
Abstract
The development of a non-invasive method of prenatal diagnosis in maternal blood has been the goal of our investigations during the last years. We have developed several anti-CD71 monoclonal antibodies and optimized a protocol for the isolation of nucleated red blood cells (NRBC) from peripheral maternal blood. The enhanced traffic of fetal erythroblasts into the maternal circulation in preeclampsia has been investigated by several groups. In this study, we compared one of our antibodies, 2F6.3, with a commercial anti-CD71 antibody in blood samples from pregnant women suffering pregnancy-induced hypertension (PIH) and in a control group of pregnant women without clinical features suggestive of an increased risk of developing preeclampsia. The mAb 2F6.3, developed by our group, has succeeded in isolating a significantly higher number of erythroblasts with less maternal cell contamination than the commercial antibody in both women with PIH and in the control group (p<0.01; Wilcoxon Signed Ranks Test). Florescence in situ hybridization analysis also demonstrated that 2F6.3 is a better antibody for the isolation of fetal NRBC in maternal blood than the commercial anti-CD71 antibody.
Keywords
I
Many researchers have selected nucleated red blood cells (NRBC) as the target cells for the development of a non-invasive method of prenatal diagnosis in maternal blood. Erythroblasts have several advantages over other types of fetal cells, such as their relative abundance in the early fetal circulation, the expression of antigens that allows their enrichment and identification, and their short life span, which precludes the isolation of fetal cells from previous pregnancies (Pearson 1967; Sitar et al. 1997; Bianchi and Lo 2001).
Because of the scarcity of fetal cells in maternal circulation, approaches are needed to enrich fetal erythroblasts from maternal peripheral blood (Steele et al. 1996). Magnetic cell sorting has been the most widely employed method. This approach is based on the binding of an immunomagnetically labeled monoclonal antibody (mAb) to a cell-surface antigen present on fetal NRBC. The most widely used mAbs for fetal NRBC isolation are those directed against the transferrin receptor (CD71) (Gänshirt et al. 1992).
Preeclampsia is a multisystem disorder characterized by hypertension and proteinuria that occurs late in the second or, more frequently, in the third trimester of pregnancy. The disease adversely affects 3–5% of pregnancies and is one of the most important causes of maternal and fetal mortality and morbidity in developed countries. It is associated with substantial risks, such as intrauterine growth restriction with attendant complications for the fetus, prematurity, and death. The mother becomes at risk of seizures (eclampsia), renal failure, pulmonary edema, stroke, and death (Roberts and Redman 1993; Ness and Roberts 1996). The pathogenesis of preeclampsia is still not completely understood, but placental dysfunction is thought to be the primary cause of the disease (Redman 1991; Dekker and Sibai 1998; Redman and Sargent 2001; Solomon and Seely 2004). Although the symptoms of preeclampsia become apparent only in the second half of pregnancy, the underlying pathological causes in the placenta occur much earlier. No reliable test exists to identify women at risk of developing the disorder early enough in their pregnancies to permit preventive treatment. In the last few years, however, several studies described the elevation in fetal cell traffic and the increased release of fetal DNA into maternal circulation of pregnant women affected by preeclampsia (Holzgreve et al. 1998; Holzgreve and Hahn 1999; Lo et al. 1999; Al-Mufti et al. 2000; Jansen et al. 2001).
We have developed several anti-CD71 mAbs against fetal erythroblasts (Alvarez et al. 1999) and have optimized a protocol for their isolation from peripheral maternal blood (Prieto et al. 2001). In a previous study done with pregnant women at risk of fetal aneuploidy, we found that one of our mAbs, 2F6.3, isolated a higher number of erythroblasts than a commercially available anti-CD71 antibody (data not shown). Therefore, we selected this mAb for further investigations.
In this study, we compare the efficacy of our 2F6.3 mAb versus a commercial anti-CD71 antibody in the isolation of erythroblasts from blood samples of pregnant women with pregnancy-induced hypertension (PIH), who thus are at risk of developing preeclampsia, and from a control group of pregnant women without suggested clinical features of any disease, at similar gestational ages.
Materials and Methods
Development of 2F6.3 Antibody
The 2F6.3 antibody is a mouse mAb produced by immunization with NRBC from human fetal livers and directed against CD71. Development and characterization of this mAb has previously been described (Alvarez et al. 1999).
Patients
Pregnant women attending the Department of Obstetrics and Gynecology at the Hospital Universitario Central de Asturias (Oviedo, Spain) were recruited for the study with informed consent approved by Human Studies Committee of our hospital. Maternal blood samples (30 ml) were collected from 30 pregnant women suffering PIH and from 13 pregnant women, matched for gestational age, without suggested clinical features of developing preeclampsia (control group). Blood was collected into Vaccutainer tubes (Becton Dickinson, Plymouth, UK) containing EDTA as anticoagulant.
PIH was defined as a sustained rise in diastolic blood pressure to 90 mm Hg or higher above previous values. The pregnant women in the control group were not hypertensive.
The mean gestational ages were 35 weeks (range: 21–40 weeks) and 34 weeks (range: 32–36) for the PIH and control groups, respectively.
NRBC Enrichment from Maternal Blood
We processed blood samples within 1 hr from being drawn. We carried out Double Histopaque (Sigma, St Louis, MO) density gradient centrifugation as described elsewhere (Prieto et al. 2001). Both plasm/1.077 and 1.077/1.107 interfaces were collected separately and split into two aliquots. We processed the aliquots as paired samples using two different mAbs against the transferrin receptor: 2F6.3, and a commercial anti-CD71 antibody (Miltenyi Biotech GmbH, Bergisch Gladbach, Germany). We incubated cell suspensions with 2F6.3 mAb or the commercial magnetically labeled anti-CD71 antibody for 15 min at 4C. We carried out a second incubation with magnetic microbeads conjugated to rat anti-mouse IgG2 antibody (Miltenyi Biotec GmbH, Bergisch Gladbach, Germany) for the fraction processed with 2F6.3 antibody, because this mAb is not magnetically labeled. Labeled cells in both fractions were immediately separated on miniMACS columns (Miltenyi Biotec GmbH, Bergisch Gladbach, Germany). Aliquots of the positively selected cells were cytospun onto slides (Cytospin 3, Shandon, Astmoor, UK).
Identification and Detection of NRBC
Slides were air-dried overnight before being fixed in methanol and stained with diaminobenzidine (DAB, Sigma, St Louis, MO) to detect the presence of hemoglobin and with hematoxylin to counterstain the nuclei. NRBC were identified according to their morphology and DAB staining. The total number of NRBC on the entire cytospun area was enumerated.
Florescence In Situ Hybridization Analysis
We treated the slides with HCl in 70% ethanol for 5 min to remove hematoxylin. We then incubated the slides with RNase A (Sigma, St Louis, MO) in a humidified chamber for 30 min at 37C. After two washings (2 × SSC and then PBS), the slides were treated, for 10 min at 37C, with a 0.0075% solution of pepsin in 0.01 N HCl and then washed three times with PBS for 5 min. The slides were fixed in a 4% formaldehyde/PBS solution for 5 min. After two PBS washings, slides were dehydrated in series of 70%, 85%, and 100% ethanol.
We performed dual-color fluorescence in situ hybridization (FISH) analysis using Spectrum CEP Y green and Spectrum CEP X orange directly labeled probes (Vysis Inc., Downers Grove, IL). We sealed the slides with rubber cement and placed them in a prewarmed humidified incubator (Hybrite, Vysis). They were incubated for 2 min at 90C for denaturation, and then hybridization was carried out overnight at 37C. The next day, rubber cement was removed, and the slides were washed three times in 50% formamide/2 × SSC for 10 min at 46C, following by two washings at 46C (first 10 min in 2 × SSC and then 5 min in 2 × SCC/0.1% Tween 20). Cells were counterstained with 4,6-diamidino-2-phenyl-indol (DAPI II; Vysis, Weisbaden-Delkenheim, Germany) and analyzed with a fluorescence microscope (Leica DMR, Heerbrugg, Switzerland).
Data Analysis
The data were analyzed by SPSS 12.0 Statistical Software Package for Windows (SPSS Inc., Chicago, IL). Because data distribution was not Gaussian, comparison between the number of NRBC isolated using 2F6.3 and the Miltenyi anti-CD71 mAb was carried out using nonparametric tests (Wilcoxon Signed Ranks Test and U-Mann Whitney Test). A p value of <0.05 was considered statistically significant.
Results
We processed 30 peripheral blood samples from pregnant women with PIH, who were thus at risk of developing preeclampsia. The median number of NRBC isolated from 30 ml of maternal blood was 483 (range: 24–7166) with 2F6.3 and 183 (range: 0–3290) with the Miltenyi antibody. The Miltenyi anti-CD71 mAb failed to isolate NRBC in 1 of 30 maternal blood samples. The differences between the numbers of NRBC isolated by the two mAbs were statistically significant (p<0.001; Wilcoxon Signed Ranks Test) (Figure 1).
In addition, 2F6.3 mAb isolated fewer contaminant cells than the commercial antibody. We defined the ratio of total cells/NRBC for each antibody. This ratio can be considered a measurement of the purity of the cell isolation. The median of this ratio was significantly higher with the Miltenyi mAb than with the 2F6.3 mAb (p<0.001; Wilcoxon Signed Ranks Test), showing that the enrichment in NRBC was higher when 2F6.3 was used. The 2F6.3 mAb isolated a median of 1 NRBC in 2783 total cells (range: 1 NRBC in 139–65,625 total cells); the Miltenyi anti-CD71 mAb recovered a median of 1 NRBC in 5813 total cells (range: 1 NRBC in 613–15,9667 total cells). Table 1 summarizes the distributions of NRBC and the ratio of total cells/NRBC isolated from maternal blood samples by both mAbs.
In 13 blood samples from normotensive pregnant women, processed as a control group, 2F6.3 also isolated a significantly higher number of NRBC with less maternal cell contamination. The median of NRBC isolated by 2F6.3 was 262 (range: 9–867), whereas the median recovery by the commercial mAb was 150 NRBC (range: 8–315) (p<0.01; Wilcoxon Signed Ranks Test) (Figure 2). The median of the ratio total cells/NRBC was 8502 (range: 1524–73,556) with 2F6.3 mAb and 15,534 (range: 1870–102,250) with the commercial antibody (p<0.05; Wilcoxon Signed Ranks Test). Table 2 shows the distribution of NRBC and the ratio of total cells/NRBC from these samples.
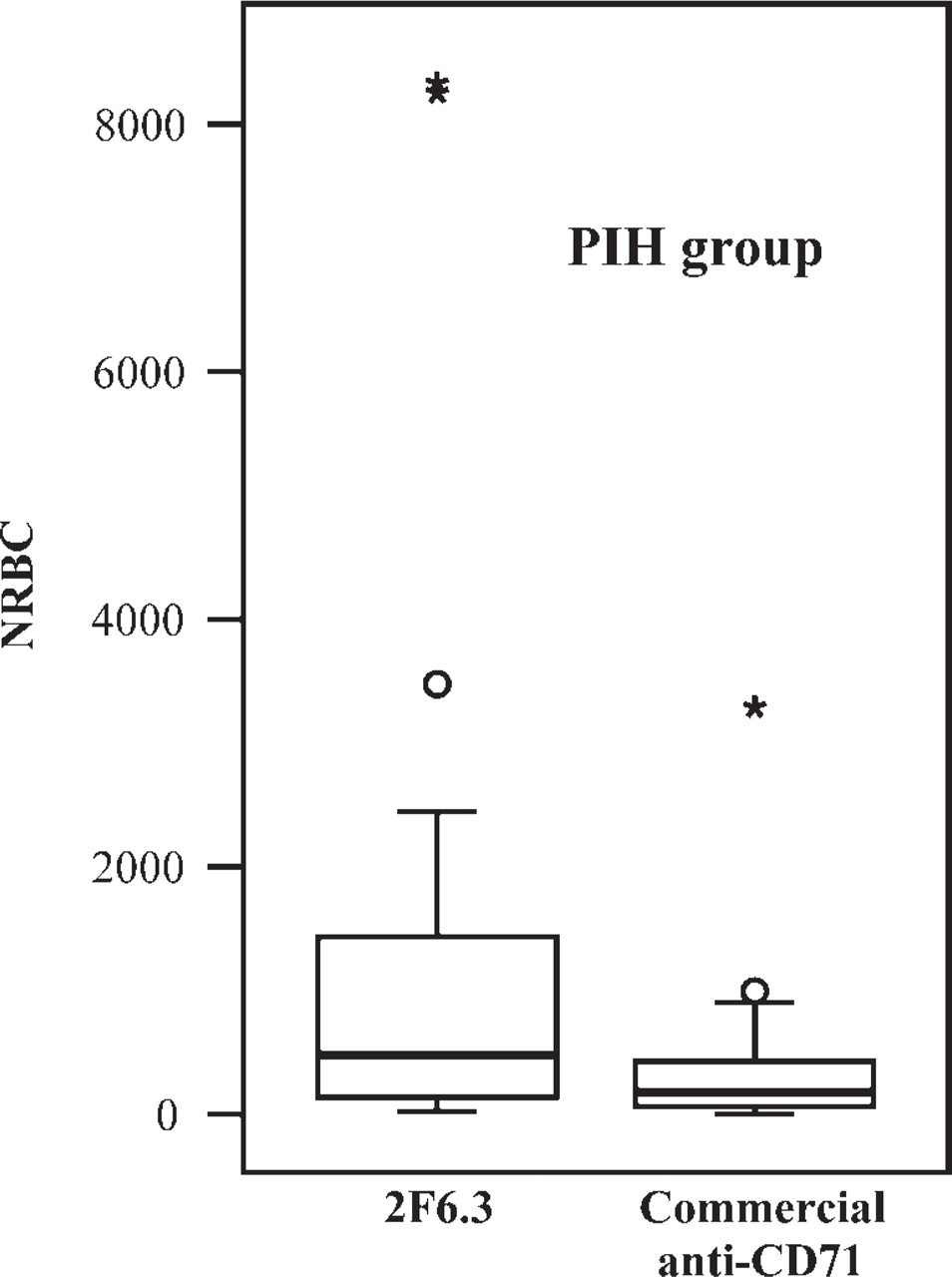
Box plot of the number of NRBC isolated by 2F6.3 and by the commercial anti-CD71 mAbs in samples from pregnant women with PIH. The top and bottom of each box-plot represent 75% and 25% of all values, respectively. The horizontal line is the median. The lower and upper bars represent the 10% and 90% limits respectively. The outliers are shown as open circles and the extremes as asterisks.
We also compared the number of NRBC isolated with 2F6.3 mAb in pregnancies at risk of preeclampsia versus the control group. The median of erythroblasts was higher in the group with PIH than in the group of normotensive pregnant women (483 and 262 NRBC, respectively), but the difference was not statistically significant. We found significantly higher ratios of total cells/NRBC in samples from normotensive pregnancies (p<0.01; U-Mann Whitney Test). In the control group, 2F6.3 isolated a median of 1 NRBC in 8502 total cells (range: 1 NRBC in 1524–73,556 total cells), whereas in the hypertensive pregnant women the median recovery was 1 NRBC in 2567 total cells (range: 1 NRBC in 139–5625 total cells).
NRBC and ratio total cells/NRBC distributions in pregnancies at risk of preeclampsia a
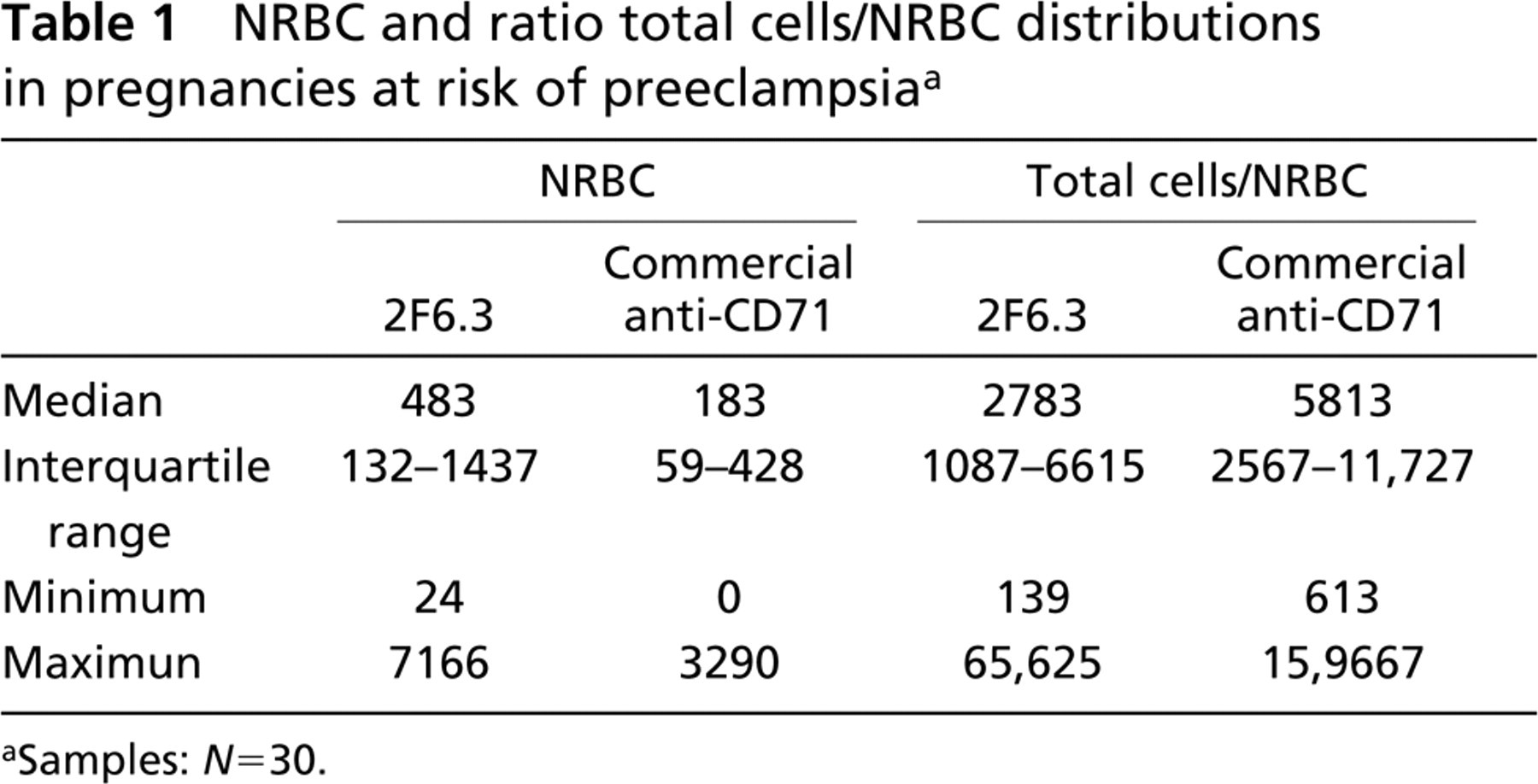
aSamples: N=30.
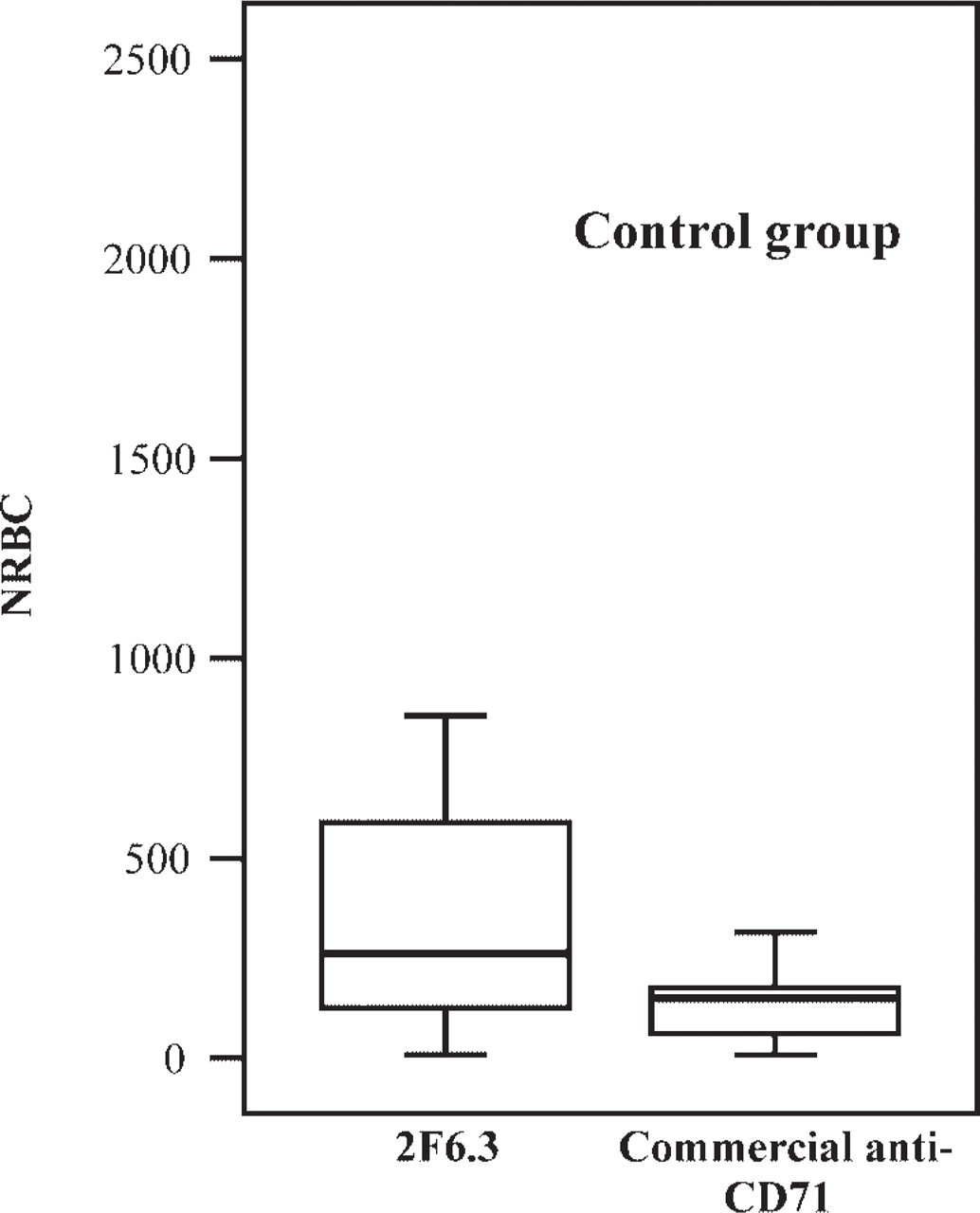
Box plot of the number of NRBC isolated by 2F6.3 and the commercial anti-CD71 mAbs in samples from normotensive pregnant women. The top and bottom of each box-plot represent 75% and 25% of all values, respectively. The horizontal line is the median. The lower and upper bars represent the 10% and 90% limits respectively.
Twelve of the 30 pregnant women with PIH developed preeclampsia. We compared the number of NRBC obtained from the women who developed preeclampsia with the number from the control group. 2F6.3 antibody isolated a higher median number of NRBC in preeclampsia samples (500 versus 262, respectively), but the difference was not statistically significant. The median of the ratio of total cells/NRBC was significantly higher in preeclampsia group, however: 1 NRBC in 3537 total cells, versus 1 NRBC in 8502 total cells in normotensive samples (p<0.05; U-Mann Whitney Test).
NRBC and ratio total cells/NRBC distributions in control group a
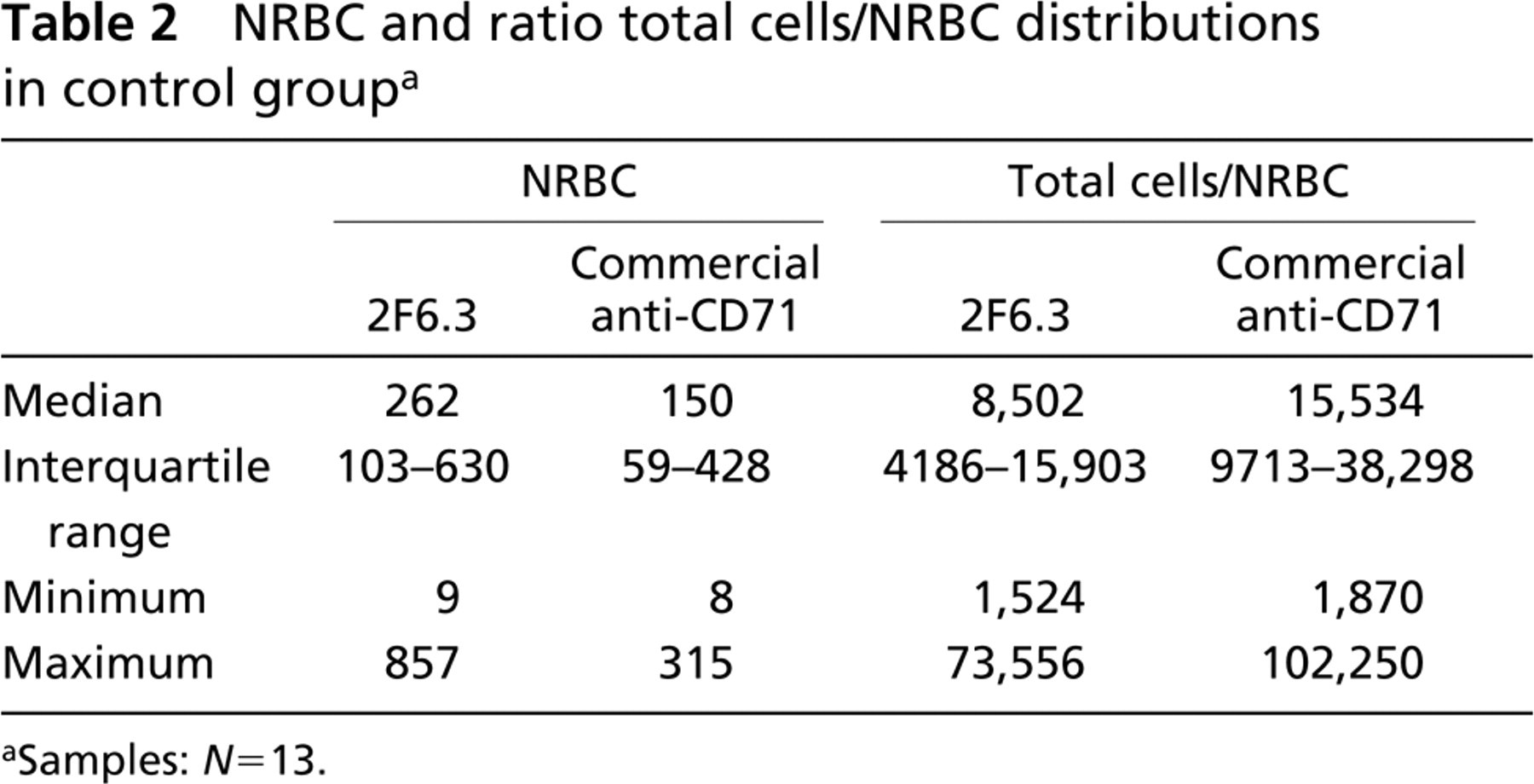
aSamples: N=13.
We used FISH to analyze maternal samples from pregnant women carrying a male fetus to verify fetal NRBC recovery. We processed blood samples from 10 women with PIH and from 6 normotensive pregnant women with both antibodies. In pregnant women at risk of developing preeclampsia, we observed fetal erythroblasts (NRBC with one X and one Y signal) in 60% of the samples processed with 2F6.3 mAb but in only 30% of the same samples processed with the Miltenyi antibody. In the six normotensive pregnancies bearing male fetuses, we found fetal cells in half of the samples tested with both antibodies. The number of fetal NRBC was significantly higher in the samples processed with 2F6.3 mAb (p<0,05; Wilcoxon Signed Ranks Test). In the PIH group, the median percentage of fetal erythroblasts was 0.8% (range: 0.0–12.5%) and 0.0% (range: 0.0–7.7%) for 2F6.3 and the Miltenyi anti-CD71 antibody, respectively. In the control group, the medians were 1.8% (range: 0.0–27.3) and 0.0% (0.0–14.3), respectively. There were no statistically significant differences between the percentage of nuclei with one X and one Y signal in hypertensive and normal pregnancies. Table 3 presents FISH analysis with 2F6.3 and the commercial anti-CD71 antibodies in both groups.
FISH analysis on samples from PIH and normotensive women carrying a male fetus
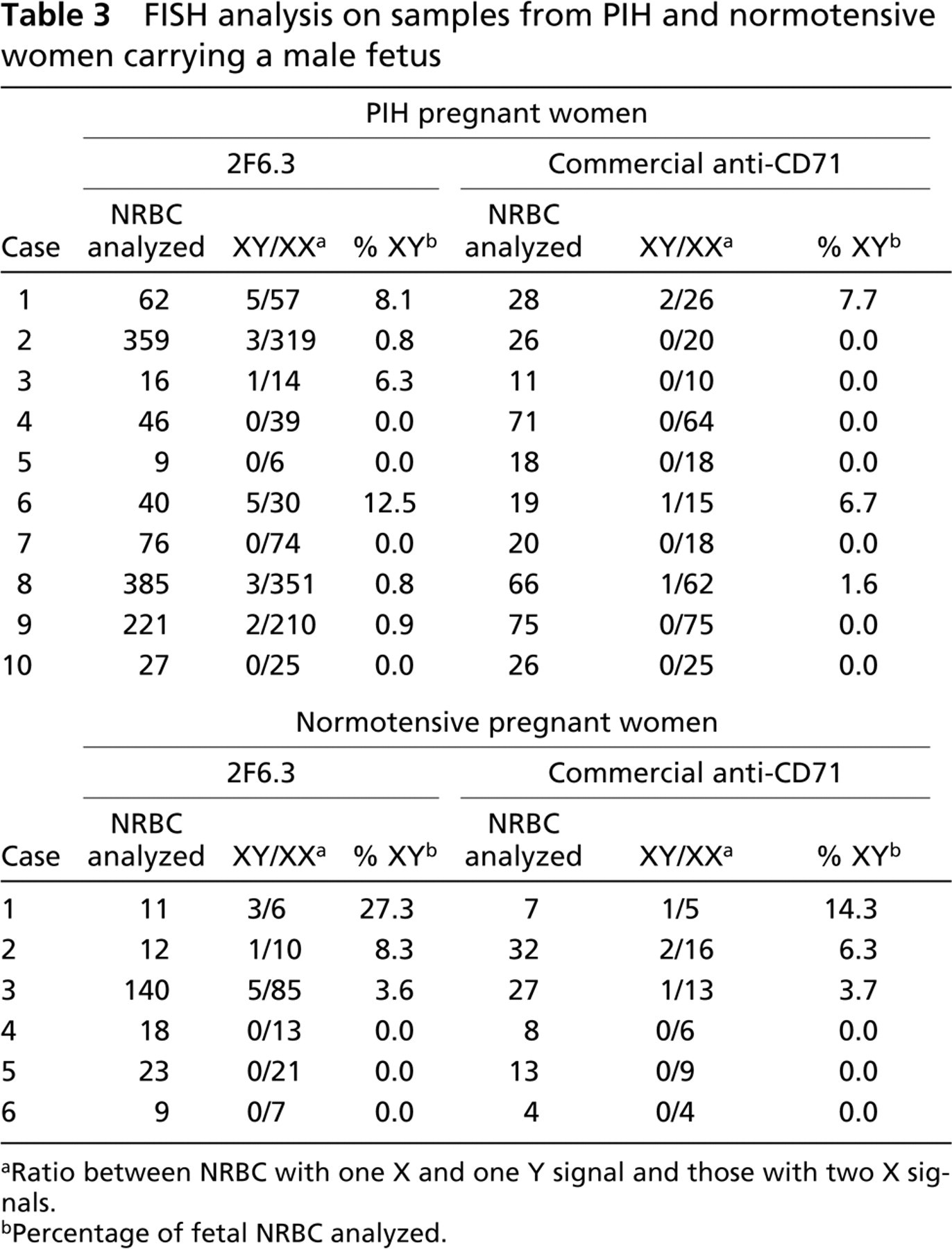
aRatio between NRBC with one X and one Y signal and those with two X signals.
bPercentage of fetal NRBC analyzed.
Discussion
Preeclampsia is an important pregnancy-associated disorder. Increased trafficking of fetal nucleated cells and an elevation in circulating cell-free DNA into maternal blood have been reported in women suffering this disorder (Lo et al. 1996; Leung et al. 2001). Because increased fetal DNA liberation could be secondary to an increased entry of fetal cells, such as trophoblasts and erythroblasts, into the maternal circulation (Bianchi and Lo 2001), the main focus of our group is the use of fetal erythroblasts, isolated by immunoaffinity to CD71, as a means of performing non-invasive prenatal diagnosis.
In this study, one of our antibodies, 2F6.3, demonstrated a higher efficacy in isolating NRBC from peripheral blood of pregnant women at risk of developing preeclampsia than a commercial anti-CD71 antibody; 2F6.3 mAb isolated a significantly higher number of NRBC with less maternal contamination. When we compared these antibodies in normotensive pregnant women, we observed the same result. In a previous study performed with samples from pregnant women at risk of carrying an aneuploidy fetus, 2F6.3 mAb also isolated more NRBC than other antibodies (unpublished data). These findings suggest that this antibody could be a useful tool for non-invasive prenatal diagnosis.
The causes of preeclampsia remain unclear, but the underlying changes leading to the disorder occur early in pregnancy, before manifestation of the symptoms. Gänshirt et al. (1994) described the elevation of the number of erythroblasts in pregnancies affected by preeclampsia. Studies performed on samples collected during the second trimester indicate that this disorder occurs early in those pregnancies in which preeclampsia subsequently develop (Holzgreve et al. 2001b; Zhong et al. 2001; Cotter et al. 2002; Zhong et al. 2002). Our data showed a higher number of NRBC in the blood of patients with PIH than in control samples, but the increase was not statistically significant (p>0.05). Not all hypertension in pregnancy is caused by preeclampsia. Gestational hypertension without proteinuria or other systemic manifestations is frequently confused with preeclampsia but usually has a benign course (Sibai 1996). In this study, only 12 of the 30 pregnant women included in the group at risk for preeclampsia actually developed the disorder. We did not find statistically significant differences in the number of NRBC isolated from preeclampsia and from normotensive samples, but we observed a tendency for an enhanced number of NRBC in preeclampsia cases. A feature observed in all the reports, as well as in our study, is that the number of erythroblasts was not increased in all cases of preeclampsia, and a degree of overlap was seen between preeclampsia and control women groups (Hahn and Holzgreve 2002).
We used FISH probes for X and Y chromosomes to quantify and compare the recovery of fetal NRBC in samples from PIH and normotensive pregnant women carrying male singleton fetuses. Using FISH, Holzgreve et al. (1998) showed a significant proportion of fetal erythroblasts in preeclampsia (up to 50%), but our findings suggest that NRBC isolated in the maternal circulation of the PIH group are predominantly maternal in origin.
The number of fetal NRBC isolated was relatively low with both antibodies but was significantly higher in samples processed with 2F6.3 mAb. The proportion of fetal erythroblasts obtained by our group was comparable to that described by other researchers (Al-Mufti et al. 2000). Several authors have described difficulties that occur during FISH analysis of the sorted erythroblasts. Micromanipulation and PCR analysis of a single fetal cell has been described as a more efficient method than FISH to analyze fetal erythroblasts (von Eggeling et al, 1997; Troeger et al. 1999; Zhong et al. 2002). FISH requires careful handling of cells at all stages of the treatment because of the risk of loss. The scarcity of fetal erythroblasts in the maternal circulation, even after enrichment, requires high hybridization efficiency for DNA probes. In this study, hybridization efficiency median was 90% for both mAbs. The efficiency of 2F6.3 antibody in isolating a higher number of NRBC with less maternal contamination, however, could explain why FISH analysis correctly identified fetal sex in 60% of pregnant women carrying a male fetus when this antibody was used for the enrichment, whereas the commercial anti-CD71 mAb correctly identified only 30% of the male fetuses.
Although increased trafficking of fetal nucleated cells in women suffering preeclampsia has been described, in this study FISH analysis did not show differences between the number of fetal NRBC isolated in the PIH and control groups. In this study, only 12 of the 30 pregnant women with PIH actually developed preeclampsia. Additional research will also be required to investigate whether abnormal fetal cell traffic of NRBC may be detectable even before the development of the clinical signs of preeclampsia. The presence of fetal erythroblasts in maternal blood, in combination with other biochemical markers, would be useful in screening for preeclampsia. The 2F6.3 antibody has demonstrated to be an efficient tool for NRBC recovery from peripheral maternal blood.
Footnotes
Acknowledgements
This project was partially supported by the Special Non-Invasive Advances in Foetal and Neonatal Evaluation Network (SAFE).
We thank all the women who participated in this study and all the physicians who collaborated by sending us maternal blood samples.