous snakes, namely spectacled cobra (Naja naja), common krait (Bungarus caeruleus), Russell's viper (Daboia russelii), and saw-scaled viper (Echis carinatus) (Table 1). Respondents advocated for standardized treatment guidelines and uniform drug administration practices for H hypnale bites, including discussions on the futility of using antivenom. Suggestions were made for further research to establish these protocols. Training and education. Recommendations included training programs for snake identification emphasizing the importance of education in managing H hypnale bites. Focus on rare manifestations and research. Concerns were raised about rare but severe manifestations such as coagulopathy, renal injury, and occasional death in H hypnale bites. Respondents stressed the need for further research, including studying the role of tranexamic acid and developing antivenom against prevalent strains. Questions were raised about the actual rarity of these severe manifestations. Ethical considerations. Respondents emphasized ethical antivenom development, avoiding endangerment of the snake species.
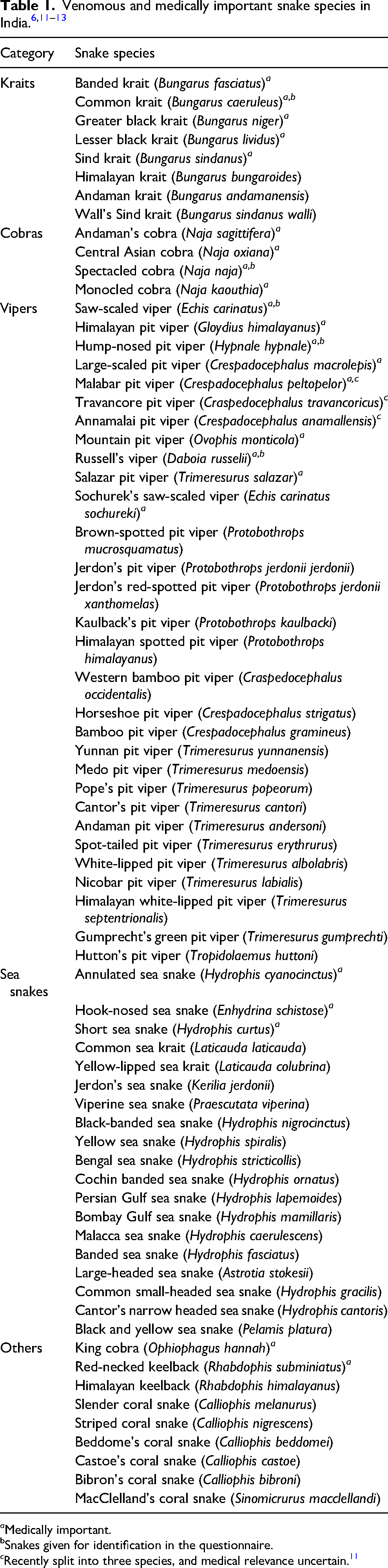
a Medically important.
Snakes given for identification in the questionnaire.
c Recently split into three species, and medical relevance uncertain. 11
Discussion
The survey highlights a varied adherence to snakebite management protocols due to the diversity of medical settings and reveals significant discrepancies in snake identification among physicians across India.
Snakebite Management
In the context of this survey, first aid treatment was defined as actions performed immediately or shortly after a snakebite, before the patient reaches a dispensary or hospital. Respondents were asked about the hypothetical actions they would (or would not) perform if they were present at the patient's side during such time/events. Everyone commonly agreed not to make any local incision and squeeze out blood, as commonly depicted in movies. Washing the wound elicited mixed opinions because it may entail rubbing of the skin, which potentially can accentuate systemic venom absorption and exacerbate local tissue damage. 6
Pressure bandaging and immobilization (PBI) is considered a relevant first aid measure based on the hypothesis that it helps reduce the flow of venom by slowing its spread through the lymphatics.14–16 Positioning the bitten part below the level of the heart, with the rationale of reducing the systemic absorption and spread of venom by decreasing the blood flow from the affected area, is mostly anecdotal and lacks trialed data.6,17 PBI for snakebites is seldom used in actual clinical practice and is not recommended in regions where cytotoxic snakebites (eg, D russellii, N naja, and E carinatus) are more prevalent.18–21 This is possibly not only because PBI potentially aggravates the development of local tissue necrosis in these snakebites but also because it is often poorly done even by trained healthcare professionals, and even if they have been taught the skill.22–24
Healthcare workers in this study did not consider the use of tourniquets a useful first aid, but they reported that tourniquets are widely used especially in regions with prolonged transport times to healthcare facilities. In Myanmar, even with all the research support, the officially promoted application of a pressure pad, bandage, and immobilization as first aid for snakebite was almost never used, whereas most patients used some form of tourniquet (92.0%).25–28 Tourniquet use can lead to significant complications, including limb ischemia, gangrene, and potential amputation, which is why they are generally not recommended.7,29 Current evidence does not support the routine use of tourniquets for snakebites, but some studies suggest that in certain contexts, such as in remote regions with delayed access to healthcare, tourniquets may delay the onset of systemic symptoms by limiting venom spread.25,30,31
However, these findings remain inconclusive, and further research is necessary to fully understand the potential role, if any, of tourniquets in such settings.
Institutional Snakebite Management
Tetanus, Antibiotics
A significant majority of respondents clean the wounds and administer prophylactic antibiotics and tetanus prophylaxis for severe snakebites, with some even prescribing antibiotics regardless of wound status. Although tetanus prophylaxis according to the patient's immunization status is recommended, the role of preemptive antibiotics in snakebites should be reconsidered and warrants further study in India.32–34
Monitoring Period
The guidelines recommend an observation period of at least 24 h for all snakebites.6,8 For those bitten during sleep or unable to recall the time of the bite and in regions where snakes such as H hypnale are known to cause delayed envenomation, extending the observation up to 48 h needs to be evaluated. 35 There was variability in the monitoring period reported for asymptomatic snakebite patients, and a lack of clarity among respondents was evident in determining whether to start the observation from the time of the snakebite or on hospital admission. One notable recommendation for research standardization is to consistently use the time of the bite as the starting point for observation. However, in cases where the time of bite is unknown or not determined, then the time of hospital admission may be taken as the starting point to avoid missing out on envenomation. Participants reported monitoring durations ranging from 12 to 48 h in their practice settings.
Protocols for repeating blood tests varied across institutions. The 20-min whole-blood clotting test or clotting time and prothrombin time with international normalized ratio remain the most common tests used to monitor development of coagulopathy. Specifically, 28.1% of respondents relied solely on bedside methods such as clotting time or 20-min whole-blood clotting test, both of which, though cost-effective, are prone to inaccuracies. 36 In contrast, 54.7% used a combination of bedside and lab tests (eg, prothrombin time, international normalized ratio, and activated partial thromboplastin time), offering more reliable results but at higher costs, especially with coagulation tests repeated over at least 24 h. This highlights the need for economic evaluation studies to create standardized protocols that ensure both cost-efficiency and accuracy in resource-limited settings. It also was interesting to note that some institutes do not routinely use coagulation testing to monitor snakebites. It was intriguing to note a comment that said that they do not give Indian polyvalent antivenom (IPAV) to patients with an abnormal 20-min whole-blood clotting test because their locale did not have any of the big four. In Kerala, even though the big four are present, the second most common bites reported by most centers are H hypnale bites.37,38 D russellii and E carinatus, are not present in the northeast regions of India, like Assam, and thus a prolonged 20-min whole-blood clotting time probably should prompt vigilant observation instead of administering IPAV. 39
Antivenom
Although most institutes follow a protocol for antivenom administration, practices differ in terms of test dosing, premedication, and the dosage range for hematotoxic snakebites, highlighting a lack of consensus on these aspects of snakebite treatment.
Test Dose
One in every 8 respondents (12.5%) reported that they routinely administer a test dose of antivenom prior to the full dose. Skin and conjunctival hypersensitivity tests can only detect IgE-mediated Type I hypersensitivity to equine proteins.40,41 However, most antivenom reactions result from direct dose-related complement activation rather than from non-dose-related IgE-mediated hypersensitivity, making these tests nonpredictive. 42 Because hypersensitivity tests may delay treatment and can be sensitizing themselves, it is advised that they not be done in cases of snakebite envenomation.6–8,43
Dosage
An initial 10 vials of antivenom seems to be the consensus for hematotoxic snakebites, but interestingly, there was no consensus on the maximum dose. The recent National Action Plan for Snakebite envenoming in India suggests a maximum dose of 20 antivenom vials for neurotoxic bites and 30 vials for hematotoxic bites. 6 Unfortunately, the guidelines still do not curtail using higher doses of antivenom in snakebite cases, stating explicitly, “Do not give more than x vials.” The WHO guideline states, “10 vials for patients envenomed by the other species, with repeated dosing if the patient fails to improve, to a maximum of 20 vials.” However, the guideline goes on to mention that there “are no adequately designed dose finding studies that selected snakebites by identified species, controlled for clinical severity,” making clinicians uncertain about their treatment actions. 7 Snakes such as H hypnale lead to deranged coagulation for days to weeks, which is not corrected by the current polyvalent antivenom. The persistence of coagulation abnormalities postbite, especially when the species of snake is unknown, poses a significant dilemma for clinicians. In such scenarios, there is a tendency to administer additional doses of antivenom in an attempt to manage the ongoing coagulopathy, largely because of uncertainty about the optimal treatment approach and the absence of a specific antivenom. Some respondents even suggested that “there's no upper limit” to the amount of antivenom used in their practices. This highlights the unscientific use of IPAV in the community. Even though it is true that the existing antivenom differs in its neutralization capacity even across the big four from different biogeographic zones, and there is uncertainty in the efficacy of the available antivenom, still this does not justify continuing to give antivenom without serving any purpose, especially in the absence of proven systemic bleeding or any improvement of coagulation.6,44 In contrast, it is crucial to emphasize that although maximum-dose guidelines provide some direction, antivenom administration should be individualized based on patient clinical response, especially in patients in whom improvement is noted. Looking for the development of clot lysis or an improvement in clotting time may be considered to be cost-effective strategies to judge improvement in coagulation in patients who initially had completely deranged coagulation parameters. 45
Species Diversity And Antivenom Efficacy In India
There are nearly 310 recognized snake species in India, and even newer ones are being described and older ones reclassified. India is a huge subcontinent with 10 different biogeographic zones, and snakes have evolved here over millenia into diverse species with significant inter- and even intraspecies venom variations. 14 Even with nearly 70 snakes classified as venomous and 23 recognized as causing medically relevant envenomation, the country still relies on a single polyvalent antivenom, the IPAV, which is recognized as the scientifically proven antidote for snakebites in India, targeting the so-called big four snake species. However, studies reveal that current antivenoms fail to neutralize venoms from certain regional populations, particularly in the desert for N naja and in the semiarid north for D russelii and near-complete absence of the big four in certain regions of the country.15,16 This emphasizes the need for geographically efficacious antivenom and highlights the importance of physicians having a comprehensive understanding of the geographic diversity and region-specific venom variations to improve treatment outcomes.
Challenges in the Syndromic Approach
It's crucial to recognize that snakebite syndromes vary geographically and even within species, as seen with D russelii in Kerala and Sri Lanka. The syndromic approach used in one region, such as Sri Lanka, may not be applicable elsewhere. For instance, neurotoxicity in D russelii bites, while significant in Sri Lanka, is less pronounced in India, and the prevalence of D russelii in South India is still uncertain. 46 Additionally, renal failure, a late-stage symptom in hump-nosed pit viper bites, offers limited utility for emergency department physicians to aid in syndromic diagnosis.
Most respondents acknowledged the importance of identifying snake species for managing snakebites in India, with 50% considering it somewhat important and 35.9% very important. However, 67.2% indicated that they do not base their management of snakebites on identifying the snake species. This study's scatter plot of confidence versus snake identification indicated a moderate positive relationship, with higher confidence being associated with better identification accuracy (Figure 1). Despite this positive correlation (r=0.44), the data show significant variability, suggesting that even with high confidence, misidentifications are frequent.
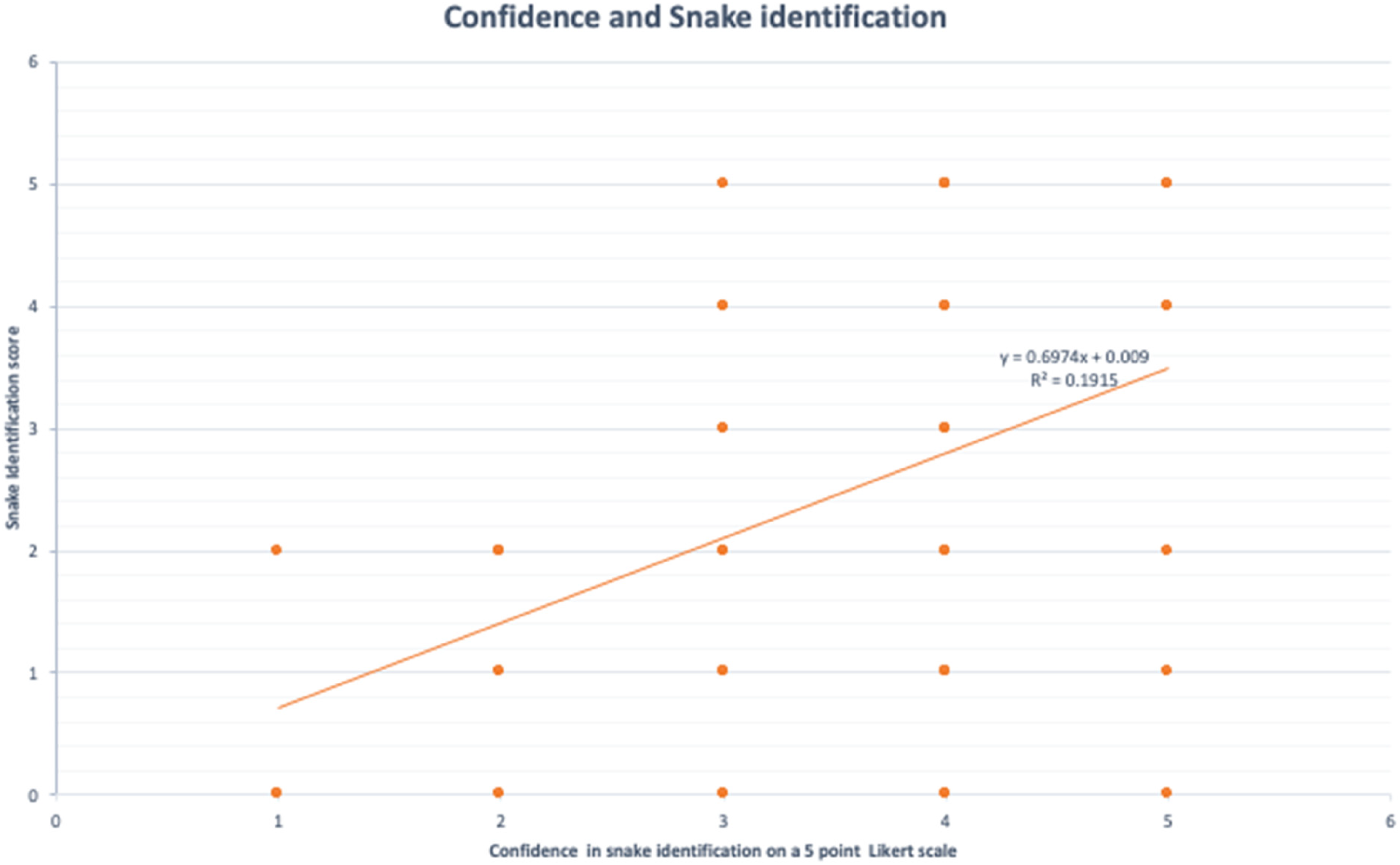
Confidence score versus snake identification score.
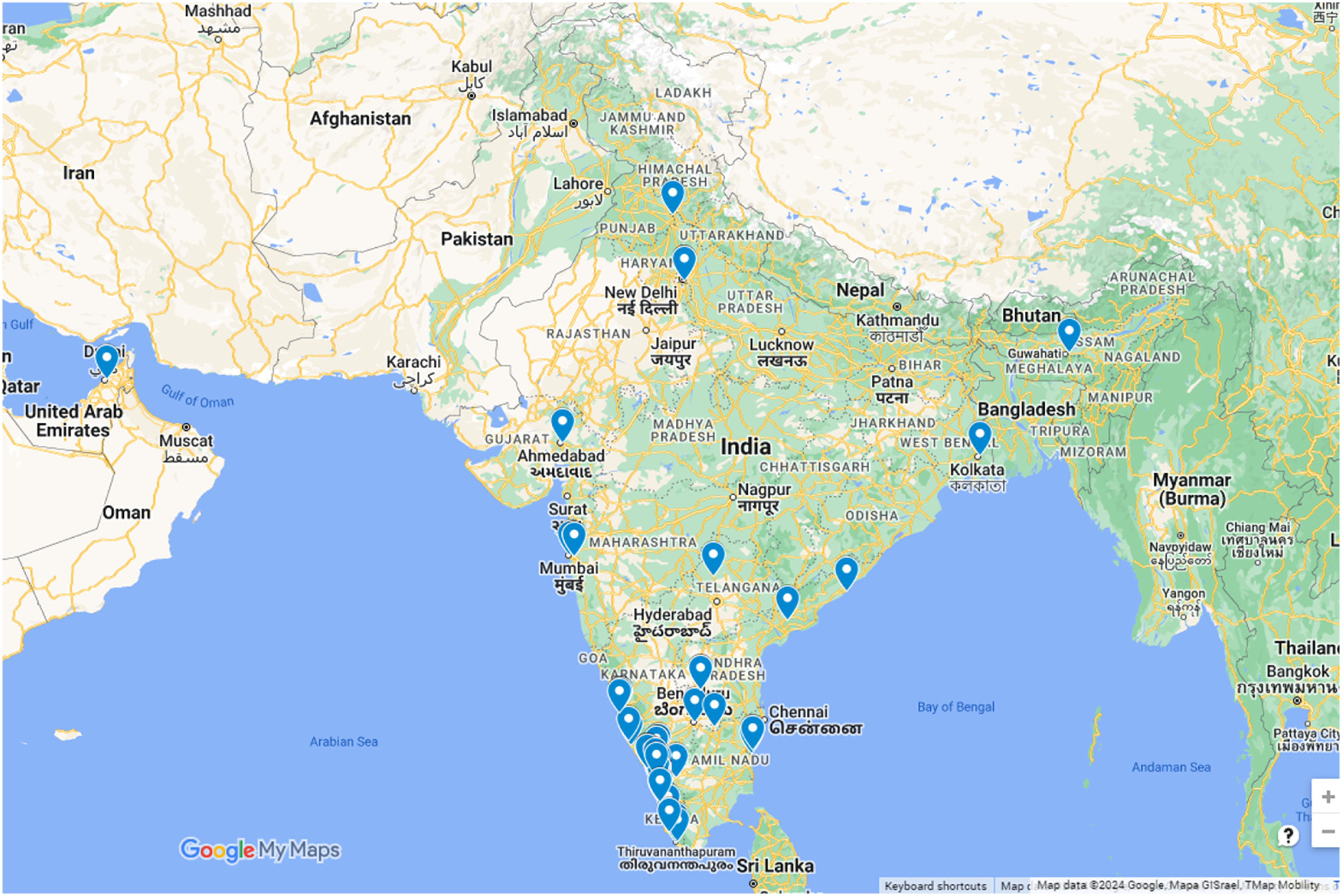
Survey response locations across India. The Google Maps plot illustrates survey response locations from physicians contributing insights on snakebite management practices.
The diverse and often superficially similar nature of snake species makes accurate identification challenging for healthcare workers, biologists, and the general public. Crowdsourcing via online communities and involving skilled herpetologists may enhance the capacity of healthcare workers to identify snakes more quickly and accurately, potentially improving snakebite treatment and outcomes.47,48
Misidentifications of snakes by treating physicians, even when presented with the actual specimen, is well documented.49–53 This discrepancy emphasizes the need for enhanced training programs such as Snake Bite Life Support to bridge this gap. 54 The syndromic classification is more useful in enabling identification of snakebites—that is, determining whether a snake had bitten the victim—rather than identifying the specific species of snake that delivered the bite 55 There should be a balance between overreliance on snake identification leading to unnecessary harm to the snake and humans alike and overreliance on a syndromic approach leading to complete disregard of snake identification. This discrepancy emphasizes the need for improved training and resources in snake identification not only to understand the problem in depth but also to improve clinical management.
Need for a Regionally Tailored Syndromic Approach
In situations where the offending snake is unidentified, a regionally tailored syndromic approach may prove useful. For instance, in regions such as Assam in northeast India, where hemotoxic big four species (ie, D russelli and E carinatus) are rare, a prolonged 20-min whole-blood clotting test may not justify antivenom use. There, antivenom administration could be reserved for neurotoxic manifestations. This exemplifies the need to develop venom detection tools and regional registries and adapt the syndromic approach based on local snake fauna and symptomatology.
Clinical Use in Learning Snake Identification
Physicians often argue that with no monovalent antivenom in the country, it's futile to invest in learning snake identification. However, accurate snake identification aids in effective clinical management, allowing for judicious antivenom use. 51 For instance, it could help avoid unnecessary IPAV treatment in cases where it is ineffective. This approach not only conserves IPAV resources but also reduces the risk of complications from inappropriate use. Additionally, correctly identifying nonvenomous snakebites can shorten hospital stays, reducing healthcare costs, an important consideration in low- and middle-income countries.
Hump-Nosed Pit viper Bite Management
The survey on H hypnale bite management was answered by most physicians (97%) who partook from Kerala and South Karnataka (Figure 2). The prevalence of H hypnale envenomation, especially in the western Ghat region, is often quoted to challenge the traditional big four concept, emphasizing the need for updated snake identification practices and recognizing the importance of other medically relevant snakebites. 56 Review of the literature and surveys of physicians show that it is a medically important snake that not only causes significant morbidity but also mortality.49,57–60 In the management of H hypnale bites, there's a uniformity in the reported need for more specific guidelines and the development of a monovalent antivenom, emphasizing the need for standardized treatment protocols, improved snake identification training, and research into region-specific antivenoms.
The current IPAV is not effective in managing envenomation due to H hypnale, but nearly half the surveyed individuals reported that they administered the current polyvalent antivenom for H hypnale, attributing to reasons such as “relying on the syndromic approach,” “uncertainty in snake identification,” “medicolegal concerns,” and “para-specific neutralization capacity.”60–64 For instance, one comment read as follows: “The current [WHO] guidelines state that the IPAV is only effective against the venoms of the ‘big four’ snake species and caution that polyspecific antivenoms may not cover all medically important snakes, such as H hypnale; however, it does not explicitly state to NOT give antivenom.” Although 1 study demonstrated that Calloselasma rhodostoma (Malayan pit viper) antivenin could cross-neutralize H hypnale venom, all preclinical studies in the region have shown that the current IPAV is ineffective against these pit vipers.37,59,62,65,66 Literature review shows no high-quality studies in the clinical context that have tested its effectiveness in H hypnale bites, but a majority of respondents in the survey reported the futility of IPAV use for blood products and express a desire for a monovalent antivenom specific to H hypnale. The thematic analysis from open-ended responses in the survey reflects a strong demand for updated guidelines and the development of a monovalent antivenom for H hypnale, indicating a critical area for improvement in snakebite management in the region.
Limitations
A limitation of this study is the uneven geographic distribution of respondents, with most being from Kerala. The study on H hypnale bites provided valuable insights into treatment practices in Kerala, but the focus on this region led to critical selection bias, potentially skewing results because other diverse regions in India were not represented. Morphometric variations among snake species and the limited set of 12 species used in the study may affect the accuracy and generalizability of the identification results. The response rate (16%) of the distributed surveys may introduce nonresponse bias because the views and practices of nonrespondents could differ significantly from those of respondents, again affecting external validity. The reasons behind the high nonresponse rate remain unclear. The use of inferential statistics post hoc with a purposive sample in our exploratory study, while aligned with recommendations for nonprobability sampling methods, limits the external validity of our findings, and they should be interpreted with caution. 67 Nevertheless, the problems of understanding and using the existing guidelines, in the our opinion, may be presumed to be the same across India, in the absence of a curriculum-based learning.
Furthermore, we did not ask for specific details on blood test methods (eg, manual, point of care, or automated for prothrombin time/international normalized ratio or activated partial thromboplastin time), treatment protocols, training received, blood product usage, or patient follow-up and continued-care strategies to keep the survey manageable. Although this decision aimed to improve response rates, it limits the granularity of the data collected. The survey was conducted in English, aligning with the medical curriculum, and was initially tested among field experts. This approach assumed familiarity with terms such as splinting and bandaging, but some respondents were unsure about bandage application, with queries about its relation to splinting. The comments reflect a need for clarity in terminology.
Conclusion
The survey exposes significant gaps in snakebite management practices in India, including inaccurate snake identification, inconsistent first aid and treatment protocols, and a need for region-specific guidelines, particularly for regional species such as the hump-nosed pit viper. Despite high confidence, physicians often misidentified snakes, and outdated practices and variability in treatment reveal the urgent need for enhanced training and standardized protocols. Our findings also highlight the need for region-specific training programs, guidelines, and antivenom coverage for medically important snakes not currently addressed by the polyvalent antivenoms to improve snakebite management in India.
Supplemental Material
sj-docx-1-wem-10.1177_10806032241290800 - Supplemental material for Challenges in Snakebite Management in India: Insights from a Physician Survey with Special Focus on Kerala and treatment of bites by Hump-nosed Pit Vipers (Hypnale spp.)
Supplemental material, sj-docx-1-wem-10.1177_10806032241290800 for Challenges in Snakebite Management in India: Insights from a Physician Survey with Special Focus on Kerala and treatment of bites by Hump-nosed Pit Vipers (Hypnale spp.) by Siju V. Abraham, Sarah Paul, Deo Mathew, Punchalil Chathappan Rajeev, Martin V. Paul and Clint Davis in Wilderness & Environmental Medicine
Footnotes
Acknowledgments
The team acknowledges the contribution of HISS investigators (Appu Suseel, C. K. Kassyap, and Aboobacker Mohamed Rafi) and Babu Urumese Palatty, HOD Emergency Medicine at Jubilee Mission Medical College for their critical inputs and review of the manuscript. We also acknowledge the contribution of Sandeep Das in review and the Snakepedia team for providing the images used for snake identification in this study.
Author Contribution(s)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The study was funded in part by the Indian Council for Medical Research Project HISS: Hemostatic Variables in Snakebite Study (ICMR Project No. 5/4/8-21/2021- NCD-11).
Supplemental Material
Supplementary material associated with this article can be found in the online version at https://doi.org/10.1177/10806032241290800.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.