
Abstract
Trop-2, a transmembrane glycoprotein, has been identified in human epithelial cells as a contributor to tumor growth and unfavorable prognosis in breast cancer (BC). Our study aimed to assess the expression of Trop-2 protein via immunohistochemistry (IHC) and correlate it with clinicopathological features in early luminal-like BC. We conducted a cross-sectional study evaluating Trop-2 protein expression in tissue microarrays using IHC. The expression was evaluated by the H-score and the following categorization was used: H-Score 0 to <100 as low, H-Score 100 to 200 as intermediate, and H-Score >200 to 300 as high. The study included 84 patients with a median age of 57, of whom 70% had invasive ductal carcinomas, 75% were classified as T2, and 47.6% had no affected lymph nodes. Trop-2 expression was high in 56% of patients and intermediate in 38%. None of the patients had an H-Score of zero. No correlation was observed between Trop-2 expression and clinicopathological features, including age, histological subtype, grade, Ki67, tumor size, nodal status, lymphovascular invasion, tumor subtype, and pathological staging. We demonstrated that Trop-2 is highly expressed in early luminal-like BC and is not influenced by clinicopathological features.
Introduction
Human trophoblast cell-surface antigen 2 (Trop-2) is a transmembrane glycoprotein calcium signal transducer expressed in epithelial cells. Enriched expression of Trop-2 has been strongly associated with tumor growth and poor prognosis in solid epithelial tumors, including breast, lung, and gastric cancer.1–5
The development of specific antibody-drug conjugates (ADCs) targeting Trop-2 and their favorable outcomes in metastatic breast cancer (BC) have increased the need for research into this subject.6–11 Bardia and colleagues 12 have comprehensively evaluated the correlation between Trop-2 expression, response to Sacituzumab Govitecan (SG), and prognosis in metastatic triple-negative breast cancer (TNBC) patients. The intervention yielded positive results for all patients, and those with higher expression experienced improved outcomes. These findings contradict previous evidences linking high Trop-2 expression with adverse outcomes.1,2,12,13
The literature lacks comprehensive data on the relationship between Trop-2 and early luminal-like BC, and the expression of this biomarker in this patient’s subset needs further clarification. Our research objective is to investigate Trop-2 expression in early luminal-like BC and to correlate with clinicopathological features.
Methods
Patients and Eligibility Criteria
A cross-sectional study assessed Trop-2 protein expression through immunohistochemistry (IHC) in non-metastatic luminal-like BC patients. The study had a convenience sample size which consisted of all patients with early breast cancer who underwent upfront breast surgery between 2010-2015 at Hospital de Clínicas de Porto Alegre (HCPA), had tumors larger than 2 cm, and with available paraffin blocks to obtain material for tissue microarrays (TMAs) construction. A total of 242 patients were included. The patients’ hormonal receptor status, HER2 hyperexpression, and Ki67 were evaluated. The extracted specimens were used to build a tumor bank at HCPA and distributed among seven TMAs. The HCPA clinical records were thoroughly reviewed to collect clinical, pathological, and prognostic characteristics such as age, histological subtype, grade, Ki67, tumor size, nodal status, lymphovascular invasion, tumor subtype, and pathological staging. The Pathology Department of HCPA performed TMAs construction and immunohistochemistry staining.
The patient pool analyzed in this study exclusively comprises individuals diagnosed with early luminal-like breast cancer. Tumors deemed luminal-like exhibit over 1% of estrogen receptors (ER). Moreover, luminal-B tumors were characterized by the lack of progesterone receptor, grade 3, or their Ki67 score of 20% or higher. 14
Individuals with metastatic breast cancer, those with HER2 protein overexpression through IHC or HER2 gene amplification identified through FISH, those with inadequate material in the TMAs for IHC testing, and those lacking ER expression were not included in this study.
Ethics
The National Research Ethics Committee has approved this study at Plataforma Brasil, with CAEE number 53053221.7.0000.5327. It is important to note that according to national legislation, informed consent forms are not required for tissue blocks that have been conserved for at least 5 years as long as they are managed within ethical guidelines. Throughout this study, we strictly adhered to ethical principles when handling TMA samples. This includes maintaining patient confidentiality and avoiding any exposure of their data.
Tissue Microarray Specimen
Formalin-fixed paraffin-embedded tissue blocks were selected and thoroughly assessed for tissue microarray construction. With a precise HE staining process, the most representative areas were handcrafted into 3.0-mm tissue cores. We applied the manual TMA T-Sue system from Simport® Scientific in Beloeil, Canada. Our technique adhered to the one described by Kononen et al., 15 where two cylinders of every tumor were extracted from the original block (donor) and transferred to the TMA block (recipient). Placental core tissue was included in each TMA for spatial guidance.
Immunohistochemistry
To conduct the analysis of paraffin sections, the Benchmark ULTRA platform, manufactured by Ventana Medical Systems in Tucson, Arizona, was employed in conjunction with the EZ PREP solution. The antigens were retrieved by applying CC2 buffer (10 mM/L, pH 6) in a steamer at 95C for 60 min. After washing the slides with water, we employed Optiview Peroxidase Inhibitor, a 3% hydrogen peroxide solution, for 10 min to inhibit endogenous peroxidase activity. The primary antibody was incubated for 32 min in a humidified chamber at 36°C. We employed Optiview HRP Multimer to detect the reaction, using 3,3′-diaminobenzidine tetrahydrochloride hydrate (DAB). Hematoxylin counterstaining was performed, and a bluing reagent was applied before dehydrating, air-drying, and coverslipping the tissues. The Trop-2 Antibody (B-9) sc-376746 from Santa Cruz Biotechnology Inc. in Dallas, TX, USA, was utilized at an optimal dilution of 1:100 for IHC. To ensure accuracy, a highly expressed breast tumor was used as a positive control, and a negative control was obtained by omitting the primary antibody.13,16,17
Evaluation of Trop-2 Expression
The modified immunohistochemical score (H-score) was employed to determine Trop-2 expression levels on tumor cell membranes. This score considers staining intensity and the percentage of cells at that intensity. The H-score is calculated by numerically weighting the summation of percent staining: H-score = (3 × % cells with strong intensity staining) + (2 × % cells with moderate intensity staining) + (1 × % cells with mild intensity staining). The H-score scale ranges from 0 to 300, with specific Trop-2 expression categories assigned: Trop-2 low is classified as an H-score of 0 to <100, Trop-2 medium is an H-score of 100 to 200 and Trop-2 high is an H-score >200 to 300. The thresholds and reading scale were selected according to a previous study by Bardia et al., 12 which evaluated Trop-2 expression by IHC in triple-negative metastatic BC (Fig. 1).
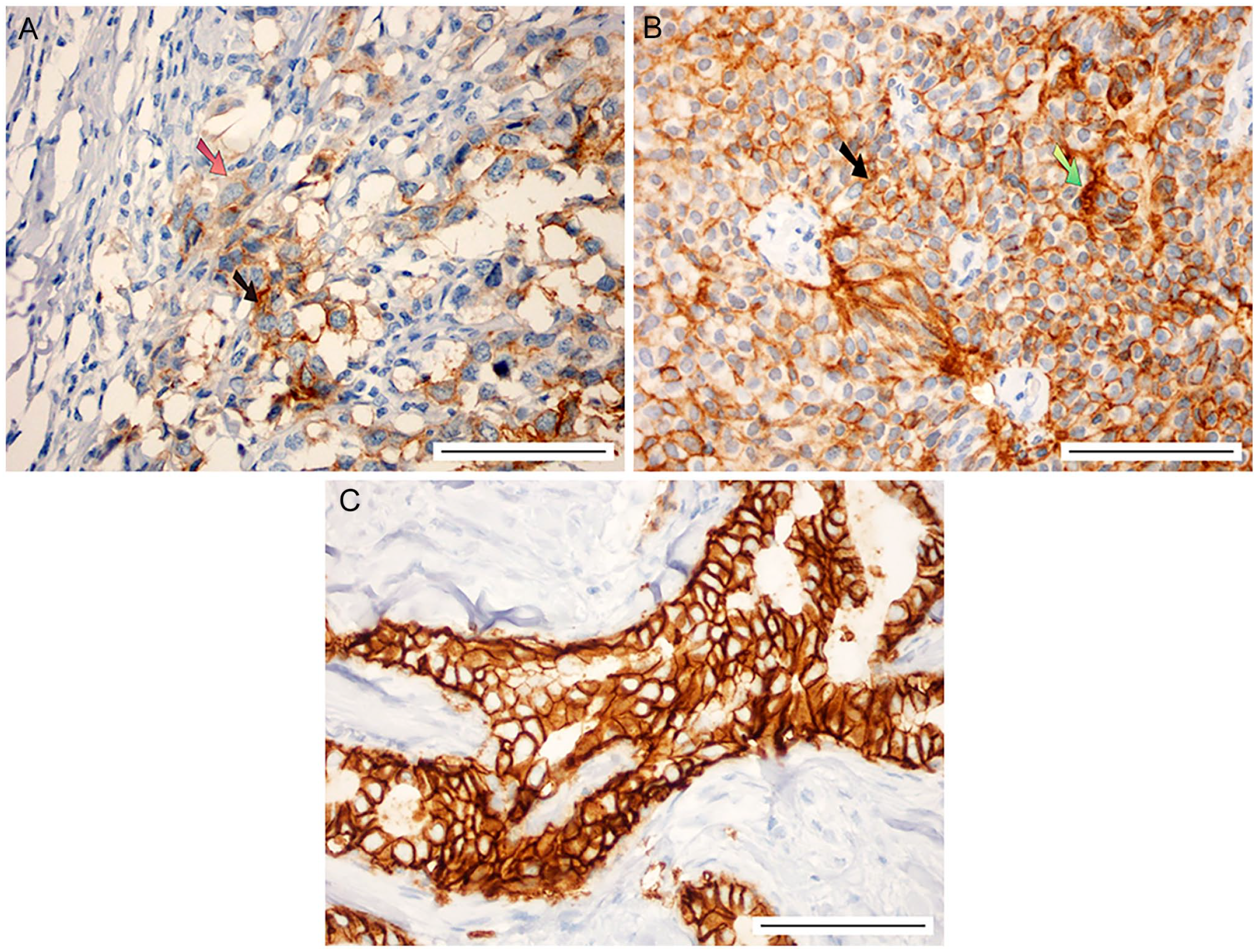
Representative images of Trop-2 staining intensity scores. Breast cancer samples were analyzed by immunohistochemistry using the Trop-2 Antibody (B-9): sc-376746 to detect membrane-associated Trop-2. (A) Weak (red arrow) and intermediate (black arrow) Trop-2 staining intensity. (B) Intermediate (black arrow) and strong (green arrow) Trop-2 staining intensity. (C) High Trop-2 staining intensity. Scale bars represent 100 µm.
The scoring and grading were carried out separately by M.S.G. and R.C.C., who were unaware of the clinical and histopathological information. To ensure the consistency and accuracy of the readings, 10% of the cases were randomly selected and evaluated by both evaluators. Cohen’s kappa index was 0.854, indicating a near-perfect agreement (p < .0001). In instances of disagreement, a consensus score was reached.
Statistical Analysis
The statistical analysis was conducted using SPSS version 29.0 from IBM Germany. The Trop-2 biomarker’s expression profile was presented in percentage and absolute frequency, considering the high, intermediate, and low expression scores. Chi-square and Fisher’s exact tests were used to compare Trop-2 expression with clinicopathological parameters. The interrater reliability was evaluated using Cohen’s kappa index. A p-value of ≤.05 was deemed statistically significant.
Results
The study enrolled a total of 84 patients (Fig. 2).
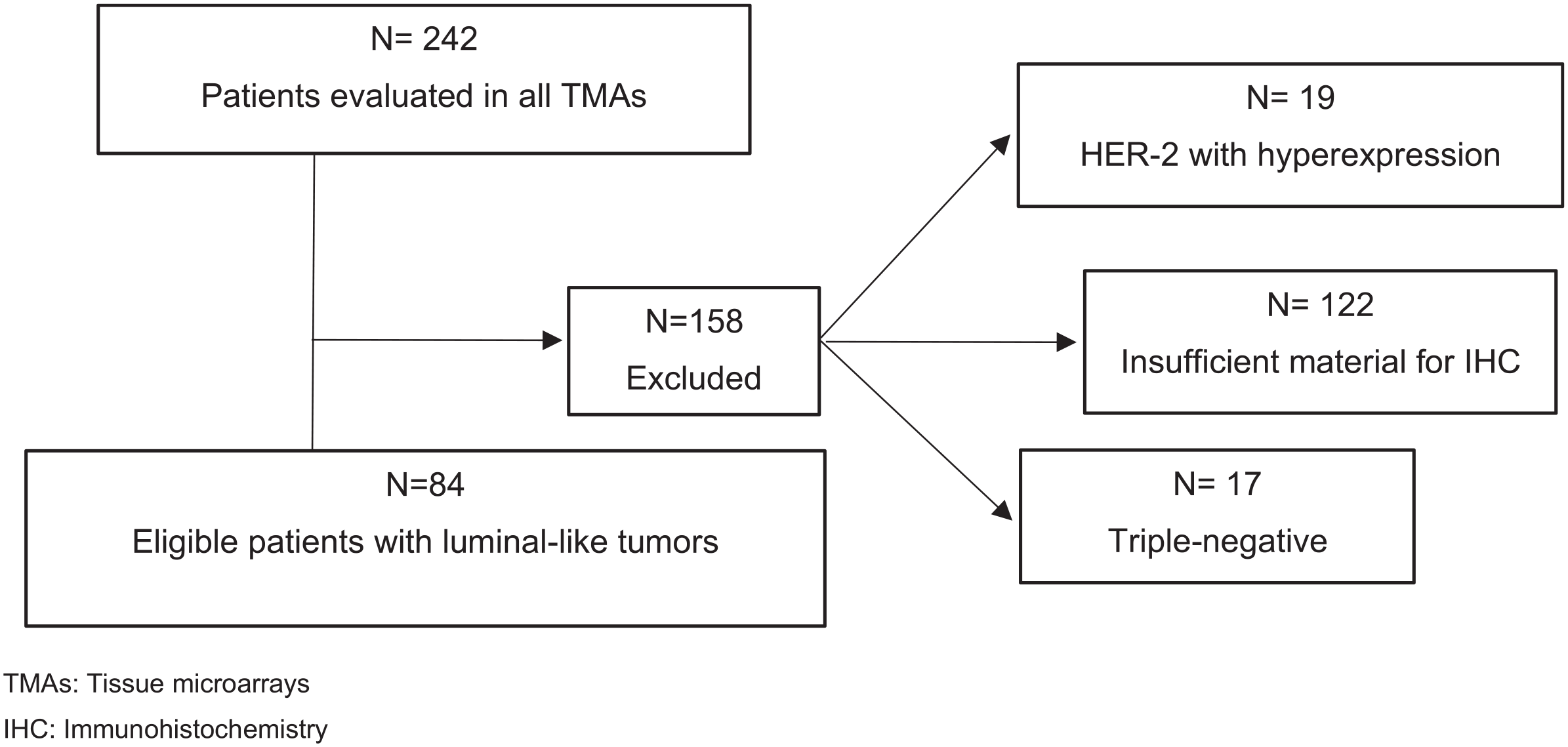
Flowchart showing eligible samples for Trop-2 expression analysis. Abbreviations: TMAs, tissue microarrays; IHC, immunohistochemistry.
Patients Baseline Characteristics
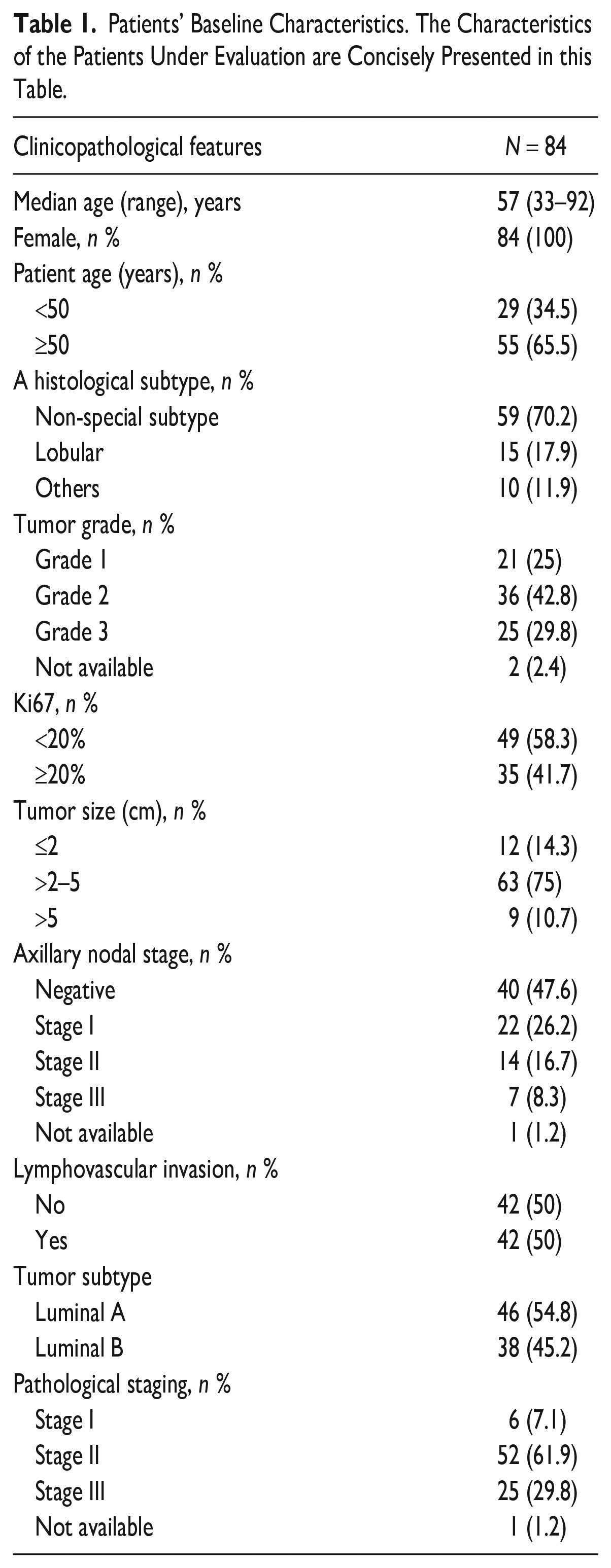
The median age was 57 years. Notably, 70% of the tumors were invasive ductal carcinomas, 75% were T2, and 47.6% were node-negative (Table 1).
Patients’ Baseline Characteristics. The Characteristics of the Patients Under Evaluation are Concisely Presented in this Table.
Trop-2 was Overexpressed in Early Luminal-Like BC
Figure 1 displays the IHC staining patterns of Ab-detected Trop-2. Cancer cell membranes showed the highest reactivity, while the cytoplasm exhibited fainter, mostly homogeneous reactivity. Trop-2 expression patterns were found to be heterogeneous in most breast tumor histotypes. According to the scoring criteria in the Methods section, samples were classified into Trop-2 high, Trop-2 medium, and Trop-2 low groups. Interestingly, more BC tissues were scored as Trop-2 high or intermediate (94%, 79/84) than low (6%, 5/84) (Fig. 3). None of the five samples with low expression had an H-score of 0, with values ranging from 30 to 80. Therefore, Trop-2 is highly expressed in early luminal-like BC. Moreover, seven patients (7%) had the highest Trop-2 score of 300.
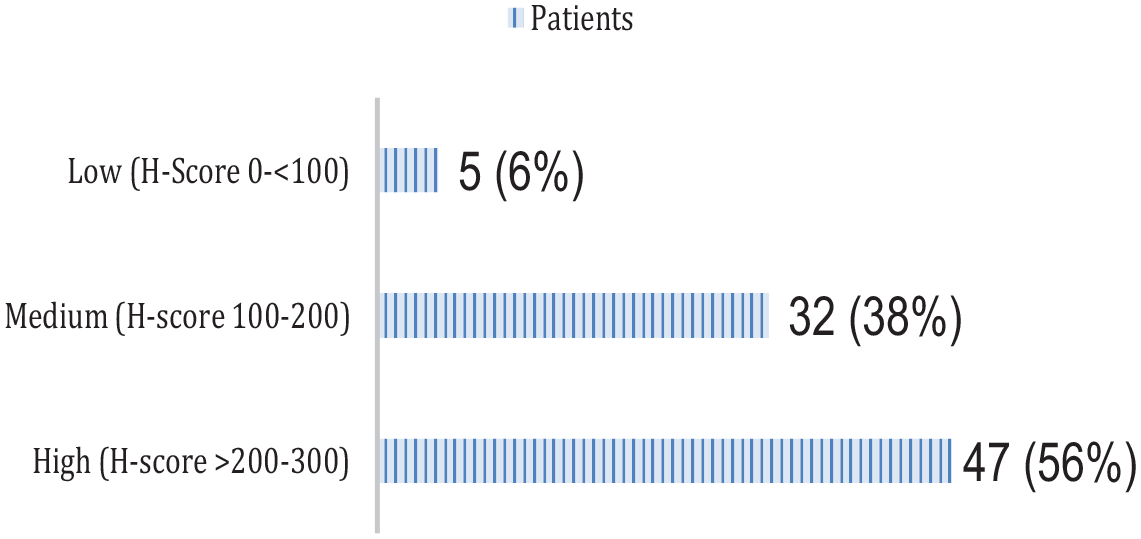
Trop-2 expression according to H-Score in TMA breast cancer samples. Most patients display a moderate to high level of Trop-2 expression, indicated by an H-Score of 100 to 300.
Correlation between Trop-2 Expression Level and Clinicopathological Characteristics
Based on our research, there is no significant variability in Trop-2 expression concerning various factors such as age, histological subtype, grade, Ki67, tumor size, nodal status, lymphovascular invasion, tumor subtype, and pathological staging. Our results have confirmed that the p-values associated with these factors were all greater than or equal to 0.290, indicating the absence of any substantial differences (Table 2).
Association among Baseline Characteristics and Trop-2 Expression. No Significant Correlation was Noted with Clinicopathological Characteristics.
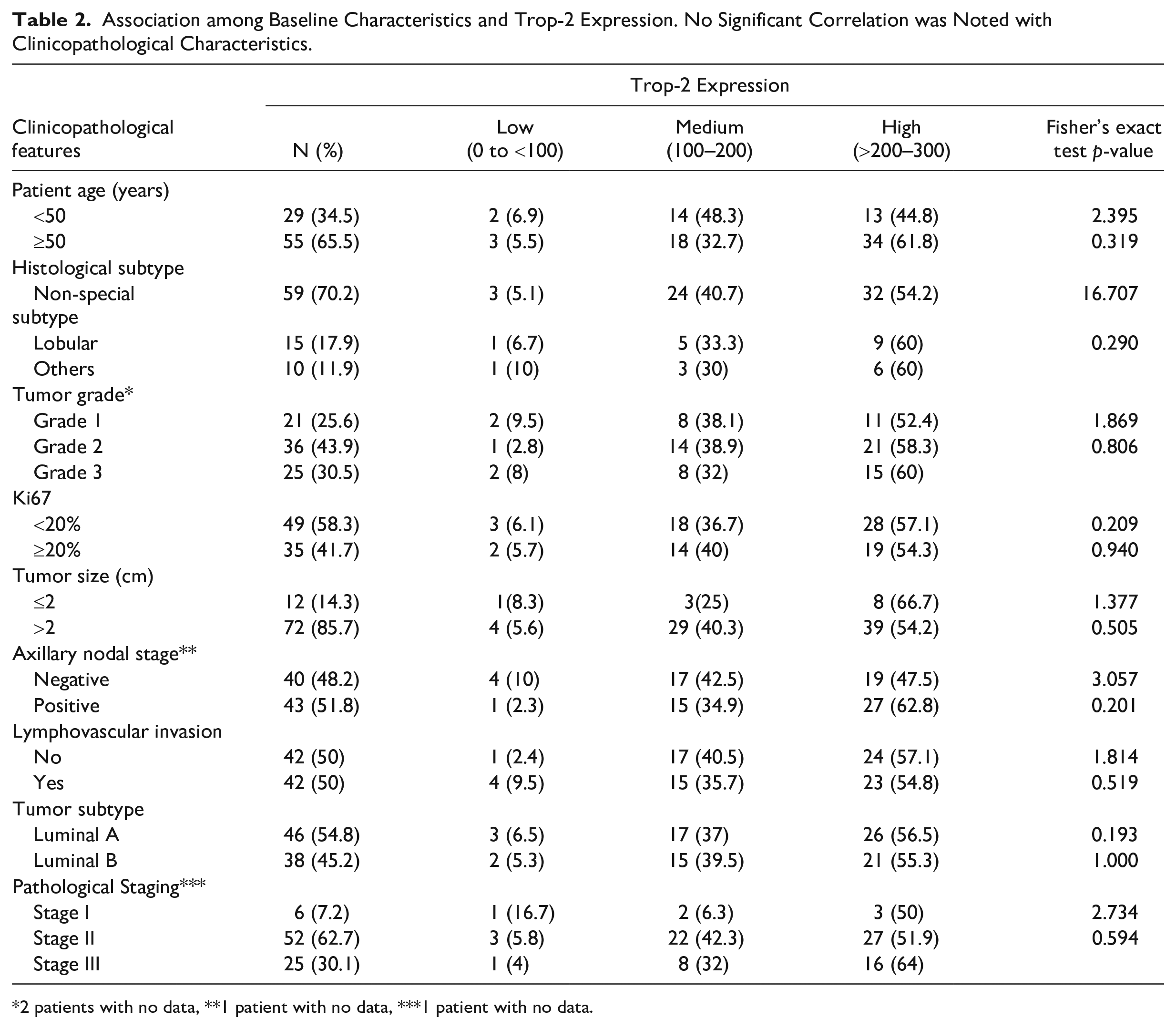
2 patients with no data, **1 patient with no data, ***1 patient with no data.
Discussion
To our best knowledge, this research is the first to show that Trop-2 is highly expressed by IHC in early luminal-like breast cancer, irrespective of clinical or pathological characteristics. This finding aligns with previous studies that have consistently demonstrated elevated levels of Trop-2 in metastatic BC.12,18 In the ASCENT trial, biomarker analyses in a TNBC cohort failed to establish any correlation between clinical outcomes and Trop-2 expression. 12 Vidula et al. researched Trop-2 gene expression in I-SPY 1, METABRIC, and TCGA datasets. In I-SPY 1, Trop-2 expression did not show significant differences in hormone receptor (HR) and HER2 status, intrinsic subtype, nodal involvement, menopausal status, grade, stage, presence of lymphovascular invasion, or age. Furthermore, in METABRIC, TACSTD2 gene expression was not significantly associated with age, menopausal status, nodal involvement, or stage. The researchers have demonstrated that the expression of TACSTD2 was not predictive of treatment response in I-SPY 1 or future outcomes in I-SPY 1 and METABRIC. 18
There is an ongoing debate regarding the role of Trop-2 in BC. Although some studies have not found any prognostic effect, other evidences suggest that it may function as a negative prognostic factor and act as an oncogene, promoting tumor growth, stem cell proliferation, and metastasis.1,2,13 The study conducted by Aslan and colleagues provides evidence that the levels of Trop-2 protein play a significant role in the development of TNBC tumors. 13 Ambrogi et al. 1 found that patients with elevated levels of membrane-associated Trop-2 have poorer outcomes. To gain a deeper understanding of the factors underlying the disparities in the clinical implications and prognostic outcomes observed in diverse studies, additional research is needed. The discrepancies could be due to a variety of factors, including differences in patient populations, a lack of standardized treatment options targeting Trop-2, short periods of follow-up, or varying methods of evaluating Trop-2.
The study has limitations due to the small sample size and the lack of follow-up data on clinical outcomes.
The assessment of a patients’ subset commonly encountered in clinical oncology has yielded significant findings that have not been extensively studied in the literature. Moreover, our results have been evaluated by two well-trained readers, achieving an exceptional level of agreement, strengthening the findings.
Trop-2 is highly expressed in early luminal-like BC independent of clinicopathological features. Due to its extensive presence in tumor samples, there is a strong rationale for further research investigating the use of anti-Trop-2 ADCs in this clinical setting.
Conclusion
Trop-2 is highly expressed in early luminal-like breast cancer and is not influenced by clinicopathological features.
Footnotes
Acknowledgements
We acknowledge and emphasize the essential contributions made by Gabriela Remonatto and Emily Ferreira Salles Pilar in the methodology and execution of immunohistochemistry. Moreover, we cannot overlook the crucial role played by Vania Hirakata in providing statistical support.
Competing Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All the authors participated in the writing and review of the article. R.C.C. played a role in planning, executing, analyzing, and interpreting the data. R.D.R. contributed to planning, executing, and interpreting the data. M.S.G. oversaw the planning, execution, analysis and interpretation of the data.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the funding for research of Hospital de Clínicas de Porto Alegre (HCPA).