
Abstract
Serum anti-ovarian antibodies (AOAs) have been shown in autoimmune premature ovarian failure and in vitro fertilization-embryo transfer (IVF-ET) cases. The specificity of assays detecting these antibodies has been questioned. Researchers have used several techniques (e.g., ELISA and indirect immunofluorescence). Few have reported on the non-specificity and the type of molecular and cellular targets. We reported earlier on the presence of naturally occurring anti-albumin antibodies as the likely factor for non-specificity. Having developed a novel blocking recipe, we show substantial elimination of this non-specificity. With these standardized tests, we hereby report multiple targets at protein and histological levels. In our study group, 15 of 50 (30%) patients with premature ovarian failure and 13 of 50 (26%) IVF-ET patients showed the presence of AOAs. Western blotting showed a large number of patients making AOAs to a 90-kDa protein, followed by 97- and 120-kDa proteins. Histochemically, it was evident that the sera of these patients predominantly react with the oocyte; other somatic cellular targets are also involved. The specific non-invasive test developed by us was found to be useful because it could carry out a reliable diagnosis of an autoimmune etiology that would be very helpful to select patients in whom immune-modulating therapy could be recommended, which in turn may restore ovarian function and fertility.
Keywords
P
In vitro fertilization-embryo transfer (IVF-ET) has become a promising treatment for infertility with various underlying causes. The presence of serum anti-ovarian antibodies (AOAs) in general circulation of women registered for the IVF-ET program (Gobert et al. 1992; Monnier-Barbarino et al. 2003) has been shown using ELISA and indirect immunofluorescence (IIF). These AOAs do not necessarily appear after follicular aspiration; preexisting AOA levels in some patients show an increase with the number of IVF attempts (Gobert et al. 1992). There is much evidence in the literature indicating autoimmune involvement and its relevance in autoimmune POF (AI-POF) and in IVF-ET. Researchers have shown the presence of antibodies to P450 side-chain cleavage enzyme (SSC), 17-hydroxylase, and 21-hydroxylase in patients with histologically confirmed oophoritis (Winqvist et al. 1993; Bakalov et al. 2005), but these seem to be associated with adrenal autoimmunity (Forges et al. 2004). However, until now, no specific, sensitive, and non-invasive diagnostic test is available for showing the presence of AOAs. The search for AOAs has been undertaken by several investigators, but their results still remain conflicting because of the high rate of false positives (Novosad et al. 2003) and because of different detection methods (Forges et al. 2004). Recent studies from our group clearly indicated that naturally occurring anti-albumin antibodies (NAAs) in the general circulation are responsible for false-positive results in IHC. We developed a simple, sensitive, non-invasive, and specific test using the novel blocking protocol published by our group earlier (Pires et al. 2006). Using this test, we undertook screening of sera from POF and IVF-ET groups for the presence of AOAs. Lack of a specific non-invasive diagnostic test has delayed the characterization of antigenic targets. It is essential to identify the autoantigenic targets to understand the pathogenesis of the disease (Nelson 2001). In autoimmune diseases, involvement of multiple antigens is proposed. It is postulated that autoimmunity can develop in response to a single inciting antigen and spread to involve other antigenic molecules of the same organ (Kaufman et al. 1993).
This study describes specific detection of AOAs along with identification of different molecular and cellular antigenic targets in the ovary. This is important because (1) it will give the clinician a clear idea about the precise AOA status in the patients from both the groups and enable them to plan appropriate treatment strategies; (2) it will help identify antigenic targets that will lead to development of reagents to screen for AOAs that could serve as an analytical tool to detect the disease and consequently design a drug regimen for treatment; (3) it will help in elucidating the mechanism of disease development, progression, and consequent ovarian damage; and (4) it will provide information about the novel proteins in the ovary and also aid in deciphering their role in ovarian biology.
Materials and Methods
Experimental Subjects
This study was performed with prior approval from the Institute's Clinical Ethics Committee.
POF. We screened 50 women with POF for ovarian autoantibodies. The women were referred to the Reproductive Endocrinology and Infertility Clinic at the Institute and at our collaborative centers for a history of secondary amenorrhea. Referring physicians made the diagnosis of POF based on the following criteria: development of amenorrhea (at least 4–6 months) before the onset of 40 years, associated with two serum follicle-stimulating hormone (FSH) levels >40 IU/liter (drawn at least 1 month apart). These women did not have any ovarian and/or any other pelvic surgery (except for a few who had undergone diagnostic laparoscopy). Women with POF as a result of surgery, having a genetic involvement, abnormal karyotypes, radiation/chemotherapy, infections/viral oophoritis, or galactosemia-induced POF were not included in the study. Participants were not on the cyclic estrogen/progestin replacement therapy before our evaluation. All subjects had an average height of 150 cm, well-developed secondary sexual characters, and no dysmorphic clinical symptoms.
IVF-ET. Fifty women registered for the IVF-ET program unable to conceive after 1 year of unprotected intercourse and for whom IVF has been determined to be the next treatment were enrolled in the IVF-ET program. Causes of infertility were tubal, male factors, or idiopathic. Most of these patients were first-time recruits (39/50) into the IVF-ET program; however; those patients with previously unsuccessful IVF (11/50) also were taken for this study. The inclusion criteria for patient selection in the IVF-ET program were (1) <40 years of age at the time of enrollment in the study, (2) having a normal FSH blood level (<10 IU/liter) on day 3 of the menstrual cycle in the past 3 months, (3) having a normal baseline pelvic ultrasound examination in the past 3 months, and (4) having a normal uterine cavity as assessed in the past year by hysterosalpingogram, hysterosonogram, hysteroscopy, or ultrasonography. Patients with the following conditions were excluded from the study: (1) those who had pelvic surgery within the past 8 weeks, including appendicitis or uterine or ovarian surgery, excluding diagnostic laparoscopy; (2) those who had clinical evidence of pelvic inflammatory disease (PID) within the past 3 months and who were treated for any viral infection; (3) those who had severe endometriosis (stage IV); (4) those who had significant abnormalities of the uterine cavity; (5) those who had submucous or intramural fibroids of any size; (6) those who had hydrosalpinx; and (7) those who had polycystic ovary syndrome.
Ten ml of blood was collected by routine venipuncture by well-trained laboratory technicians, and serum was separated. In case of IVF-ET cases, the serum was obtained before ovarian hormonal stimulation. All serum samples were centrifuged, coded, and stored at −20C for further studies. Fifty healthy, normally menstruating, proven fertile women with a median age of 28 years served as controls. They did not have evidence of any autoimmune disease, and they had never presented with any infertility problems. None of the subjects and controls were on any treatment before enrolling in the study. All subjects gave written informed consent for participating in this study.
Animals
Female Holtzman rats (15-20 weeks of age) were housed in a temperature-controlled room with a 12-hr light cycle. The animals were provided food and water ad libitum. All animal care practices and experimental procedures complied with the guidelines of the Care and Prevention Society against Cruelty of Experimental Animals (CPSCEA) on animal care, and the study was approved by the Institutional Animal Ethics Committee.
Isolation of Total Protein
The ovaries were collected from sexually mature, untreated female rats on the day of estrus. The ovaries were washed in chilled 0.01 M PBS, pH 7.4, to remove traces of blood. The tissue was homogenized in distilled water containing 1% SDS (SISCO-SRL; Mumbai, India), 0.2% (3-[3-cholamidopropyl] dimethyl ammonio)-1-propane sulphonate (CHAPS; SISCO-SRL), and a cocktail of protease inhibitors (Roche; Mannheim, Germany) using a polytron homogenizer (Kinematica AG; Luceme, Switzerland). The homogenate was left overnight at 4C and sonicated (Ralsonex; Mumbai, India) the following day for 5 min on ice. The resultant homogenate was centrifuged at 10,000 × g (Eppendorf 5415R; Hamburg, Germany) for 30 min at 4C, and the supernatant was collected, aliquoted, and stored at −20C. The total protein content of the ovaries was estimated by the modified method of Lowry using BSA as the protein standard (Lowry et al. 1951).
SDS-PAGE and Western Blot Analysis
This was carried out as described earlier (Pires et al. 2006). In brief, 40 μg of total rat ovarian (RO) protein was separated on a 10% gel by electrophoresing at 80 V for 3 hr under reducing conditions as described by Laemmli (1970) and electrophoretically transferred to nitrocellulose membranes (Amersham Biosciences; Piscataway, NJ) according to the procedure described by Towbin et al. (1979) using an electroblotting apparatus (BioRad Labs; Richmond, CA) at 80 V for 2 hr. The individual lanes were appropriately marked, isolated, and blocked for 1 hr at room temperature with 5 g% non-fat dry milk in PBS, pH 7.4 (NFDM-PBS). Sera from controls and patients undiluted or diluted to 1:5 with blocking buffer were added to the strip and incubated at 4C overnight. A strip with no primary antibody served as a negative control. The following day, the membrane strips were washed with 0.1% Tween 20 in PBS and incubated with suitably diluted (1:100,000) goat anti-human horseradish peroxidase-labeled secondary antibody (Sigma; St Louis, MO) in 1 g% NFDM-PBS for 1 hr at room temperature. Strips were washed as described above. Detection was done using an enhanced chemiluminescence plus kit (GE Healthcare; Buckinghamshire, UK) as per standard protocol.
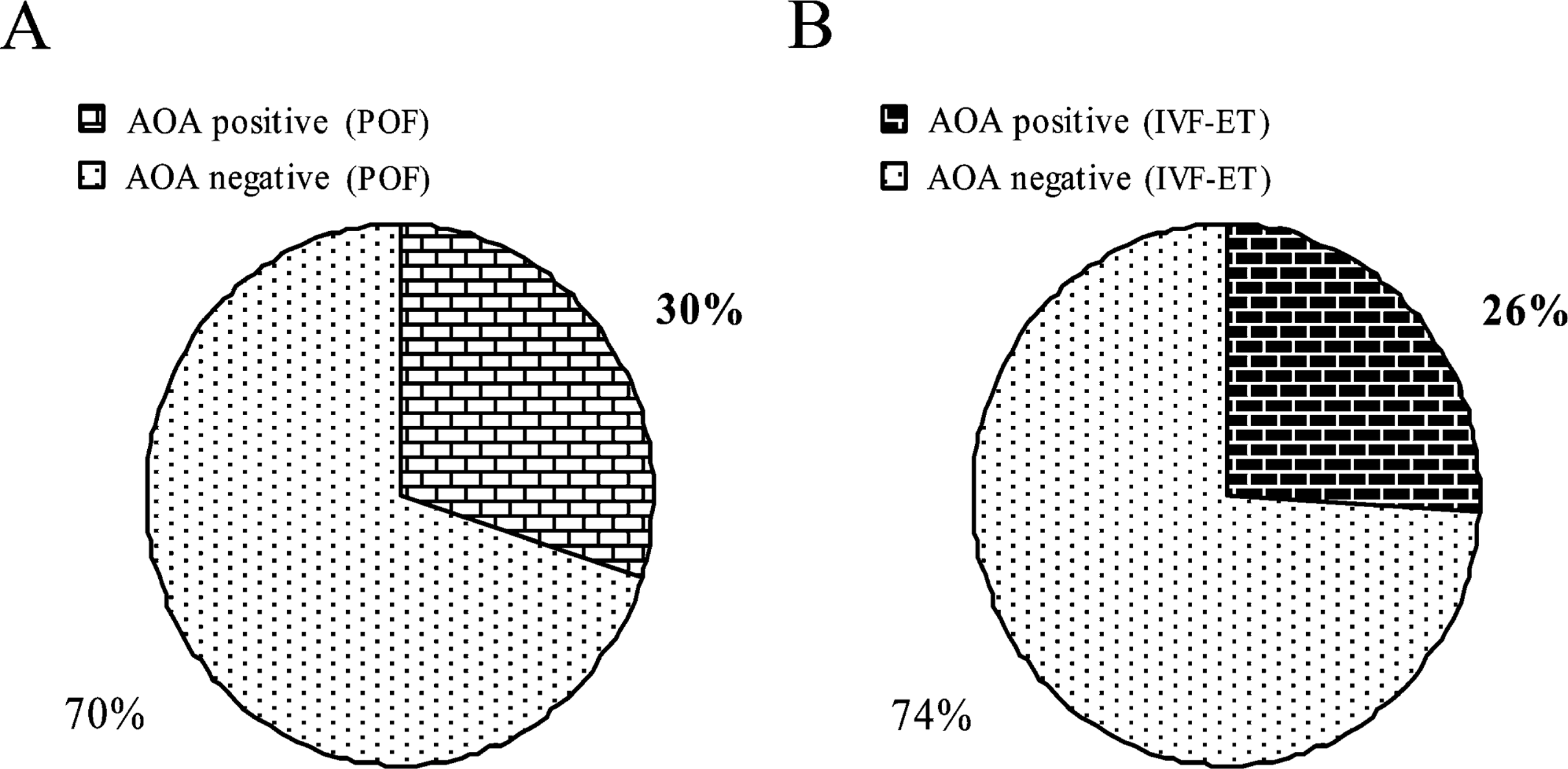
Pie charts depicting the prevalence of serum anti-ovarian antibody (AOA) in patients with premature ovarian failure (POF) and in vitro fertilization-embryo transfer (IVF-ET) patients. Thirty percent (15 of 50) of patients with POFs (
Immunohistochemistry
Rat ovarian tissues and a panel of rat somatic tissues were fixed and processed for IHC as per the protocol described by Pires et al. (2006). Five-μm-thick serial sections were cut on a microtome (Leica RM 2125RT; Leica, Wetzlar, Germany). Only those ovarian sections containing follicles at different stages were taken, so that most stages in folliculogenesis could be viewed at a glance. Paraffin from sections was melted at 56C, deparaffinized in xylene, quenched by endogenous peroxidase activity, and rehydrated. Sections were blocked with NFDM-PBS containing 20% rabbit polyclonal anti-albumin antibodies (AAAs) for 2 hr at room temperature. Sera from control and patients undiluted or diluted to 1:5 with 2.5 g% NFDM-PBS were added on the slide and incubated at 4C overnight in a humid chamber. Sections serving as negative controls were incubated with 2.5 g% NFDM in PBS. The following day, slides were washed with PBS three times, suitably diluted (1:1000) with goat anti-human secondary antibody (Sigma) in 1 g% NFDM in PBS, and incubated for 2 hr at room temperature in a humid chamber. After washing, the immunoperoxidase color reaction was developed using 3,3′-diaminobenzidine substrate chromogen solution (Sigma), counterstained for 30 sec using Delafield's hematoxylin (Qualigens; Mumbai, India), dehydrated through a series of alcohol grades, cleared in xylene, and mounted in DPX mounting medium (SRL; Mumbai, India). Slides were examined on a Zeiss Axioscope microscope (Carl Zeiss; San Marcos, CA).
Results
Prevalence of Ovarian Antibodies
Figure 1 shows a pie chart depicting the prevalence of AOAs in patients with POF and IVF-ET patients. Fifteen of 50 (30%; Figure 1A) and 13 of 50 (26%; Figure 1B) were positive for AOAs by Western blot analysis in the POF and IVF-ET groups, respectively. None of the controls showed the presence of AOAs (p<0.000 in comparison with both test groups; statistical analysis was performed using SPSS software (Chicago, IL) version 11 with Chi-square tests). The Western blot-positive sera were used for immunohistochemical localization of cellular targets.
Multiple Antigenic Targets by Western Blot Analysis
Table 1 shows the molecular targets under immune attack in individual AOA-positive patients. Data from Western blotting are depicted in Figure 2. Figure 2 is a representative picture of various molecular targets. The immunoblotting assay was set up using the sera of POF and IVF-ET-registered patients and from proven fertile women serving as controls. A no primary antibody control showed no immunoreactivity to any of the ovarian proteins, ruling out the contribution of a secondary antibody in the immunoreactivity (Lane NC). Sera from normally menstruating, proven fertile controls showed immunoreactivity only to the 66-kDa albumin moieties (Lane C). However, when sera from the test group were used, multiple antigenic targets were detected. These antigenic targets spanned molecular masses ranging from ∼30 to 150 kDa (Lanes P1-P12). Fifteen of the 50 patients with POF and 13 of the 50 IVF-ET-registered patients that were screened showed the presence of an antibody to the ovarian proteins.
Baseline characteristics of the patients positive for anti-ovarian antibodies in POFs (N1-N7, S1-S3, K1-K5) and the IVF-ET (J1-J13) group showing the molecular and cellular targets
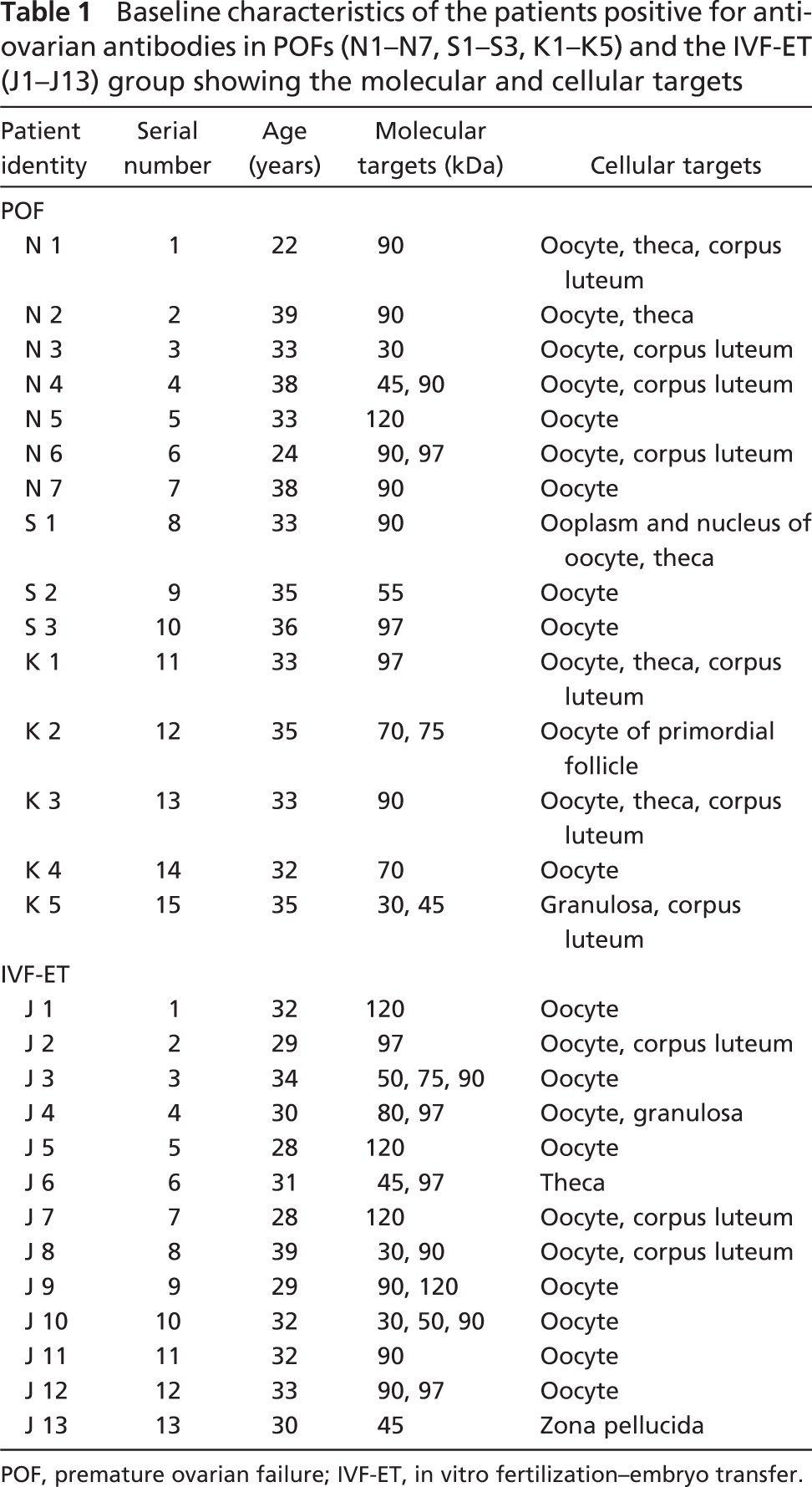
POF, premature ovarian failure; IVF-ET, in vitro fertilization-embryo transfer.
Frequency of Immunodominant Antigenic Targets
Figure 3 depicts the prevalence of immunodominant antigenic targets. The Western blot data clearly indicate the presence of multiple antigenic targets. The sera of these patients reacted to a wide range of proteins spanning the loci between 30 and 150 kDa. From Table 1 it is clear that sera of some patients reacted to more than one protein. A similar phenomenon was noted in the IVF-ET group. Western blot analysis using serum from POF and IVF-ET groups revealed that a 90-kDa protein seems to be the predominant antigenic target. Seven of 15 AOA-positive sera from patients with POF and 6 of 13 AOA-positive sera from the IVF-ET group showed immunoreactivity to this antigen. The next most frequently targeted antigens were 97- and 120-kDa proteins.
True Histological Targets Localized Using the Novel Blocking Protocol
All the Western blot-positive sera from the POF and IVF-ET groups were used for IHC localization. Figure 4 is a representative picture of various cellular targets showing immunoreactivity with these sera. A no primary antibody control showed no immunoreactivity to any of the ovarian cell types (data not shown). As described in the Materials and Methods, the ovarian sections were incubated with the novel blocking reagent developed by us to localize the true antigenic targets in the various compartments of the ovary. The preimmune rabbit sera did not appreciably block background nonspecific immunostaining in rat ovarian sections, whereas sera from the same rabbit postimmunization with human serum albumin were competent in the novel blocking recipe developed by us. Sera from control patients and from patients belonging to both study groups that were found to be AOA negative by Western blot analysis did not show any reactivity to any ovarian target by IHC (Figure 4A). Of the various cellular targets, the majority of the test group patients mounted an immune response to the ooplasm of the oocyte; nevertheless, other cell types were also under immune attack. The oocyte, being the most frequently targeted cell type, showed various degrees of staining intensity from mild to strong. Serum from individual patient responded differently and showed different cellular targets undergoing an immune attack. One clearly sees that multiple cellular targets are under immune attack. As shown in Figure 4, immunoreactivity is seen to ooplasm of the oocytes (Figures 4B, 4C, and 4E-G), cumulus cells (Figures 4C and 4D), granulosa cells (Figures 4D and 4I), zona pellucida (Figure 4J), corpora luteal cells (Figure 4K), interstitial region of the corpora lutea (Figures 4G and 4L), and thecal cells (Figures 4E and 4M). Sera of few patients showed immunoreactivity to all the stages of folliculogenesis right from primordial follicles (Figure 4H) to the antral and matured follicles (Figures 4B and 4C, respectively). Serum of one patient with POF reacted to the nuclear and cytoplasmic compartments of the oocyte (Figure 4E).
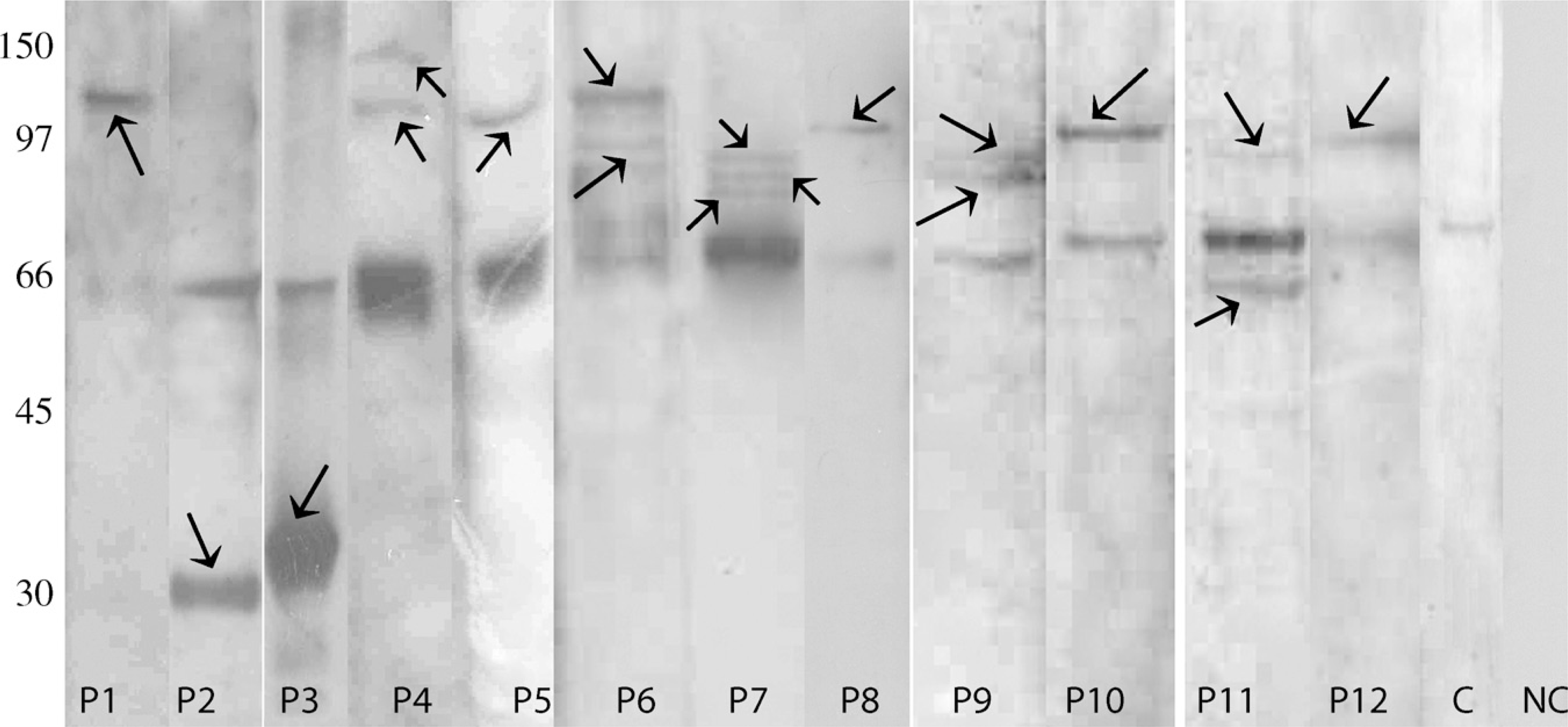
One-dimensional Western blot showing that the involvement of not only a single protein but multiple targets seem to be involved in ovarian autoimmunity. These antigenic targets spanned molecular masses ranging from ∼30 to 150 kDa (indicated by arrows) using sera of different patients with POFs and in IVF-ET patients (Lanes P1-P12). A no primary antibody control (Lane NC) showed no immunoreactivity to any of the ovarian proteins, ruling out contribution of a secondary antibody in the immunoreactivity. Sera from normally menstruating, proven fertile controls showed immunoreactivity only to the 66-kDa albumin moieties (Lane C).
Tissue specificity of these sera was checked using a panel of rat somatic tissues. All AOA-positive sera reacted to the ovary. However, some of the sera showed immunoreactivity to the adrenal and thyroid tissues (Table 2).
Discussion
The endocrine and the immune system work in unison with each other, regulating the functions of the ovary. It is a well-established fact that, in some women with POF, an autoimmune mechanism is involved that is responsible for the loss of ovarian function (Nelson et al. 1996). For most of the autoimmune diseases, screening for specific autoantibodies is probably the best and practical way for evaluating immunological involvement. Several studies have been undertaken; however, the results are conflicting, likely because of methodological differences and multiplicity of immune targets. The source of ovarian tissue has been rat, rabbit, monkey, or human. Although human ovaries would be the ideal choice of source, it is not always possible to get good quality and quantity of the tissue. Even if one was able to have access to the surgical material, very often it does not contain follicles in various stages of folliculogenesis. As a result, the target antigens from this area are likely missed. Results from Wheatcroft and colleagues (1997) called into question the specificity of ovarian antibodies as a marker for autoimmune POF. This group sought to define the prevalence of ovarian autoimmunity using ELISA and IIF and to establish the diagnostic relevance of these two techniques. Western blotting was also used to establish whether there were any discrete autoantigens against which AOAs were directed. Using ELISA, 9 of 30 patients with POF showed the presence of AOAs, and 2 of 30 were positive by IIF using monkey ovarian sections. These two IIF-positive patients did not show AOA positivity using ELISA. It was also not possible to get a well-defined picture of the type of cellular targets involved in these two cases. In Western blotting, two of six patients with idiopathic POF (it was not clear whether these two patients were positive either by ELISA or by IIF) showed immunoreactivity to an 82, 86-kDa doublet protein, which was not reproducible when an ovarian antigen from a different lot was used. The authors attribute this to variations in antigenicity between ovaries procured during different stages of the menstrual cycle. Also, in the study, presumed nonspecific reactivity of the large IgG chain band seen in all patients and controls at the 52- to 63-kDa loci could not be eliminated, despite preincubating protein fractions of IgG with protein A-coated Sepharose beads.
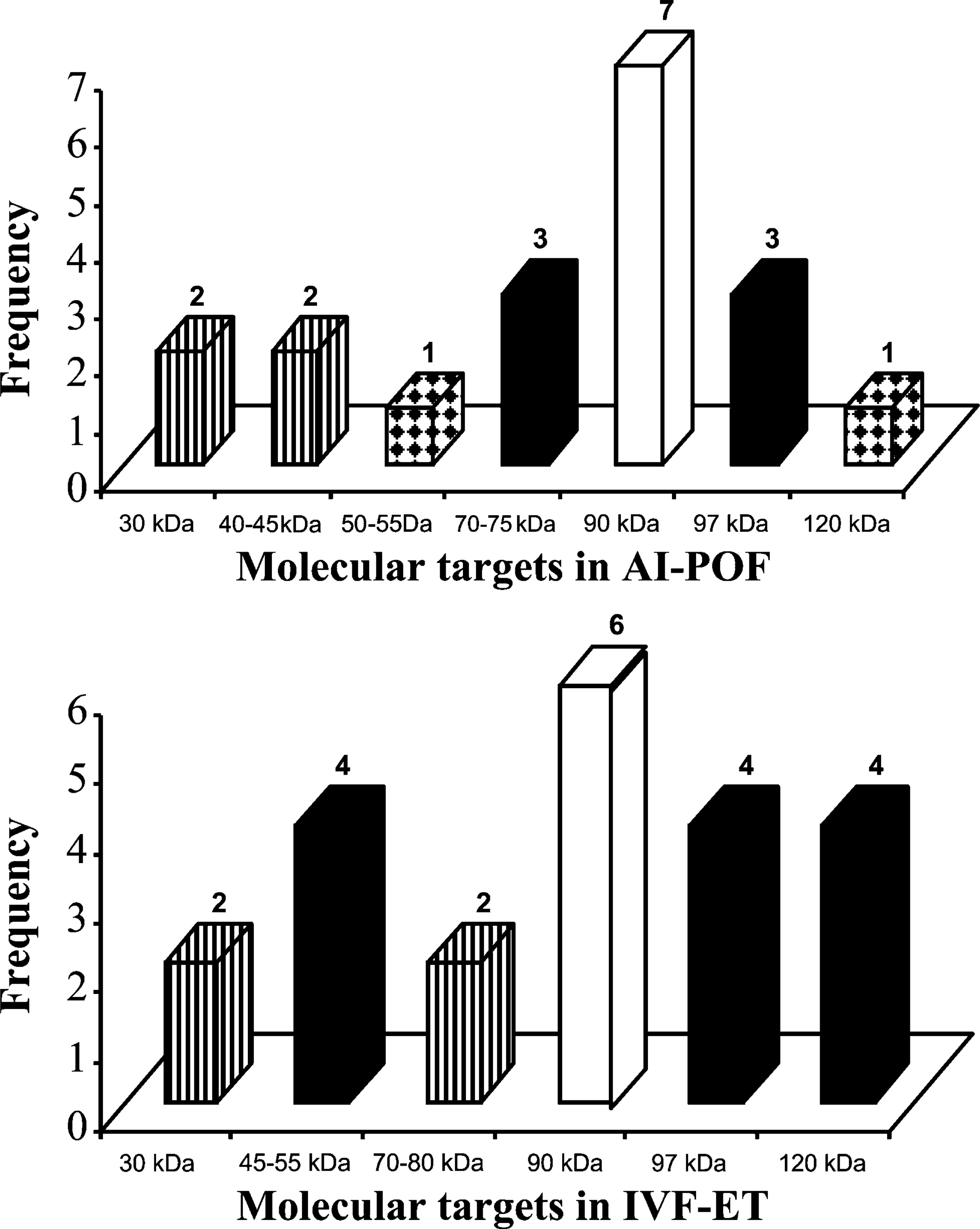
Bar graphs prepared from data of Western blot analysis using serum from patients with POF and IVF-ET patients reveals that a 90-kDa protein seems to be the immunodominant antigenic target. Seven of 15 (46.6%) POF-positive sera (top panel) and 6 of 13 (46.15%) IVF-ET-positive sera (bottom panel) showed immunoreactivity to this antigen.
We systematically studied the cause of non-specificity and succeeded in creating a reliable blocking method to solve this problem (Pires et al. 2006). Results from our laboratory clearly showed that there are specific AOAs in the sera of patients with POF and IVF-ET patients as detected by Western blotting and IHC, which could be involved in ovarian failure, eventually leading to ovarian autoimmunity. From our Western blot data (Figure 2), the antigenic targets span a wide range of molecular mass from 30 to 150 kDa, where 15 of 50 patients with POF (30%) and 13 of 50 IVF-ET cases (26%) were AOA positive. Seven of 15 (46.6%) AOA-positive sera from patients with POF and 6 of 13 (46.1%) AOA-positive sera from IVF-ET patients show immunoreactivity to the 90-kDa protein (Figure 3). No reactivity to any of these targeted proteins using control sera suggests that the identified antigens are specific autoantigens. The ovarian specificity of the multiple antigens identified has been tested using somatic tissues in Western blotting (data not shown). However, some of the patients' sera reacted to adrenal or thyroid antigens in IHC (Table 2). POF is classified as a part of autoimmune polyglandular syndrome, where it is known to be frequently associated with adrenal or thyroid autoimmunity (Kim et al. 1998; Betterle et al. 2002). None of the control sera reacted to any somatic tissue. From Table 1, we can also see that most of the patient's sera reacting to the 90-kDa protein showed immunolocalization to the cytoplasm of the oocyte, with the exception of one patient whose serum also reacted to the nucleoplasm of the oocyte. The majority of the sera reacting with the 120-kDa protein showed oocyte localization, whereas sera targeting the 97-kDa protein showed localization to oocytes and to different compartments of the ovary.
The specificity of our novel diagnostic test has been validated by using internal patient controls that were clinically POF but AOA negative by Western blot analysis. The sera of these women did not show immunoreactivity to any of the cellular targets by IHC. We showed that all patients with POF who were termed Western blot positive showed immunoreactivity to different cellular targets in IHC. This has clearly established the correlation between AOA detected by Western blotting and by IHC and thus diagnostic relevance of the tests. Additionally, when sera were processed for IHC, we ensured that the rat ovaries had been collected on the day of the estrus phase of the ovarian cycle and that sections contained follicles from primordial to Graafian stage. This was possible only because we used rat ovaries. Luborsky and Pong (2000) reported that there is 90% correlation of AOA detection using rat or human ovaries.
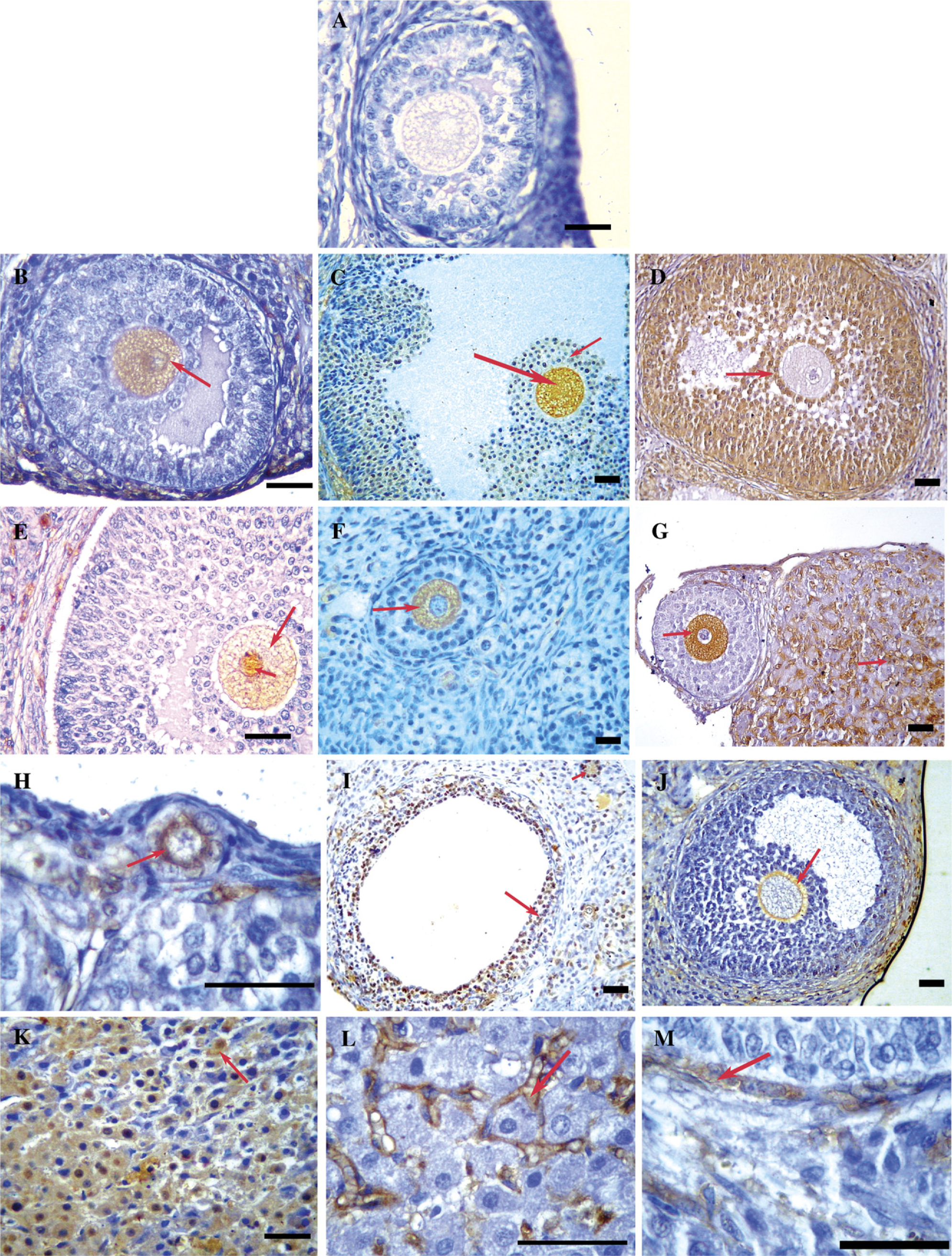
Immunohistochemical localization of serum AOA against 5-μm rat ovarian sections. (
Tissue specificity of the identified antigens using the sera of the test group
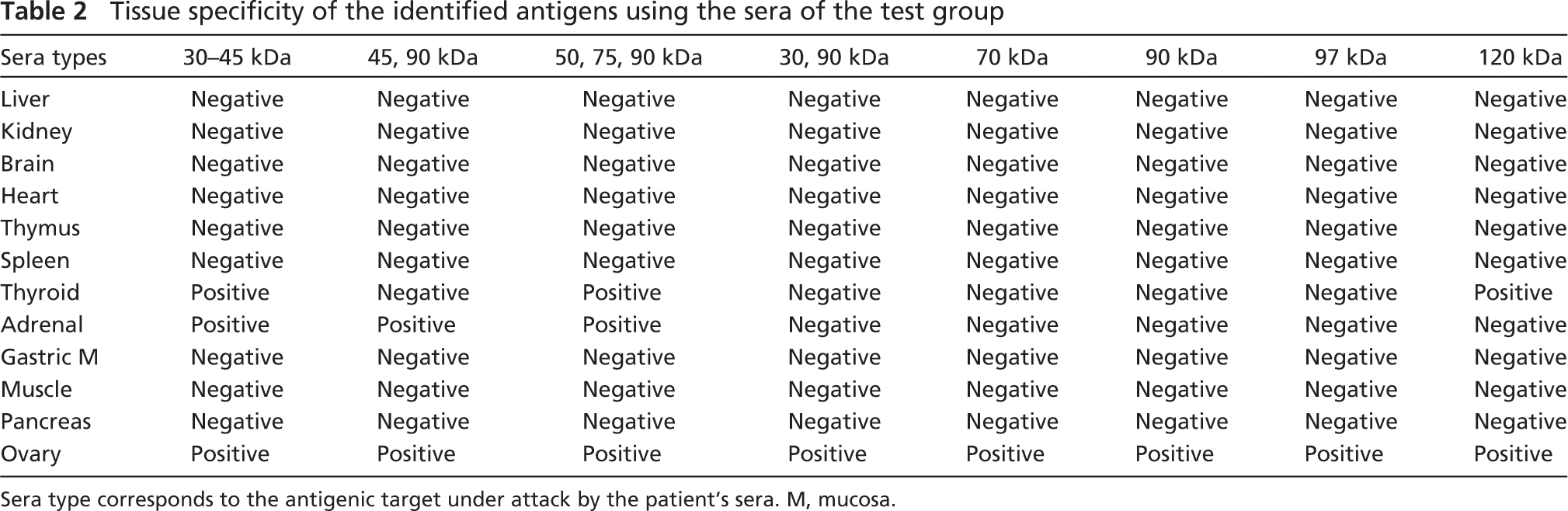
Sera type corresponds to the antigenic target under attack by the patient's sera. M, mucosa.
Reactivity of AOAs to ovarian cell types has been shown by IIF (Irvine et al. 1968; Sotsiou et al. 1980; Elder et al. 1981; Ahonen et al. 1987). However, there was no specificity, and it varied according to source of ovarian tissue and maturation state. It has been reported by Luborsky (2002) that the IHC results by several researchers have been tabulated as positive or negative, but specific reaction sites are rarely depicted pictorially. However, our IHC data very clearly showed reactivity with the cellular targets. Kelkar et al. (2005) and Koyama and Hasegawa (2006) reported reactivity of POF patient sera with zona pellucida (ZP) and suggested that ZP could be an important ovarian antigen. However, our data clearly indicated that, besides ZP, several proteins from other cellular targets such as oocytes, corpus luteum, theca, and granulosa cells are definitely involved in ovarian autoimmunity.
A specific non-invasive test is particularly important for a reliable diagnosis of an autoimmune etiology and is essential to detect concomitant or future associated disorders, as well as to select the patients in whom immune-modulating therapy may restore, at least temporarily, ovarian function and fertility. Glucocorticoid therapy has been suggested to restore ovarian function (Corenblum et al. 1993). A prospective, randomized controlled study of alternate prednisone therapy for AI-POF was taken up at clinical center of the National Institutes of Health. However, lack of a non-invasive diagnostic serum marker necessitated histological confirmation of the disease using biopsy before prednisone administration. Even today, there is no specific, non-invasive diagnostic serum marker available. In fact, our study clearly showed that multiple antigenic targets are involved, and therefore, there cannot be a diagnostic test based on one single biomarker. Our data suggest that the antibodies could be targeting oocyte/granulosa cell/theca cells and corpora luteal cells and thereby causing subsequent pathology.
We can therefore conclude that detection of specific autoantibodies is the most practical clinical and research marker of autoimmune disease. Using both Western blot analysis and IHC, we showed that several patients with POF and IVF-ET patients exhibited the presence of antibodies to ovarian antigens. The Western blot data confirmed that multiple molecular targets seem to be involved in ovarian autoimmunity, whereas IHC data clearly indicated involvement of multiple cellular targets such as ovarian cellular elements and oocyte antigens. Repeated IVF attempts are likely to induce production of AOAs because of repeated hormonal stimulation (Moncayo et al. 1990) and repeated microtrauma during oocyte retrieval (Monnier-Barbarino et al. 1991). It has been shown by these researchers that these antibodies could affect egg development and embryo development and could be responsible for implantation failures. There are reports showing higher prevalence of these antibodies in patients with IVF failures than those with IVF success (Geva et al. 1997). It has also been stressed that follicular aspiration may not be the cause for anti-ovarian autoimmunization (Forges et al. 2006. Moreover, in some cases, AOAs appear after follicular aspiration, whereas in other cases, preexisting AOA levels increase with the number of IVF attempts (Gobert et al. 1992). Therefore, testing for the presence of AOAs in women before initiation into the IVF-ET program should be recommended because this would help to counsel the patients regarding the reproductive outcome with IVF. We also propose that the AOA test should be a part of the battery of tests included for infertility treatment and management. A specific non-invasive test like the one developed by us (Pires et al. 2006) will not only help the clinician in proper disease management but also in the treatment of those who are AOA positive. A pilot study conducted by us (data not shown) showed effective application of this diagnostic test in AOA-positive IVF patients who were put on corticosteroid therapy. The patients were followed up for their AOA status every month. Once these patients reverted to an AOA-negative status (as assessed by our tests), they were taken for the IVF-ET procedure, and an increase in fertility (in terms of pregnancy rates) was observed. This initial finding throws light on the clinical significance of AOA testing in these patients and selecting them for immune therapy before enrolling them into the IVF-ET program.
In conclusion, it is clear that the test developed by us is useful in terms of its specificity; but it has its limitations in regard to the dilution of the sera. We have now embarked on molecular characterization of these autoantigens and are in the process of identifying the autoantigens' immunodominant antigenic peptides. Using these peptides, we plan to set up peptide-based microarrays that have been shown to detect antibodies in diluted human sera with high specificity (Andresen et al. 2006).
Footnotes
Acknowledgments
E.S.P. thanks the Council of Scientific and Industrial Research (CSIR, New Delhi) for financial support (as Senior Research Fellow) received during the course of this study.
The authors thank Dr. Chander P. Puri, Director of the Institute, for support during this study and Dr. Beena Joshi for assistance with statistical analysis. We also thank Dr. Padma Menon and her team from the Department of Endocrinology, King Edward Memorial (KEM) Hospital, Mumbai, for providing us with sera of POF subjects.