
Abstract
The use of multiple probes in fluorescence in situ hybridization (FISH) permits the simultaneous analysis of several chromosomes in both blastomeres and spermatozoa. Preimplantation genetic diagnosis (PGD) for aneuploidy provides information on embryonic chromosomal status, enabling the selection of embryos carrying aneuploid condition. This strategy directly affects implantation, as documented for patients with a poor prognosis for pregnancy, who have the tendency to generate high proportions of chromosomally abnormal embryos. PGD for aneuploidy also has contributed information on early phases in human embryology by clarifying the molecular basis in some cases of irregular development. Multicolor FISH has also been used to study chromosomes on spermatozoa. Experimental strategies and modifications enabled the analysis of samples with a very low number of sperm cells, including samples retrieved from the genital tract or directly from the testicular tissue. The results confirmed that the incidence of aneuploidy increases proportionally with the severity of the male-factor condition. This observation suggests that, in selected cases, the paternal contribution to aneuploidy in the developing conceptus could be more relevant than expected from general data from aborted fetuses and live births.
Keywords
E
Preimplantation genetic diagnosis (PGD) for aneuploidy provides information for embryonic chromosomal assessment. This information is of great importance in some groups of patients and contributes an additional criterion for embryo selection. Data reported on the clinical outcome after PGD for aneuploidy show the main results are an increased implantation rate, a reduced incidence of spontaneous abortion, and a minimized risk of trisomic conception (Gianaroli et al. 1999,2003; Munné et al. 1999; Munné 2002). Thus, this approach is aimed both at improving the chances of healthy implantation and at increasing the efficiency of assisted reproductive techniques by refining the methods of embryo selection when morphological criteria alone are not sufficient to identify viable embryos.
The data obtained by the chromosomal analysis of preimplantation embryos have confirmed the exposure to nondisjunction events during oogenesis, providing the molecular basis for the known decline in the reproductive outcome of women in advanced age. These findings suggest that chromosomal abnormalities could be the reason for poor reproductive performance in other groups of infertile patients and encourage an attempt to identify categories of patients for whom PGD for aneuploidy might be of benefit.
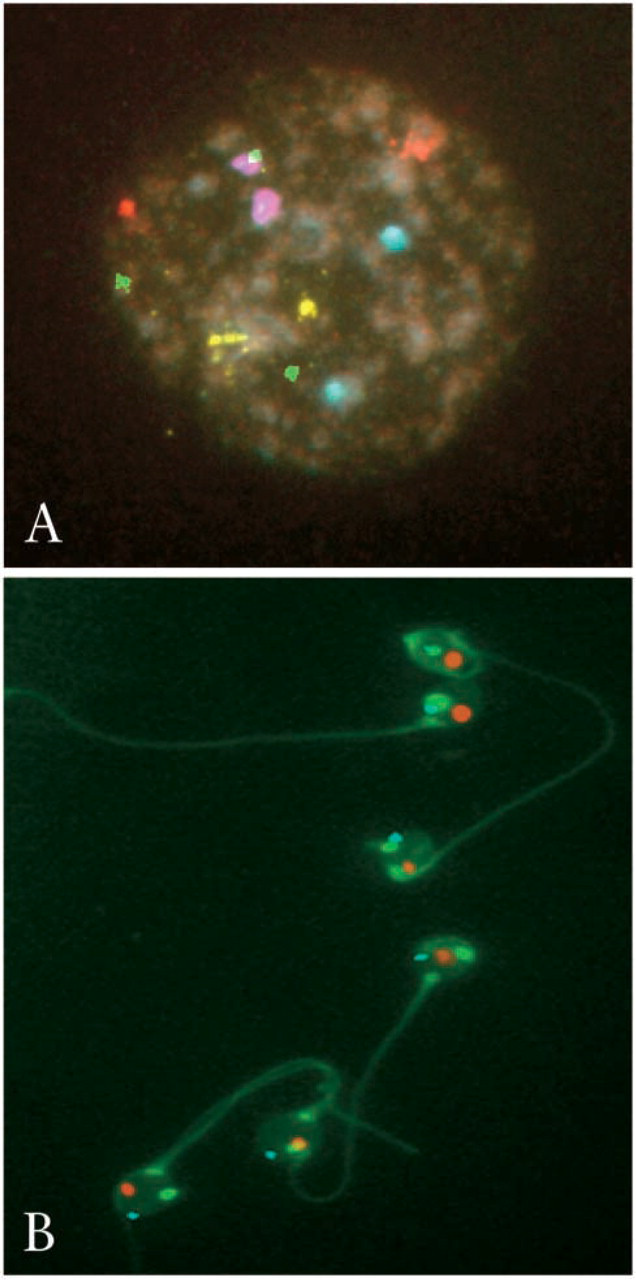
Conventional karyotype analysis is not possible in preimplantation embryos because of the low yield of metaphase chromosomes after anti-mitotic treatment. Therefore, alternative approaches have been developed, and PGD for aneuploidy is mostly based on fluorescence in situ hybridization (FISH) in interphase nuclei (Figure 1A).
FISH has also been applied to study chromosomes in spermatozoa (Figure 1B) and makes it possible to include this investigation, otherwise extremely complicated, as a routine test for the screening of infertile couples. The introduction of intracytoplasmic sperm injection (ICSI) in assisted reproduction more than a decade ago (Palermo et al. 1992) has permitted treatment of male infertility at an increasing rate that is now close to a ratio of 1:1 compared with conventional insemination. Because karyotype results from the children born after ICSI report increased incidence of de novo chromosomal abnormalities, with a notable rise in sex chromosome aneuploidy (Bonduelle et al. 2002), the paternal contribution to aneuploidy is now considered as possibly relevant, especially in cases of severe male-factor infertility.
The aim of this study was to evaluate the results generated by the analysis of preimplantation embryos for the chromosomes that are mainly involved in numerical defects in the human. Special attention was dedicated to estimating the paternal contribution to aneuploidy by directly analyzing chromosomes on spermatozoa and by evaluating the incidence of aneuploidy in embryos in relation to the sperm quality.
Advanced maternal age has been the first indication for PGD of aneuploidy based on the consideration that the selection of euploid embryos could reverse the age effect. Other categories of younger patients with a poor prognosis for pregnancy were also included in the study: (a) multiple unexplained failures in three or more consecutive cycles of in vitro fertilization (IVF); (b) an altered karyotype caused by gonosomal mosaicism or by structural abnormalities such as translocations or inversions; (c) the occurrence of repeated spontaneous abortions in couples with a normal karyotype; and (d) a condition of gonadal failure in women (poor responders) and men (azoospermia).
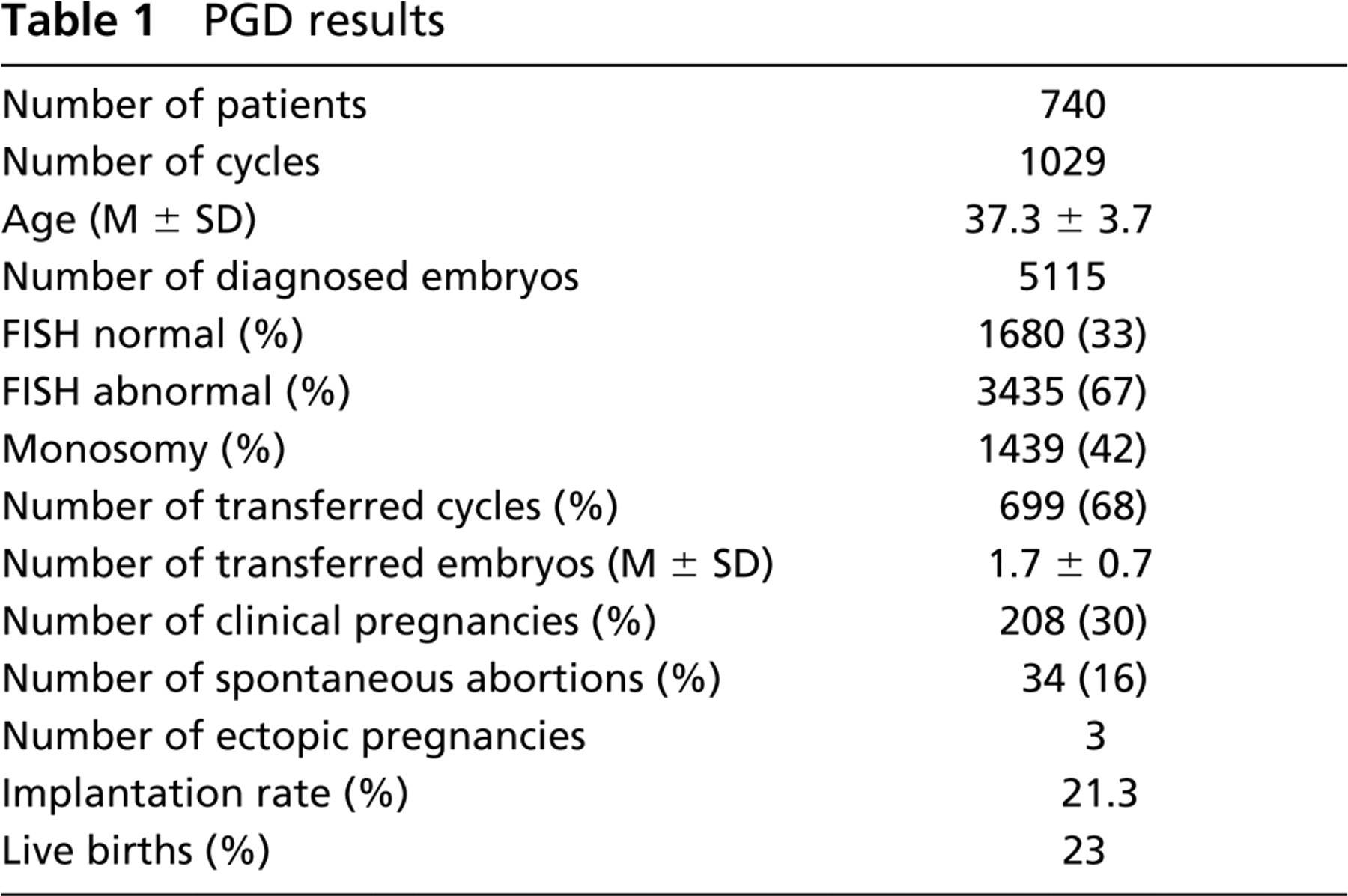
Between September 1996 and December 2003, PGD for aneuploidy was performed in 1029 conception cycles at S.I.S.ME.R. Reproductive Medicine Unit (Table 1). A diagnosis was obtained in 5115 embryos (99% of 5152 biopsied embryos); of these, 1680 had a normal chromosomal complement (33%) and made the transfer possible for 699 cycles (68%) with an average of 1.7 ± 0.7 euploid embryos replaced. Two hundred eight clinical pregnancies were generated (30%) with an implantation rate of 21.3%.
Multicolor FISH analysis on blastomeres
The analysis of the data revealed that the proportion of aneuploid embryos was high in the studied categories of patients, exceeding 60% in all cases except for patients with repeated IVF failures, for whom the figure was 59%. As expected, the type of abnormality differed among the studied groups, with monosomy and trisomy being the prevailing defects in the patients of advanced maternal age (43%), patients with gonosomal mosaicism (43%), those with a history of recurrent abortions (42%), poor responders (45%), and azoospermic patients (43%). The results indicate that such patients have a tendency to generate aneuploid conceptuses, although additional factors may contribute to their poor prognosis for pregnancy.
PGD results
In the patients with repeated IVF failures, the most frequent defects were complex abnormalities, haploidy, and polyploidy, which accounted for 64% of total abnormalities. This frequency was significantly different from that in patients of advanced maternal age (57%, p<0.001), suggesting the possibility of alterations in the mechanisms of cell division, such as asynchrony between karyokinesis and cytokinesis, or centriolar defects. The male gamete could have a role in determining this condition, because the first oocyte divisions are controlled by the sperm-derived centriole and corresponding microtubule organizing regions (Schatten 1994). The sperm centrosome also determines the plane of the first cleavage, with critical consequences for the polarity and ploidy of the resulting embryo (Edwards and Beard 1997). In the present study, the proportion of couples with male-factor infertility was 71% in the group with repeated IVF failures vs 44% in the group of patients with advanced maternal age (p<0.001). This difference in the frequency of male-factor infertility could explain the results of the chromosomal analysis in the resulting embryos for which complex abnormalities were the prevailing defect.
Besides demonstrating the clinical relevance of PGD for aneuploidy, PGD also provides information on early embryology. Two factors are especially relevant: (a) the association between chromosomal status and embryo morphology and (b) the frequency with which specific chromosomes undergo aneuploid events.
As shown in Figure 2, embryos with seven or eight cells at 62 hr after insemination, with less than 10% fragmentation, absence of multinucleation, or cytoplasmic irregularities, have the highest chances of being chromosomally normal (Magli et al. 2001). At this stage, more than half of the abnormalities (825 abnormal embryos, representing 51% of the 1617 analyzed) are monosomies and trisomies (30% of total abnormalities), whereas complex abnormalities, haploidy, and polyploidy prevail in embryos cleaving at an abnormal rate, either too slowly (four to six cells early on day 3) or too fast (more than eight cells early on day 3). The presence of an aneuploid complement does not preclude development of a morphologically normal blastocyst, confirming that morphological criteria alone are of limited value in poor-prognosis patients (Magli et al. 2000).
The analysis of PGD data has revealed that each chromosome originates aneuploidies at a different rate. In the patients with an age factor, the group most exposed to segregation errors, chromosomes 15, 21, and 22 exhibited the highest rate of variation followed by chromosomes 13 and 16 with a proportional increase in relation to age. Chromosomes 1, 14, 17, 18, X, and Y showed similar aneuploidy rates irrespective of age (Gianaroli et al. 2002,2003). These data are in agreement with others (Munné et al. 2004) and suggest that if some chromosomes are more prone than others to nondisjunction at meiosis in an age-dependent manner, other chromosomes might have different frequencies of aneuploidy in other categories of poor-prognosis patients. Figure 3 depicts the results of chromosome-specific variations in the groups of patients included in the study. These data have a distribution different from that of patients of advanced maternal age, confirming that, despite the common tendency to generate high proportions of chromosomally abnormal embryos, the genesis of a poor-prognosis condition probably differs among the groups studied. Two observations were especially interesting. First, in patients with an altered karyotype caused by gonosomal mosaicism, all the tested chromosomes varied at similar rates, suggesting that, if these patients have a tendency to generate mosaic cell lines, all chromosomes seem to be equally involved. Second, azoospermic patients had a pattern similar to that observed in the patients of advanced maternal age, with higher frequencies for abnormalities of chromosomes 15, 21, and 22 (43%, 39%, and 44%, respectively). This finding further suggests that aneuploidy could be especially frequent in gametes derived from azoospermic patients and is in agreement with the data that report an increase in the percentage of de novo chromosomal abnormalities in babies born after ICSI. Similar findings were observed in patients with a poor response to hormonal stimulation (Gianaroli et al. 2000a). It can be postulated that a condition of gonadal failure occurring in young patients could resemble ageing, with the same consequences on the process of meiosis that have been described for women of advanced reproductive age.
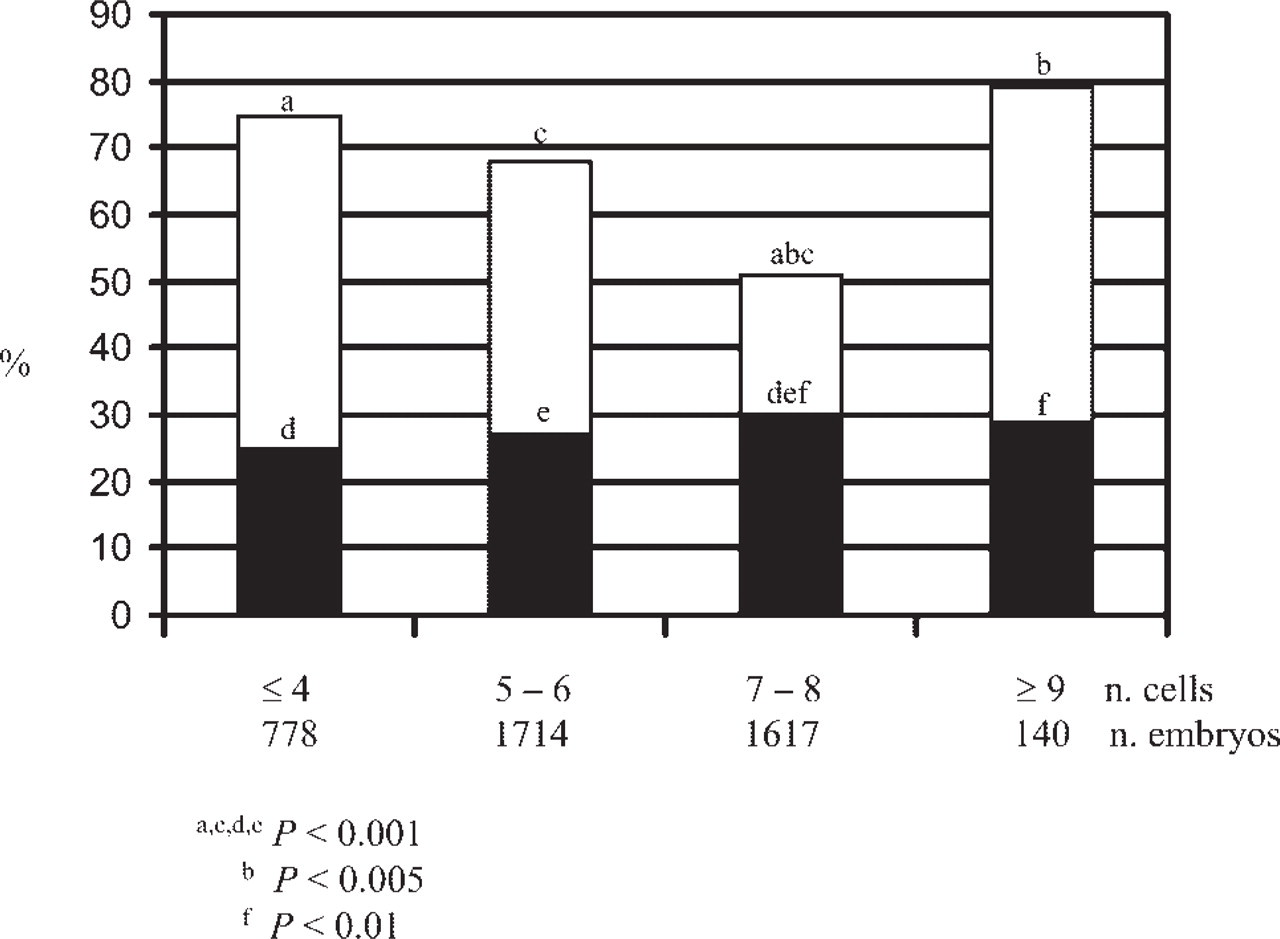
Chromosomal abnormalities and cellular stage at 62 to 64 hr after insemination. The bars represent the total abnormalities, and the dark areas indicate monosomies and trisomies. Values with same letter designation are significantly different.
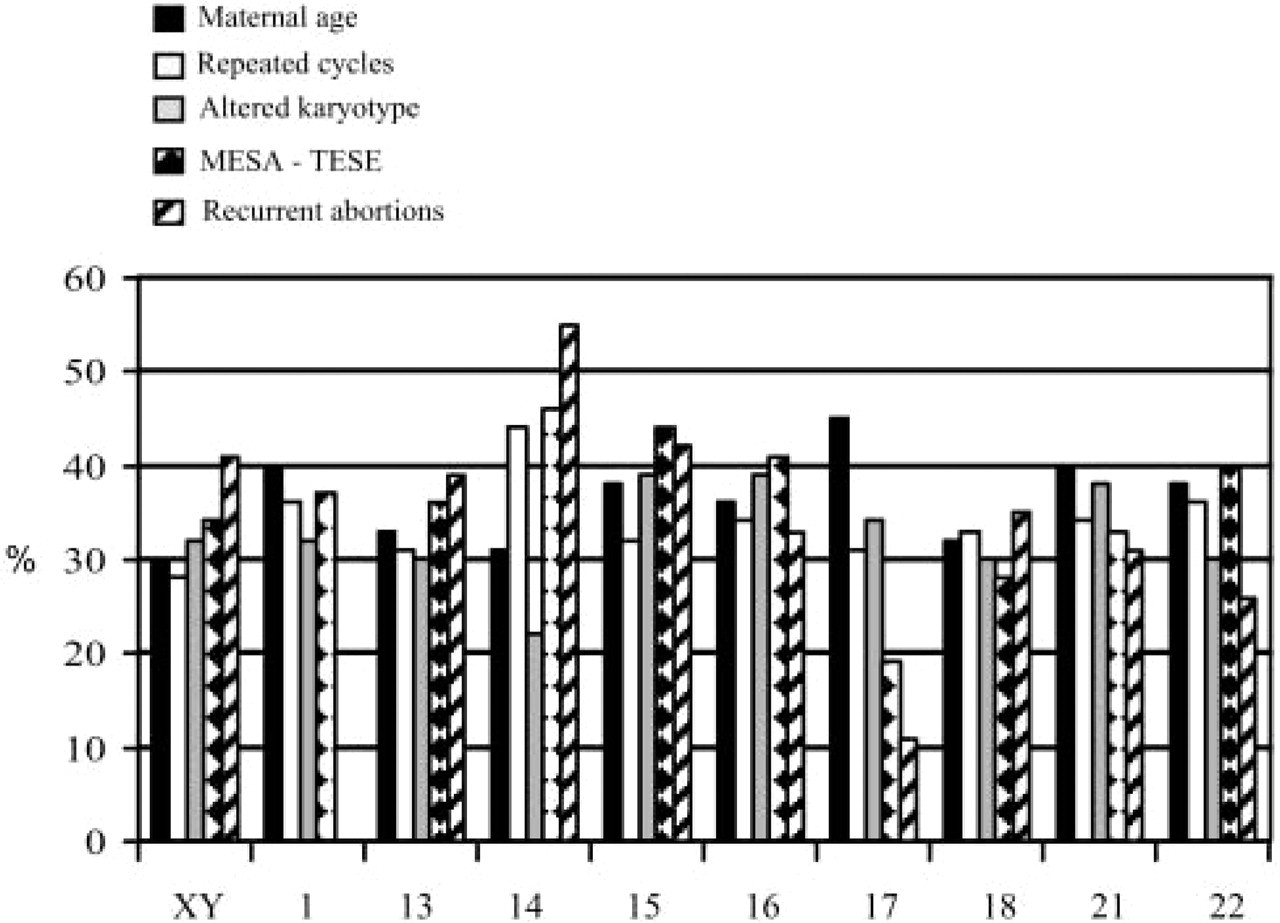
Distribution of abnormalities per analyzed chromosomes in different PGD indications.
Additional data are needed to validate these preliminary observations, but the main conclusion is that chromosomes other than those routinely tested by PGD might be important in determining embryo viability. The identification of these specific chromosomes probably depends on the type of patients, their history, and the indication for PGD.
The widespread use of ICSI for the treatment of extremely severe male-factor infertility in reproductive medicine and the data from the follow-up of the children born have raised concern about the safety of the procedure (Bonduelle et al. 2002). The resulting increased incidence of de novo chromosomal abnormalities suggested the possibility that in selected groups of patients the paternal contribution to aneuploidy could be relevant. This subject was indirectly investigated in a study in which a group of 136 patients underwent PGD for aneuploidy (Gianaroli et al. 2000b). Only couples with a female partner younger than 36 years were admitted to evaluate the effect of sperm indices on the chromosomal constitution of preimplantation embryos. The results were analyzed by dividing the patients in four groups according to the sperm parameters: (a) normospermic patients requiring ICSI for previous fertilization failures, (b) moderately oligoastenoteratospermic (OAT) patients, (c) severely OAT patients, and (d) azoospermic patients with sperm retrieved by microsurgical interventions in the epididymus using microsurgical epididymal sperm aspiration (MESA) or in the testis using testicular sperm extraction (TESE). The data were compared with data obtained from normospermic patients undergoing conventional insemination.
There were no differences in the overall percentage of chromosomally abnormal embryos in the different groups. A higher incidence of monosomies and trisomies, however, was found in embryos generated by MESA and TESE sperm. In addition, the rate of aneuploidy for sex chromosomes increased proportionally with the severity of the male-factor condition. The extension of this study to other cases allowed the evaluation of differences between MESA and TESE embryos and, in the TESE embryos, between those generated by patients with obstructive and non-obstructive azoospermia. In agreement with other reports (Silber et al. 2003), complex abnormalities were the prevailing defect in embryos generated by TESE patients with non-obstructive azoospermia. In addition, this group also presented a significant increase in gonosomal aneuploidy (unpublished data).
FISH evaluation of sperm
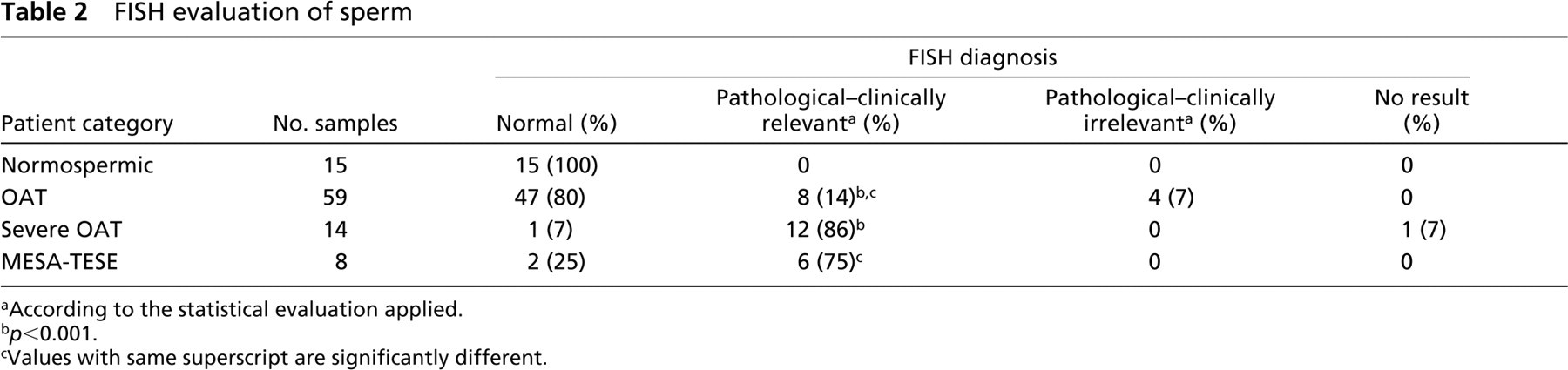
aAccording to the statistical evaluation applied.
b p<0.001.
cValues with same superscript are significantly different.
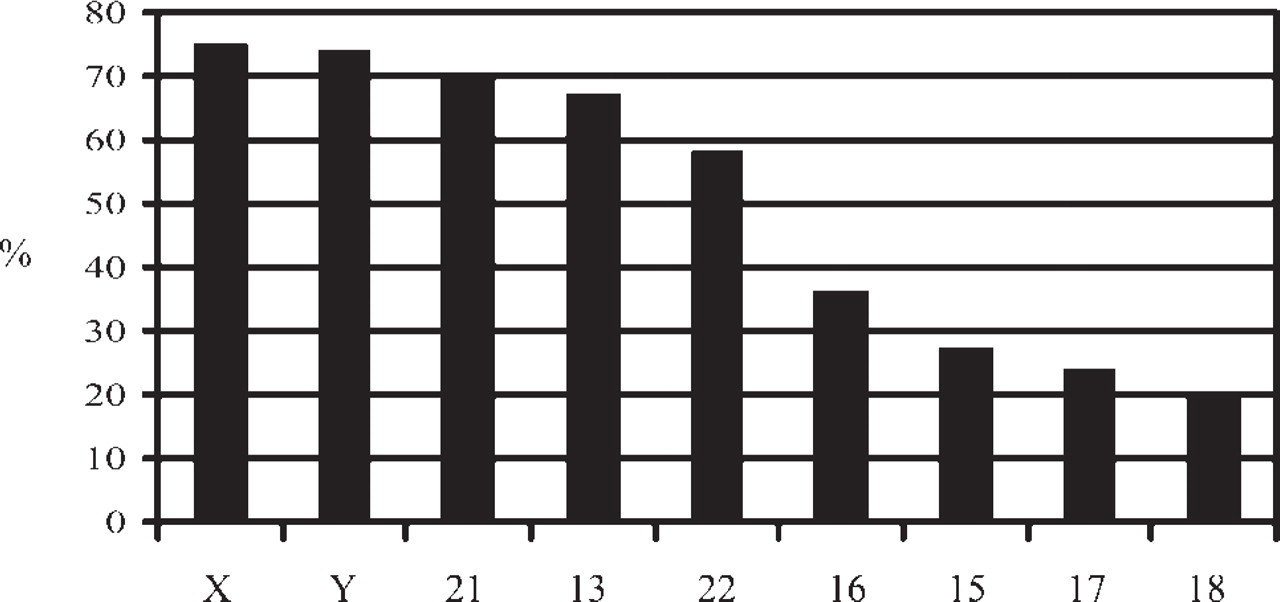
Frequency of aneuploidy per single chromosome on spermatozoa analyzed by FISH.
These results showed the importance of including the chromosomal analysis of sperm cells in the preliminary tests given infertile couples, especially in cases of repeated failures in cycles of assisted reproduction. Several reports have documented the greater frequency of chromosomal abnormalities in spermatozoa from infertile males as compared with the normospermic population (Egozcue et al. 1997; In't Veld et al. 1997; Pang et al. 1999; Bernardini et al. 2000).
A FISH test with probes specific for chromosomes 13, 15, 16, 17, 18, 21, 22, X, and Y was developed and applied to 96 sperm samples (15 normospermic, 59 OAT, 14 severely OAT, and 8 MESA and TESE spermatozoa). When available, 5000 spermatozoa were analyzed by combining the three probes in three different sets. In cases of extremely severe oligospermia, each spermatozoon was analyzed with a five-probe mixture while its position on the slide was recorded. A second-round hybridization followed with the four remaining probes on the same slide, allowing analysis of nine chromosomes for each sperm cell (unpublished data). Results were analyzed using a statistical analysis based on chi-square test by applying the binomial distribution of Poissons. The results were interpreted by assigning clinical relevance of the detected aneuploidy at p values lower than 0.001. In these cases, patients were sent to the andrologist to evaluate the necessity of a therapy aimed at improving sperm indices, including the proportion of aneuploid cells. The highest incidence of aneuploidy was detected in samples belonging to severely OAT and MESA-TESE patients (Table 2). The difference was significantly relevant when compared with the normospermic population.
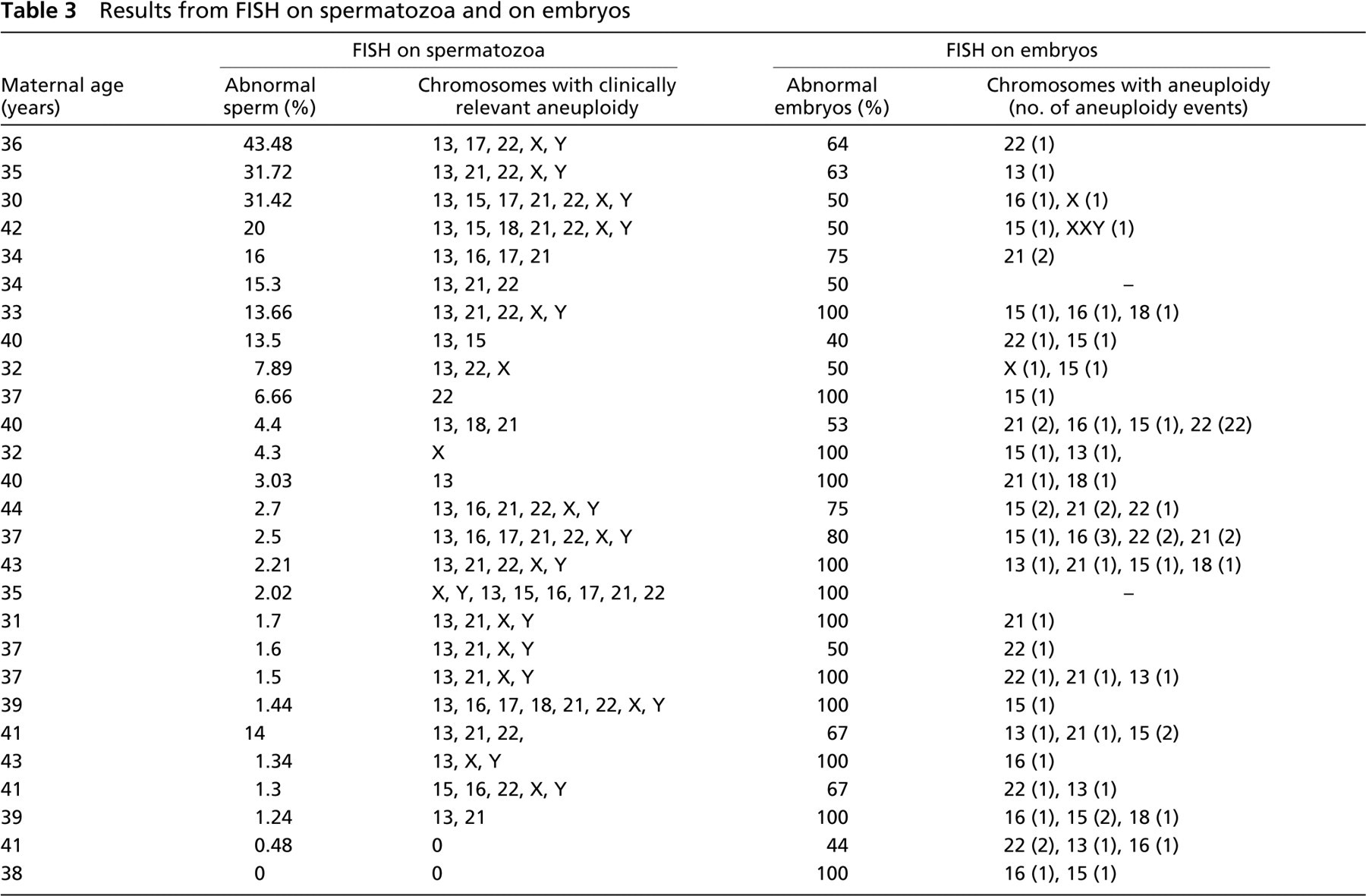
Results from FISH on spermatozoa and on embryos
For the tested chromosomes, the analysis of aneuploidy showed different frequencies of variation, with the highest values for sex chromosomes, followed by chromosomes 21, 13, and 22 (Figure 4).
Although the maternal contribution to aneuploidy is prevalent, with 90% of trisomic pregnancies being maternal in origin (Koehler et al. 1996), the current results could represent a factor of reproductive risk. The derived clinical implications are still unknown, but probably the increasing number of ICSI pregnancies will contribute more data in a few years, and these data could be substantially different from those obtained from the general population.
In our center, for patients of poor prognosis, the first treatment option is generally FISH on embryos. After a failed cycle of PGD for aneuploidy on blastomeres with no transfer caused by FISH results or no pregnancy after repeated PGD cycles, FISH on sperm is recommended to the male partner. If the results are within the normal range, a cycle with polar body biopsy is the following step. Conversely, if the results are significantly abnormal, the patient is referred to the andrologist; if therapy is recommended, the FISH test is repeated after completion of the treatment (Magli et al. 2004). The aim of this approach is to determine whether the aneuploidy originates in the gametes or in the embryos. In some cases, comparison with the results obtained by FISH analysis is informative and permits correlations between aneuploidy in gametes and embryos to be established. Table 3 shows the data from 27 couples that underwent FISH on sperm and embryos. Although a higher number of cases will be needed to draw valid conclusions and to control for the dominant effect of female age, this approach seems to be promising in indicating correlations between sperm aneuploidy and the resulting embryos. According to these very preliminary data, when sperm aneuploidy exceeds 10% in patients younger than 36 years, mosaicism seems to be the prevailing defect in the generated embryos.
In conclusion, FISH results in preimplantation embryos have been reported to have a prognostic usefulness for subsequent attempts (Ferraretti et al. 2004). The possibility exists that a cutoff level in the frequency of aneuploidy could be established for sperm, allowing the reproductive possibilities for each infertile couple to be predicted. This strategy, in association with the most adequate therapeutic program, offers patients the most favorable management.