
Abstract
Steroid receptor coactivator-3 (SRC-3) has been reported to be overexpressed in the development and progression of many tumor types. SRC-3 has been detected in several lung cancer cell lines, but its expression and clinical significance in non-small cell lung cancer (NSCLC) remain unclear. In this study, 48 NSCLC tissues were collected and tissue microarrays were performed. The expression of SRC-3 was examined using nickel-intensified IHC. The results showed that of these 48 cases, 18 (37.5%) exhibited high levels of SRC-3 immunoreactivity, 23 (47.9%) exhibited moderate levels of SRC-3 immunoreactivity, and 7 (14.6%) were negative; thus, the total frequency of SRC-3 overexpression was 85.4% (41/48). This SRC-3 overexpression frequency was similar to the overexpression frequency observed for squamous cell carcinoma and adenocarcinoma (82.1% vs 90%) and for metastasis and non-metastasis patients (84.6% vs 85.7%). Data analysis demonstrated a significantly higher overexpression frequency in male patients compared with that in female patients (88.6% vs 76.9%). However, female patients tended to have higher expression levels of SRC-3, as measured by immunoreactivity, than male patients. These results demonstrate a high frequency of SRC-3 overexpression in NSCLC with a gender difference, suggesting that there is a specific role for SRC-3 in the pathogenesis of NSCLC. (J Histochem Cytochem 58:1121–1127, 2010)
Keywords
T
SRC-3, presumably acting in its capacity as a transcriptional coactivator, is an oncoprotein (Yan et al. 2006a,b). Amplification of the SRC-3 gene has been correlated with high expression levels and increased tumor size. In addition, SRC-3 amplification has been correlated with estrogen receptor (ER) positivity and progesterone receptor positivity, supporting the role of this coactivator in ER-dependent tumor development and progression (Anzick et al. 1997; Bautista et al. 1998). In mice, transgenic SRC-3 overexpression is sufficient to induce mammary tumorigenesis and increase mammary insulin-like growth factor-1 (IGF-1) mRNA and serum IGF-1 protein levels (Torres-Arzayus et al. 2004). Consistently, a reduction in SRC-3 expression reduces the incidence of Ras-mediated and chemical carcinogen-induced breast tumors (Kuang et al. 2004, 2005) and decreases mammary gland ductal morphogenesis. Mouse model studies have further defined SRC-3 as an important oncogene (Kuang et al. 2004, 2005; Torres-Arzayus et al. 2004) and a master regulator with many other functions (Wu et al. 2002; Louie et al. 2004; Yan et al. 2006a,b, 2008; Yu et al. 2007).
Overexpression of SRC-3 has been observed in other cancers. It is overexpressed in pancreatic adenocarcinoma and its precursor lesions (Henke et al. 2004). In endometrial carcinoma, high SRC-3 expression levels are associated with the parameters of poor prognosis (Balmer et al. 2006; Sakaguchi et al. 2007). In prostate cancer, SRC-3 is overexpressed in prostatic luminal epithelial cells during tumorigenesis. In addition, knockout of SRC-3 in mice suppresses the progression of spontaneous prostate carcinogenesis (Tien et al. 2009). SRC-3 appears to be a tumor promoter in a mouse model of thyroid cancer because of its role in regulating multiple target genes and signaling pathways during thyroid carcinogenesis (Ying et al. 2008). SRC-3 gene amplification has been reported to occur in ovarian tumors with a frequency of 7.4% (9/122) (Bautista et al. 1998) or 29% (9/31). In addition, amplification of SRC-3 has been reported to be associated with both ER positivity in sporadic ovarian carcinomas and poor survival of patients (Tanner et al. 2000).
Lung cancer is the leading cause of cancer deaths in the United States (Harichand-Herdt and Ramalingam 2009). Each year, it is estimated that more than 180,000 new cases of non-small cell lung cancer (NSCLC) are diagnosed in the United States, with about 165,000 patients dying from the disease (Stabile and Siegfried 2003). Several in vitro studies have studied the expression of SRC-3 in lung cancer. For example, SRC-3 expression was detected in the glucocorticoid-sensitive small cell lung cancer (SCLC) model, COR L103 cells (Waters et al. 2004), and the NSCLC cell lines, A549 and H23 (Suen et al. 1998; Marquez-Garban et al. 2007). Other than the in vitro reports mentioned earlier, there is no in vivo clinical data about the SRC-3 expression in lung cancer. To address this question, we evaluated the immunoreactivity of SRC-3 in NSCLC and explored its clinical significance.
Materials and Methods
Patient Specimens
Tissues from 48 patients with NSCLC (Table 1; from January 2003 to December 2003) of both genders and different ages, including 20 cases of adenocarcinoma and 28 cases of squamous cell carcinoma (SCC), and 3 normal lung tissues were obtained from biopsy. All tissues were collected and stored at the Institute of Pathology, Southwest Hospital, Third Military Medical University, Chongqing, China. Study protocols were approved by the local Institutional Review Board. Tumors were classified according to WHO Classification of Tumors (Travis et al. 2004). The tissues were formalin fixed and paraffin embedded. The tissue blocks were sectioned and stained with hematoxylin and eosin (H&E) then used for further investigation.
Tissue Microarray
Three tissue microarrays (TMAs) were constructed as described in a previous report (Li et al. 2009). Briefly, using the H&E sections as templates, representative areas of each tumor were identified and marked on a section of the donor block. Approximately 3-mm-thick (0.6-mm diameter) tissue cylinders were punched from each donor paraffin block using a TMA instrument (Beecher Instruments; Silver Spring, MD). The donor cores were placed into the corresponding recipient block holes that were punched in advance using the same TMA instrument. To better represent each case, two tumor and two normal tissue cores that were located adjacent to the tumor were punched from each case. After construction, recipient blocks were placed into an oven at 37C for 20 min, rapidly removed, and pressed down by a slide for a moment to flatten the surface. Serial 4-μm-thick sections were cut with a Leica microtome (Leica Microsystems; Wetzlar, Germany) and mounted onto polylysine-coated slides.
Immunohistochemistry
The nickel-intensified IHC procedure with TMAs was carried out as described in our previous report (Zhang et al. 2002) with slight modification. Briefly, sections of TMAs were first washed with PBS (0.01 M, pH 7.4), quenched for 15 min in 3% H2O2 (v/v) in PBS, and blocked in 2% normal goat serum (v/v) for 30 min at room temperature. Sections were then incubated overnight at 4C with primary rabbit polyclonal anti-SRC-3 antiserum (sc-25742; Santa Cruz Biotechnology, Santa Cruz, CA) diluted 1:200 with Antibody Diluent (S3022; Dako, Glostrup, Denmark). After several washes with PBS, the sections were incubated with secondary biotinylated goat-anti-rabbit antibody (ZB2010; Zhongshan Golden Bridge Biotechnology, Beijing, China) for 1 hr at room temperature. The sections were washed in PBS, incubated in horseradish peroxidase–labeled streptavidin reagent (ZB2404; Zhongshan Golden Bridge Biotechnology) for 1 hr at room temperature, and then visualized using a DAB–nickel chromogen solution for 5 min at room temperature. Negative controls were carried out using the same procedure, but the primary antiserum was replaced with Antibody Diluent.
Clinicopathological information and expression of SRC-3 in the NSCLC tissue microarray
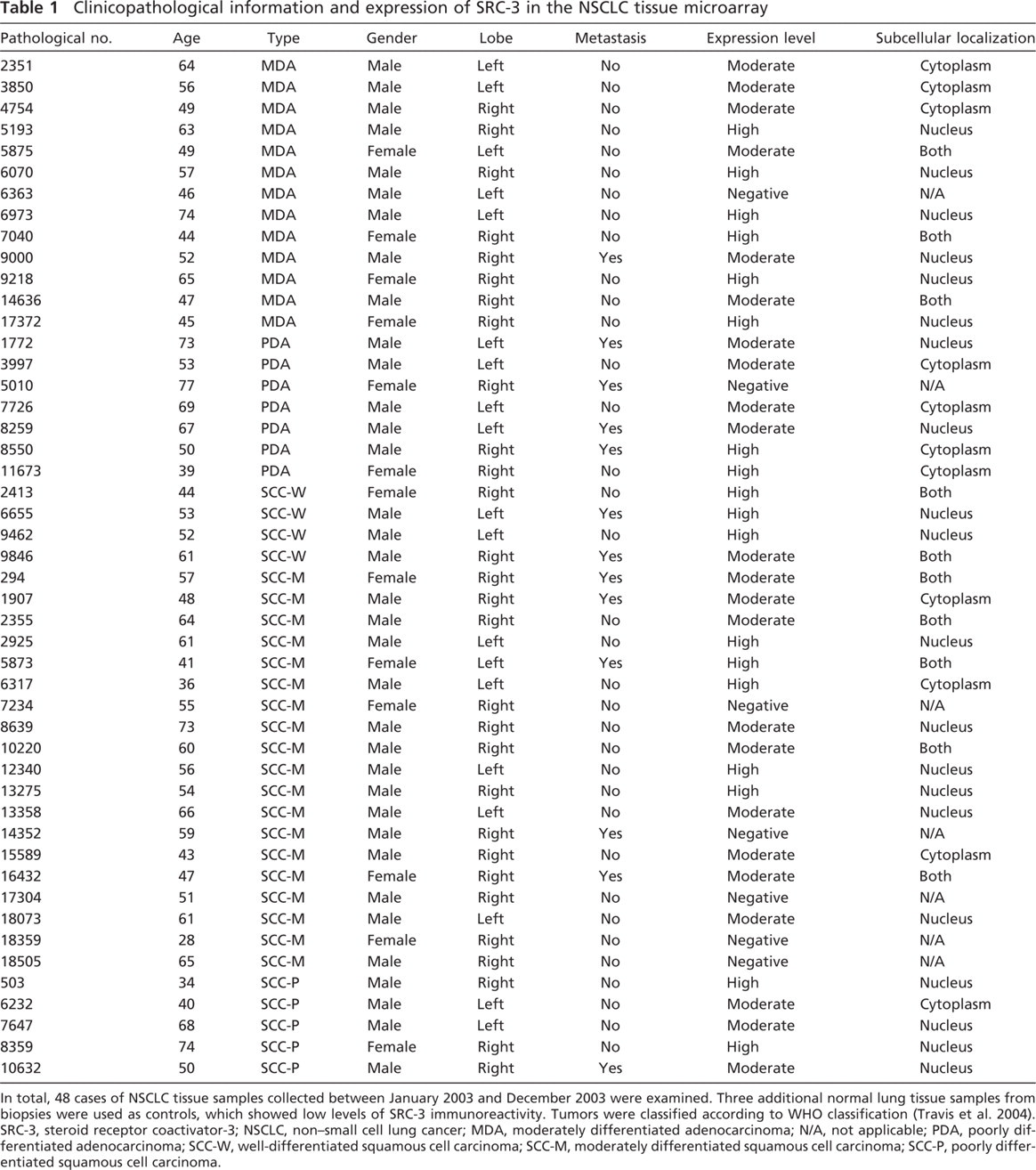
In total, 48 cases of NSCLC tissue samples collected between January 2003 and December 2003 were examined. Three additional normal lung tissue samples from biopsies were used as controls, which showed low levels of SRC-3 immunoreactivity. Tumors were classified according to WHO classification (Travis et al. 2004).
SRC-3, steroid receptor coactivator-3; NSCLC, nonsmall cell lung cancer; MDA, moderately differentiated adenocarcinoma; N/A, not applicable; PDA, poorly differentiated adenocarcinoma; SCC-W, well-differentiated squamous cell carcinoma; SCC-M, moderately differentiated squamous cell carcinoma; SCC-P, poorly differentiated squamous cell carcinoma.
In total, 48 cases of NSCLC tissue samples collected between January 2003 and December 2003 were examined. Three additional normal lung tissue samples from biopsies were used as controls, which showed low levels of SRC-3 immunoreactivity. Tumors were classified according to WHO classification (Travis et al. 2004). SRC-3, steroid receptor coactivator-3; NSCLC, non-small cell lung cancer; MDA, moderately differentiated adenocarcinoma; N/A, not applicable; PDA, poorly differentiated adenocarcinoma; SCC-W, well-differentiated squamous cell carcinoma; SCC-M, moderately differentiated squamous cell carcinoma; SCC-P, poorly differentiated squamous cell carcinoma.
Image and Data Analysisgraph
Images of SRC-3 immunostaining of the TMAs (n = 3) in each case were recorded with a digital camera (DP70; Leica)–equipped Olympus microscope (BX60; Olympus, Tokyo, Japan). The relative expression (RE) levels presented are the average levels recorded as part of a double-blinded study. Average levels of expression were calculated using an area ratio (AR) to represent relative positive area: AR = 0 means less than 5% positive area, AR = 1 means 6–25% positive area, AR = 2 means 26–50% positive area, AR = 3 means 51–75% positive area, and AR = 4 means more than 75% positive area. RE level was used to represent the immunostaining intensity of each sample: RE = 1, 2, or 3 means positive area was light-blue, blue, or black-blue, respectively. The final expression level was the sum of AR and RE: low level means AR + RE ≤ 2, moderate level means AR + RE = 3 or 4, and high level means AR + RE ≥ 5. Data analysis was carried out using the multinomial logistic regression and likelihood ratio test in the analytical software, SPSS 13.0 (Chicago, IL).
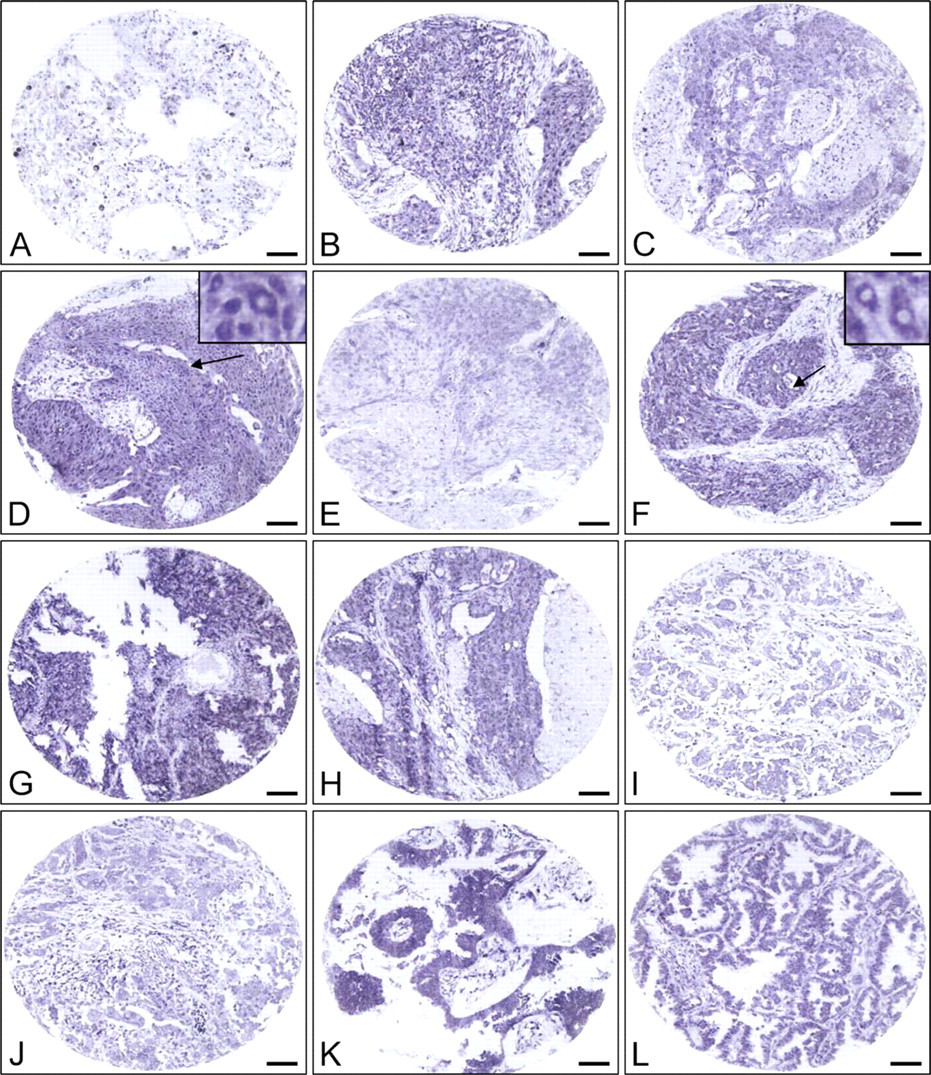
Steroid receptor coactivator-3 (SRC-3) expression levels in representative samples of control and non-small cell lung cancers. (
Results
Using nickel-intensified immunostaining, the final reaction product appears blue/black. We found that SRC-3-immunopositive materials were predominantly detected in the nucleus, but they were also detectable in the cytoplasm as shown in Figures 1D and 1F. The normal lung tissue control had weak SRC-3 immuno-reactivity (Figure 1A).
Of the 48 cases of NSCLC used in this study, over-expressed SRC-3 immunoreactivities were detected with different levels in most of the cases when compared with that of the control. For example, most of the well-differentiated SCC (SCC-W) exhibited high levels of SRC-3 immunoreactivities (Figures 1B and 1C), whereas most of the moderately differentiated SCC (SCC-M; Figures 1D and 1F) and poorly differentiated SCC (SCC-P) showed moderate expression levels (Figures 1G and 1H). These also occurred in moderately differentiated adenocarcinomas (MDAs) or poorly differentiated adenocarcinomas. In SCCs, the highest expression of SRC-3 was in SCC-M, whereas in the adenocarcinomas, the highest expression was in MDA.
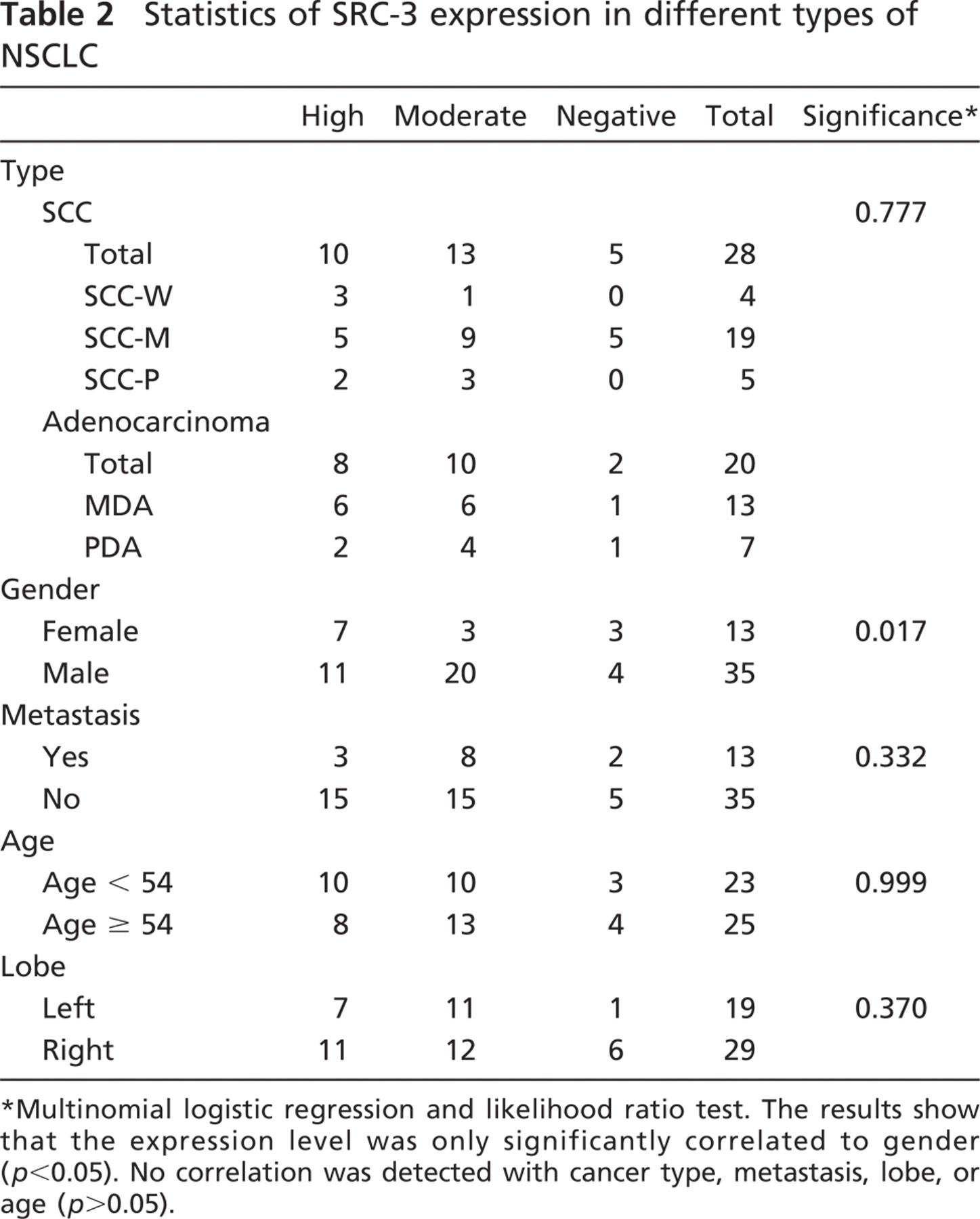
The frequency of SRC-3 overexpression in the 48 patients studied was 85.4%; it was 76.9% in women and 88.6% in men. More than half of the women but only about one third of men exhibited high levels of SRC-3 expression. Women tended to have high but men tended to have moderate expression levels of SRC-3 immunoreactivities. In most of the cases, no metastasis was detected, and nearly half of the non-metastatic cases also exhibited different levels of SRC-3, suggesting that the SRC-3 was overexpressed in lung cancer regardless of metastatic status. Different levels of SRC-3 immunoreactivities were also detected in different age groups (younger or older than 54 years) of lobes (left or right). Multinomial logistic regression and likelihood ratio test analysis showed that there was only a significant correlation between SRC-3 expression levels and gender (p = 0.017), as shown in Table 2.
Discussion
TMA studies of histopathological material have been frequently reported in the studies of malignant diseases. In this study, we report, for the first time, the SRC-3 immunoreactivity in NSCLC based on TMA. Among the cases examined, 85.4% showed different but overexpressed levels of SRC-3 immunoreactivity and the remaining 14.6% were negative, suggesting that high expression or overexpression of SRC-3 correlates with NSCLC.
Statistics of SRC-3 expression in different types of NSCLC
Multinomial logistic regression and likelihood ratio test. The results show that the expression level was only significantly correlated to gender (p < 0.05). No correlation was detected with cancer type, metastasis, lobe, or age (p > 0.05).
Our results further demonstrate that although SRC-3 immunoreactive materials are predominantly detected in the cell nuclei, SRC-3 is also detectable in the cytoplasm, consistent with what was stated by the antibody manufacturer, and the significance remains unclear. Nucleocytoplasmic shuttling of SRC-3 may be promoted by hormone treatment because similar results have been observed by studying other coactivators (Grenier et al. 2004); cells exhibiting cytoplasmic SRC-3 protein expression might not be exposed to local steroid hormone(s) or involved in the phase of any gene transcription at the time of tissue sampling. However, cytoplasmic SRC-3 might also imply a novel, non-genomic signaling pathway which is different from its classic genomic effect. Similar activity has been reported for many classic nuclear receptors (like ERα and ERβ) have an extra-nuclear component and exert their function through a secondary messenger cascade to rapidly activate protein kinase pathways and alter membrane electrical properties. Thus, the exact role of extranuclear SRC-1 in specific brain regions needs further investigation.
Our results also demonstrated that overexpression of SRC-3 immunoreactivity was more frequent in men than in women. Multinomial logistic regression and likelihood ratio test demonstrated significant correlations between the expression levels and gender. Our results suggest that metastasis is not correlated to the expression level of SRC-3; however, lower levels of SRC-3 immunoreactivity were more frequent in metastatic patients.
Gender differences in lung disease and cancer have been well established. For example, regardless of smoking habit, adenocarcinoma of the lung occurs more frequently in women than in men (Dougherty et al. 2006; Nose et al. 2009). In this study, we found that 46.2% (6/13) of female and 40% (14/35) of male patients suffered from adenocarcinoma. This suggests a higher occurrence of adenocarcinoma in female patients and an association between sex hormones and the development of these tumors. Also, we found that 53.8% (7/13) of female and 60% (21/35) of male patients suffered from SCC, suggesting a male predominance. Regardless of cancer type, SRC-3 immunoreactivity was found with a higher frequency in male patients than in female patients (88.6% vs 76.9%; 31/35 vs 10/13; p = 0.017). However, the underlying mechanisms currently remain unclear.
The etiology of NSCLC has not been fully defined, and understanding tumor characteristics may direct the development of a targeted treatment for this disease. Nuclear receptors have been extensively examined in SCLC and NSCLC (Ishibashi et al. 2005; Lu et al. 2006; Sommer et al. 2007; Ali et al. 2008; Hershberger et al. 2009; Raso et al. 2009; Zhang et al. 2009). It is well accepted that nuclear receptor coactivators play an important role in the modulation of transcriptional activity. Previous studies have shown that SRC-3 may be involved in the estrogen regulation of lung cancer (Marquez-Garban et al. 2007). Because SRC-3 over-expression was detected in NSCLCs, the role that SRC-3 plays in the carcinogenesis and mechanisms of NSCLCs require further investigation.
Footnotes
Acknowledgements
This work was supported by the Natural Science Foundation Project of Chongqing Science and Technology Commission (CQ CSTC, 2007BB5030) and by the Third Military Medical University (2007XG41) and in part by the National Natural Science Foundation of China (30772145).
The authors thank Dr. Yazhou Wu (Department of Health Statistics, Third Military Medical University, Chongqing, China) for assistance with statistical analysis and Robert Trieu (The University of Texas Health Science Center at Houston, Houston, TX) for proofreading this manuscript.